Did you hear that?
Is that a face?
What is that?
Did You say mouth?
What about the neck?
100
What are the most common organisms that cause acute otitis media ?
•Typically viral
RSV, Influenza virus, Rhinovirus, and Enterovirus
•Bacterial causes
•S. pneumoniae (35% of cases)
•H. influenzae (nontypable strains)
•M. catarrhalis
100
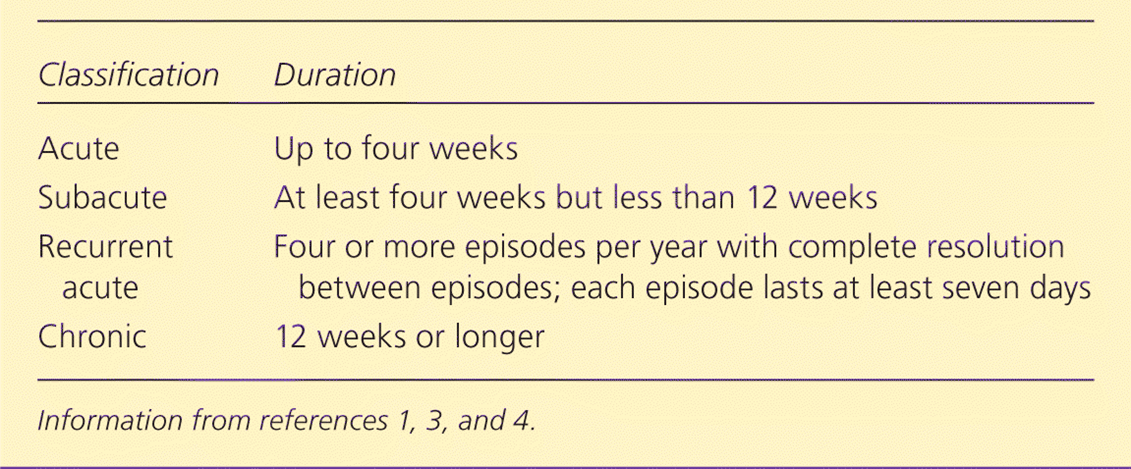
What is sinusitis? what are its different classification?
•Inflammation of one or more of the paranasal sinuses (frontal, sphenoid, ethmoid, maxillary)
100
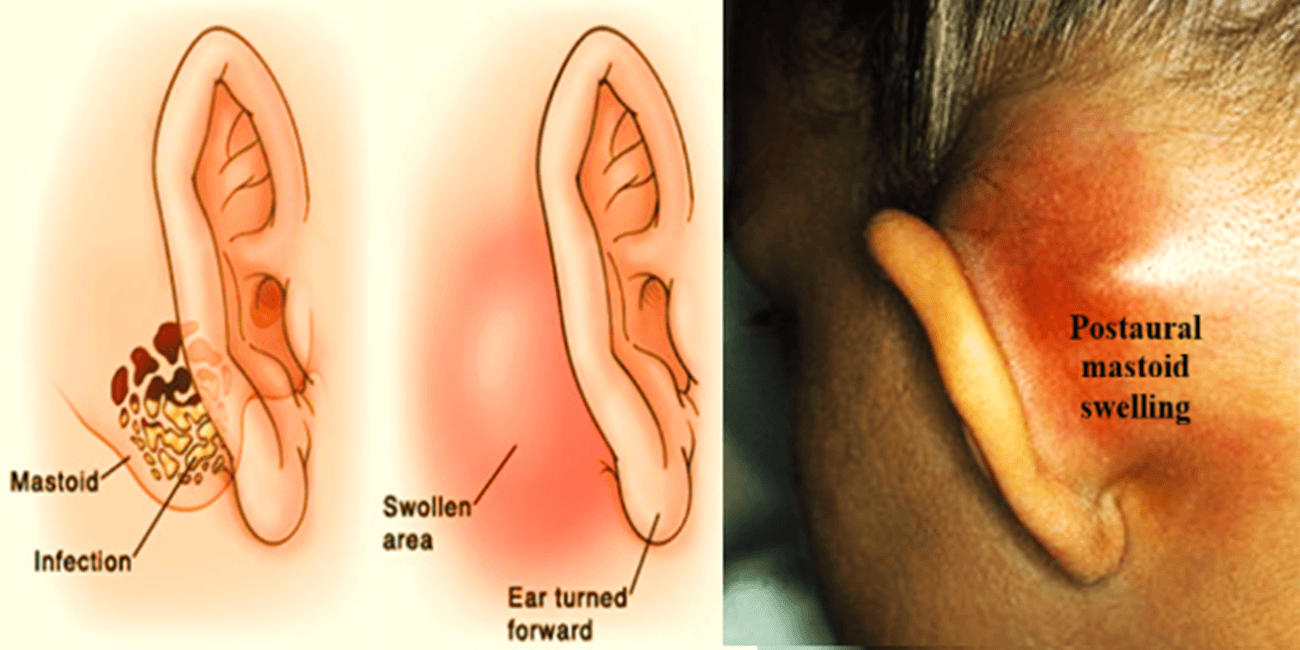
What is the diagnosis?

