Don't Lose Heart
Catch Your Breath
An Ounce of Prevention
Breaking Bad Cells
Faculty Fun Facts
100
Three determinants of stroke volume
Preload
Contractility
Afterload
100
Indication for antibiotics in AECOPD
Purulent sputum +1:
increase in sputum volume or dyspnea
2025 GOLD Report recommends antibiotics in following scenarios:
•3 cardinal symptoms present (dyspnea, ↑ sputum volume, ↑ purulence)
•2 of the cardinal symptoms presents, if ↑ sputum purulence is one of them
•Requiring mechanical ventilation
100
USPSTF recommendation for lung cancer screening
50-80 years of age with
>20 pack-year smoking history and
currently smoking or quit within the last 15 years
100
Classic chem panel findings in TLS
and
Pharmacotherapy for prevention of hyperuricemia
Hyperkalemia, hypocalcemia, hyperphosphatemia
Allopurinol
100
Dr. Juakiem endoscopically removed a stone swallowed by this zoo animal
Dolphin
200
Categorize the shock:
CO 2.0, SVR 1400, SV 18, PCWP 22, CVP 15
Cardiogenic
[low CO, high PCWP and CVP, low SV, high SVR]
200
Estimate arterial pH and pCO2
based on this VBG: pH 7.29, pCO2 58, HCO3- 24
ABG: pH 7.34 (add 0.05), pCO2 53 (-5)
200
Most effective first-line pharmacotherapy for smoking cessation
Varenicline (Chantix)
or combination NRT (patches and lozenges/gum)
200
Potential issue with prolonged use of calcitonin in management of acute hypercalcemia
Tachyphylaxis after 48 hours
(due to receptor down-regulation)
200
Names of Roe's cats
Frank and Jack
300
Stabilize the shock:
CO 10.4, PCWP 12, CVP 6, SVR 364, SV 82
Fluids and pressors
[distributive shock; also need to treat underlying]
300
Indication for addition of inhaled corticosteroids to maintenance regimen in COPD
absolute eos >300
(can consider for eos 100-300)
300
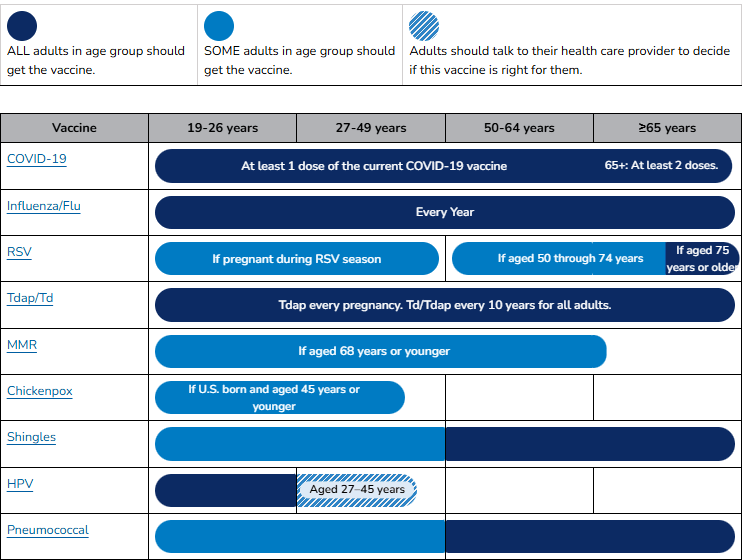
CDC recommends addition of these two immunizations at age 50 for all average risk individuals
(in addition to those recommended at younger ages)
Pneumococcal
Shingrix
300
Deficient enzyme and treatment for TTP
ADAMTS 13 (cleaves vWF)
Steroids + PLEX (plasmapheresis)
300
Former aerospace engineer
Bert Patino
(interventional cardiologist)
400
Treat the shock:
CO 2.1, SVR 1500, CVP 15, PCWP 4, SV 18
Alleviate obstruction
(etiology-specific: e.g. pericardiocentesis, needle decompression, thrombectomy)
[Obstruction -> impaired filling -> high CVP, low PCWP, low CO, low SV, high SVR]
400
Broadly speaking, what kind of blood gas would be concerning for impending respiratory collapse in a patient presenting with severe asthma exacerbation?
