Etiology
Pathogenesis
Diagnostics
Presentation and Treatment
Complications
100
What is the most common risk factor for aortic dissection and what demographic is most associated with aortic aneurysm and dissection?
Hypertension, Males 60 years and older
100
What layer of the aortic wall ruptures initially in the pathogenesis of an aortic dissection?
Tunica intima
100
What is the first step in diagnosing aortic dissection?
EKG and Labs (Double points: What sensitive lab test could have been ordered in our case but was not?)
100
True or False: The first line treatment for a Stanford Type B dissection is surgery.
False
100
Shock-like symptoms are caused by what complication of aortic dissection?
Aortic wall rupture -> acute blood loss
200
List the genetic conditions associated with aortic dissection.
Marfan syndrome
Ehlers-Danlos syndrome
Turner syndrome
Bicuspid aortic valve
Coarctation of the aorta
200
What is the most common classification of aortic dissection?
Stanford A
200
True or False: Widened mediastinum on CXR is a definitive imaging finding in diagnosing aortic dissection.
False
200
Outside chest and back pain, what are some features that may raise suspicion of aortic dissection? (4 features)
Neck/truncal pain
Neurological symptoms (stroke-like symptoms, limb weakness, paresthesia)
Syncope
Acute limb ischemia
200
Spinal artery occlusion as a result of aortic dissection leads to what major complication?
Paraplegia (lower extremity paralysis)
300
Cocaine and amphetamines are known to increase risk of aortic dissection. What impact do these substances have on the body that cause this increased risk?
Increased arterial pressure, increased heart rate
300
What are the three most common sties for aortic dissection?
Above aortic root
Aortic arch
Distal to left subclavian artery
(Double points: Why?)
300
What are the Stanford and Debakey classifications of this aortic dissection?

Stanford Type B, Debakey Type III
300
How should hypotensive aortic dissection patients be medically treated?
IV fluids, vasopressor support if fluids do not treat hypotension
300
What are common complications of a Stanford Type A aortic dissection that propagates proximally?
Myocardial infarction
Aortic regurgitation
Pericarditis, Cardiac tamponade
Stroke (moreso distally than proximal)
400
Tertiary syphilis can disrupt a structure related to the aorta, increasing the risk of aortic aneurysm and dissection. What is this structure called?