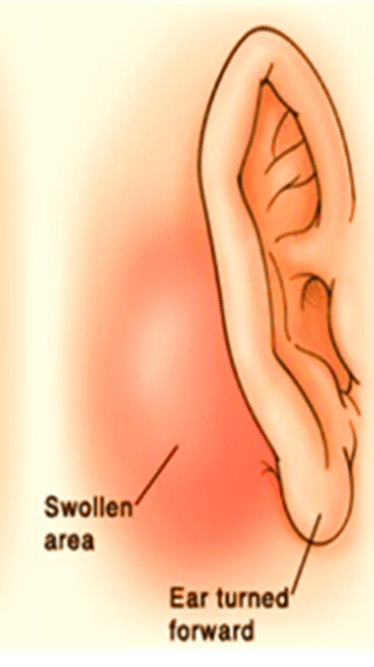
mastoditis
100
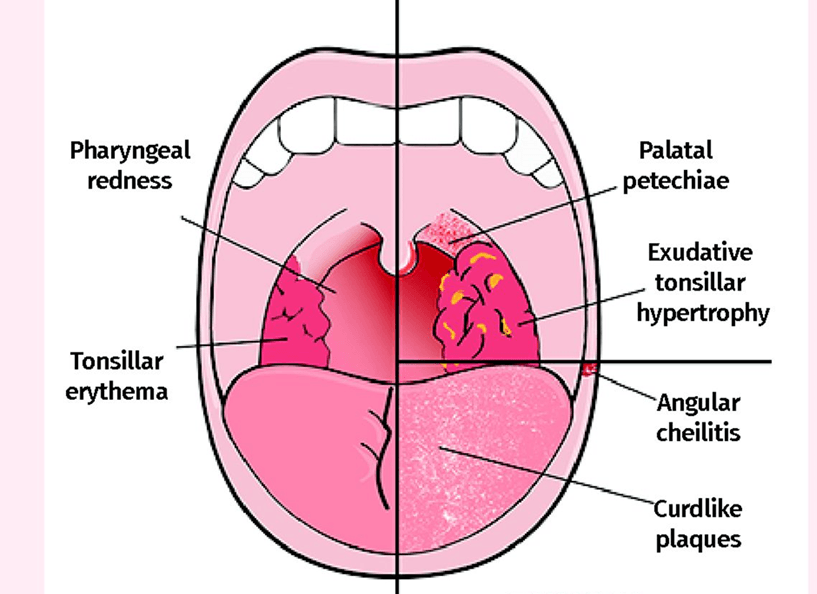
What is the diagnosis?
Pharyngitis
100
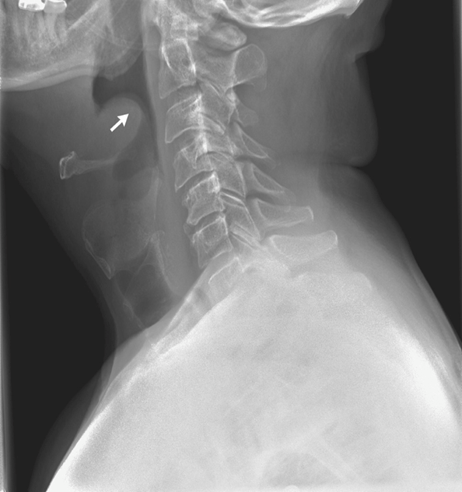
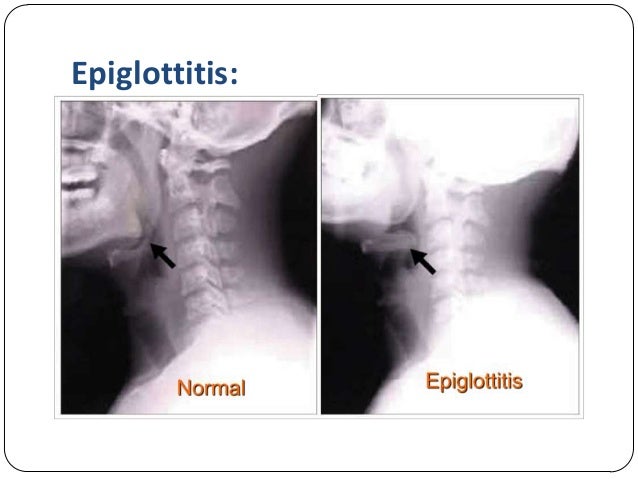
What diagnosis does this picture make you think of?