Normal
[While patients are able to compensate, pCO2 would be low in the setting of hyperventilation (respiratory alkalosis). As they fatigue, pCO2 will begin to climb, and the blood gas can look normal.]
400
For a patient with T-score (-1.0 to -2.5) and no other risk factors, what scores (specifically) would be an indication to start treatment to reduce the 10-year risk of hip and major osteoporotic fractures, respectively?
FRAX >3% (hip)
FRAX >20% (major osteoporotic)
400
Likely diagnosis for patient short of breath, new cough, and these exam findings:

Thoracic central venous obstruction
(accept SVC syndrome)
400
Dr. Wood's (infectious disease) hobby related to microbiology
Vinting
(accept home brewing)
500
Empirically treat the shock:
CO 2.3, PCWP 22, CVP 18, SV 50
BP 82/68, Temp 92.6, RR 8
IV levothyroxine, IV triiodothyronine, IV hydrocortisone
(myxedema coma: bradycardia and impaired contractility -> lower SV and CO; high PCWP and CVP; high SVR)
500
Vent finding and management (as far as changing vent settings)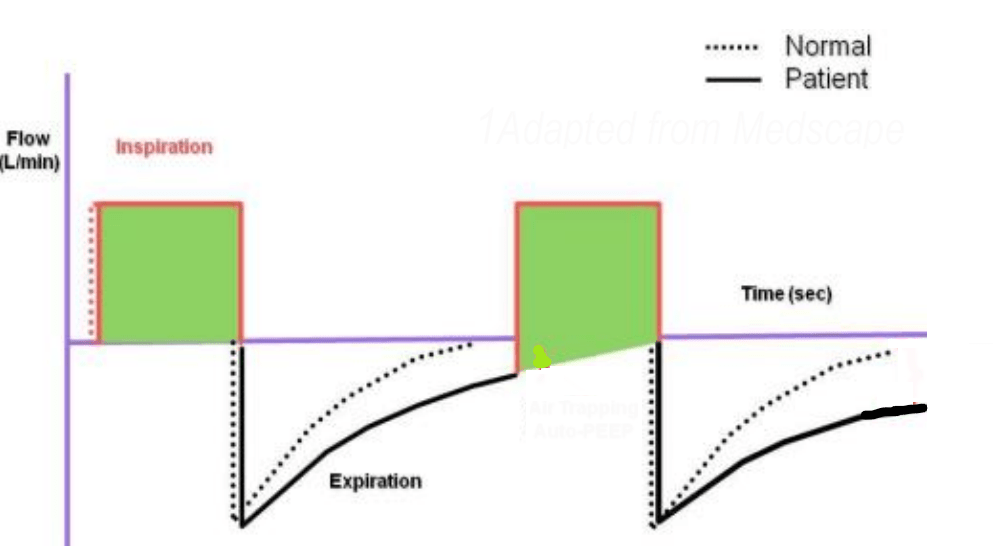
Auto-PEEP
Increase expiratory time
[accept reduce I:E ratio]
500
AGA/ACG indication for upper endoscopy screening for Barrett's
Chronic GERD + at least 3:
Age > 50, male, white, obese, hiatal hernia, nocturnal reflux, current/prior tobacco use, first-degree relative with Barrett's or esophageal adenocarcinoma
500
Indications for empiric gram positive coverage in a patient with neutropenic fever (name 3)
Severe sepsis (hemodynamic instability)
Pneumonia
BCx + for gram positive bacteria
Suspected CLABSI
Skin/soft tissue infection
Known MRSA colonization
500
Previously drove a locomotive for the USAF
Call sign as "Popeye"
Dr. Pizzino (Nephro)