Vasa vasorum
400
As the false lumen grows and propagates down or up the aorta, in which layer(s) of the aortic wall can a new rupture form?
Intima (reentry into true lumen)
Full aortic wall (rupture and acute blood loss)
400
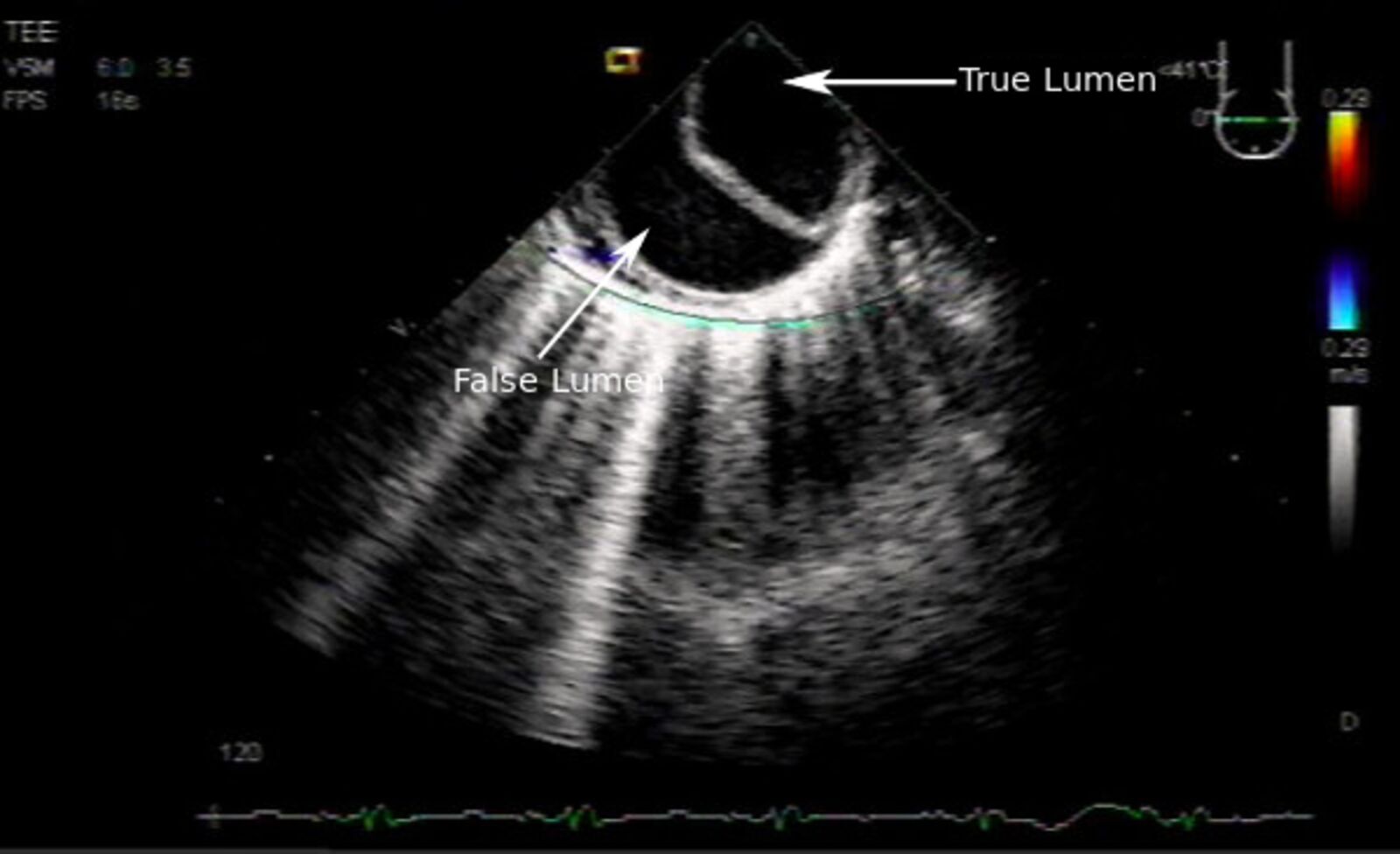
What are we looking at here? (View+point out features)

Transesophageal echocardiogram, descending aorta
400
A patient has tearing pain in the chest, neck, and jaw. Limbs had asymmetrical blood pressure readings with the right arm being normal and left being markedly low. EKG shows normal findings. You suspect an aortic dissection. Where is the most likely location of the dissection?
Aortic arch (Double points: What are the Stanford and Debakey classification for this dissection?)
400
What are major concerns about undergoing reperfusion therapy in Rodney's severe rhabdomyolysis?
Reperfusion injury due to generation of free radicals
Acute compartment syndrome due to edema from reperfusion
500
Which form of Ehlers-Danlos Syndrome is indicated as a risk factor for aortic dissection and what type of collagen is affected?
Vascular EDS, Type III Collagen
500
What happens in cystic medial degeneration on a histopathological level? (3 main features)
Mucoid extracellular matrix accumulation
Thinning, fragmentation, and disorganization of elastin fibers
Loss of smooth muscle nuclei
500
A patient's EKG presents with peak T waves, discernible but small P waves, and narrow QRS complexes. What is the most likely range of the patient's serum K+ levels given the patient had rapid-onset hyperkalemia?
5.5-6.4 mEq/L
500
What are the goals in medical therapy for aortic dissection and what medications are used?
Pain relief, maintain SBP of 100-120 mmHg, maintain HR ~60 bpm
Morphine, IV beta blocker (esmolol, labetalol), vasodilator (nitroprusside, nicardipine)
CCBs if beta blocker's contraindicated (verapamil, diltiazem) (Double points: Why would beta blockers be contraindicated in Rodney's case?)
500
What was the cause of Rodney's abnormal lab values (elevated potassium, amylase, creatinine, creatine kinase, blood lactate; decreased bicarbonate; high anion gap)?
End-organ damage and rhabdomyolysis
Potassium: Muscle breakdown
Amylase: Hypoperfusion to pancreas
Creatinine: Hypoperfusion to kidneys and myoglobin build up from muscle breakdown -> acute kidney injury
Creatine kinase: Leg muscle breakdown and death
Lactate: Hypoperfusion and tissue ischemia