Basics
NIMO
Physical Exam
Path 1
Path 2
100
What is considered the dynamic stabilizers of the shoulder joint?
The Rotator Cuff Muscles
100
NIMO: Deltoid
N: C5-6 Upper Trunk, Posterior Cord, Axillary Nerve
I: Humerus
M: Shoulder Abduction >15*, Flexion, Extension, External Rotation
O: Clavicle, Acromion, Spine of Scapula
100
Passively bringing the patient's arm into 90 degrees of forward flexion and their elbow flexed to 90 degrees. The examiner then horizontally adducts the flexed arm across the patient's body, bringing the elbow toward the contralateral shoulder
Scarf Test or Cross-Body Adduction Test
This position results in compression of the medial acromial facet against the distal clavicle to provoke symptoms at the acromioclavicular joint.
100
What type of exercises would you recommend for a patient that has a history of repeated shoulder dislocations?
Isometric Strengthening Program
100
What 2 movements are the first to be restricted in patients with adhesive capsulitis?
Abduction
External Rotation
200
What are the 3 static stabilizers of the shoulder joint?
Superior, Middle, and Inferior Glenohumeral Ligaments. The inferior GH Ligament is the most critical ligament in preventing anterior translation of the humerus on the glenoid.
200
NIMO: Infraspinatus
N: Suprascapular Nerve (C5 & C6)
I: Greater Tuberosity of the Humerus
M: External Rotation
O: Infraspinatus Fossa of the Scapula
200
The patient's arm should be elevated to 90 degrees in the scapular plane, with the elbow extended, full internal rotation, and pronation of the forearm. This results in a thumbs-down position as if the patient were pouring liquid out of a can. The physician should stabilize the shoulder while applying a downwardly directed force to the arm, the patient tries to resist this motion. This test is considered positive if the patient experiences pain or weakness with resistance.
Empty Can Test is used to assess the supraspinatus muscle and supraspinatus tendon
200
Where is the weakness in a patient with Lateral Scapular Winging?
Trapezius is weak
200
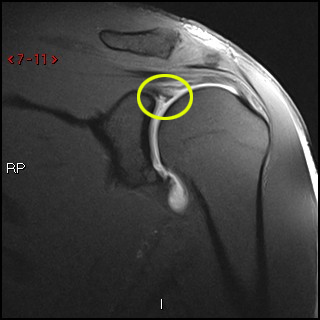
What is the defect in a Hill-Sachs Lesion?
Posterolateral humeral head compression Fracture
![]()
Hill Sachs lesion (black arrow) seen as a cortical depression of the postero-superior aspect of the humeral head. This depression is located medial to the head-neck junction (arrowhead). A Bankart lesion (fracture of the antero-inferior aspect of the glenoid rim) is also seen (white arrow).
300
TUBS is a mnemonic. What pathology is it used for and what does it stand for?
Traumatic Shoulder Dislocation Mgmt
Traumatic
Unidirectional, unilateral
Bankhart lesions co-exist
Surgery
vs AMBRI (Atraumatic, Multidirectional Instability, Bilateral, Rehab, Inferior capsular Shift)
300
NIMO: Teres Minor
N: Axillary nerve from the posterior cord, Upper Trunk, to C5 & C6 Roots
I: Greater Tuberosity of the Humerus
M: External Rotation (+Assists with Adduction and Extension)
O: Upper two-thirds of the lateral border of the scapula
300
While stabilizing the patient’s scapula with one hand and holding the affected arm at 90° abduction and internal rotation, the examiner grasps the elbow and axially loads the humerus in a proximal direction. The arm is moved horizontally across the body. A positive result is indicated by a sudden clunk.
Jerk Test used to detect posteroinferior instability of the Glenohumeral joint.
A positive result is indicated by a sudden clunk as the humeral head slides off the back of the glenoid. When the arm is returned to the original position, a second jerk may be observed, that of the humeral head returning to the glenoid.
+Kim Test
300
What population of patients would you suspect a Humeral stress Fracture?
How long before your patient can return to play?
Pitchers, Throwers (Due to repetitive overuse)
8-12 weeks --> May gradually return and increase activity after it is healed
300
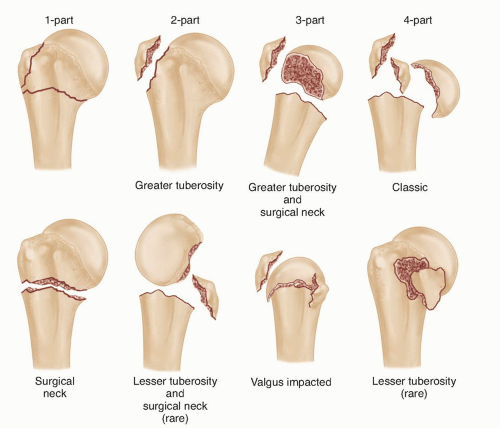
What system is used when classifying proximal humerus fractures and what are the anatomical parts used in this system?
Four-Part Fracture System
Humeral Head, Greater Tuberosity, Lesser Tuberosity, Humeral Shaft
400
What imaging would you order to prove a labral tear exists?
MR Arthrogram: dye will flow into the labral defect and show up white on images.
400
NIMO: Pectoralis Major
N: C5-T1, all 3 trunks, Medial & Lateral Cords, Medial & Lateral Pectoral Nerves
I: Greater Tubercle of the humerus
M: Shoulder Adduction, Flexion
O: Clavicular head – originates from the anterior surface of the medial half of clavicle.
Sternocostal head – is the larger of the two heads and originates from: The anterior surface of sternum, anterior surface of the superior six costal cartilages, Superior part of the aponeurosis of external oblique muscle.
400
The upper extremity to be tested is placed in 90° of shoulder flexion and 10-15° of horizontal adduction. The patient then fully internally rotates the shoulder and pronates the elbow. The examiner provides a distal stabilizing force as the patient is instructed to apply an upward force. The procedure is then repeated in a neutral shoulder and forearm position. A positive test occurs with pain reproduction or clicking in the shoulder with the first position and reduced/absent with the second position.
O'Brien's Active Compression Test is to indicate potential labral (SLAP Lesion) or acromioclavicular lesions as cause for shoulder pain.
Depth of symptoms must also be assessed as superficial pain can indicate acromioclavicular joint symptoms and deep pain is more often a sign of a labral lesion
+Crank Test, Anterior Apprehension and one of either Biceps Load II, Speed's, or Yergerson's for SLAP lesions.
400
You identify AVN in the humeral head on a radiograph of a patient complaining over shoulder pain. What information is important to obtain in this patient’s medical history?
Prior trauma due to potential for Proximal humeral fracture involving the anatomic neck due to potential damage to the posterior circumflex artery.
400
What exercises would you recommend for a young pitcher with subacromial impingement syndrome?
Progressive Resisted Eccentric Internal Rotation, that focus on RC muscles and scapular stabilizers, with progression to sports-specific activities.
500
What acromion morphology (Type 1, 2, or 3) is more highly associated with RC Tears?
Type 3 is more highly associated with RC Tears
Type 1 is flat, Type 2 is curved, Type 3 is hooked.

500
NIMO: Triceps
N: C6-C8, 3 trunks, Posterior Cord, Radial nerve
I: Posterior surface of the olecranon process of the ulna, capsule of the elbow joint, and antebrachial fascia
M: Shoulder & Elbow Extension
O: Long Head - Infraglenoid tubercle of the scapula
Lateral Head - Posterior aspect of the humerus, superior to the radial groove
Medial Head - Posterior aspect of humerus, inferior to the radial groove
500
Patient is sitting upright with the arm flexed to 90°, the examiner stands adjacent to the affected shoulder forearm holding the flexed elbow or forearm. [1] Joint load is applied along the axis of the humerus with one hand while the other hand performs humeral rotation while the shoulder is being elevated in the scapular plane. The test can be repeated in supine. A positive test is indicated during the maneuver (usually during external rotation) if there is reproduction of symptoms (usually pain) with or without a click.
Crank Test is used to identify glenoid labral tears and assess an unstable superior labral anterior-posterior (SLAP) lesions.
500
The patient presents with an abnormal EMG after a proximal humeral fracture. What Motor and Sensory deficits do you expect to see on physical exam?
Proximal humeral fractures most commonly occur at the surgical neck.
Axillary Nerve is prone to injury at this site.
Impaired Abduction and external Rotation due to Deltoid and Teres Minor Involvement
Impaired Sensation over the lateral shoulder and arm due to Upper Lateral Cutaneous Nerve of the Arm involvement.
500
What injuries are associated with a Type 4 AC Joint Separation?
Complete AC Tear, Complete CC = clavicle floats upward & posteriorly over the acromion. Patient requires surgery