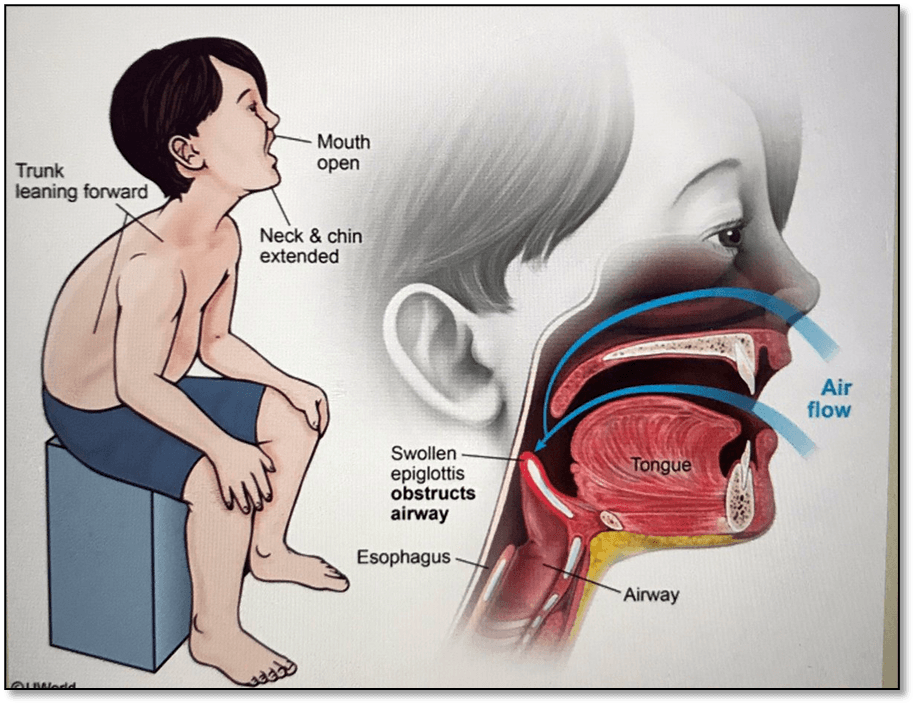
Epiglottitis
200
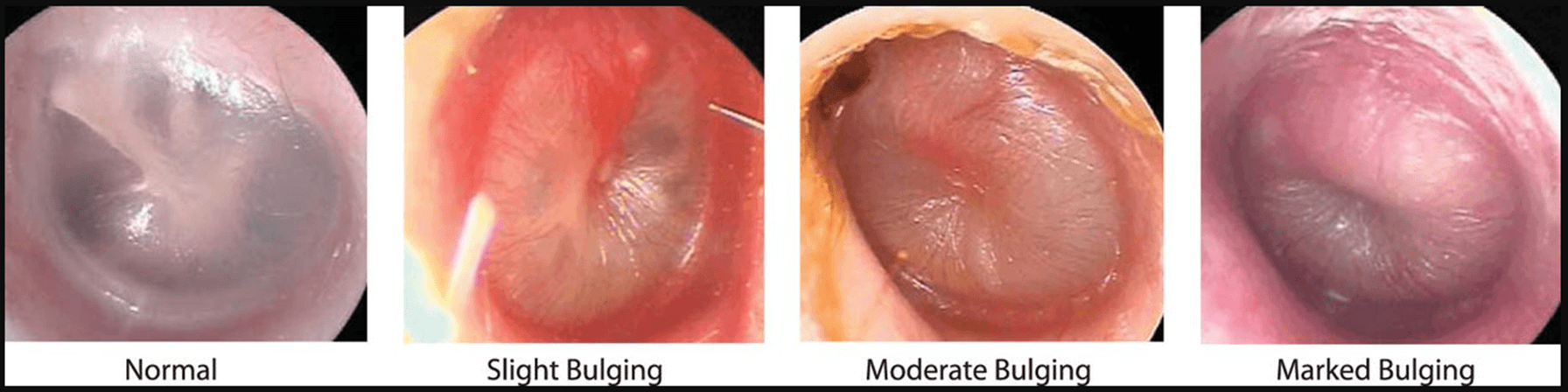
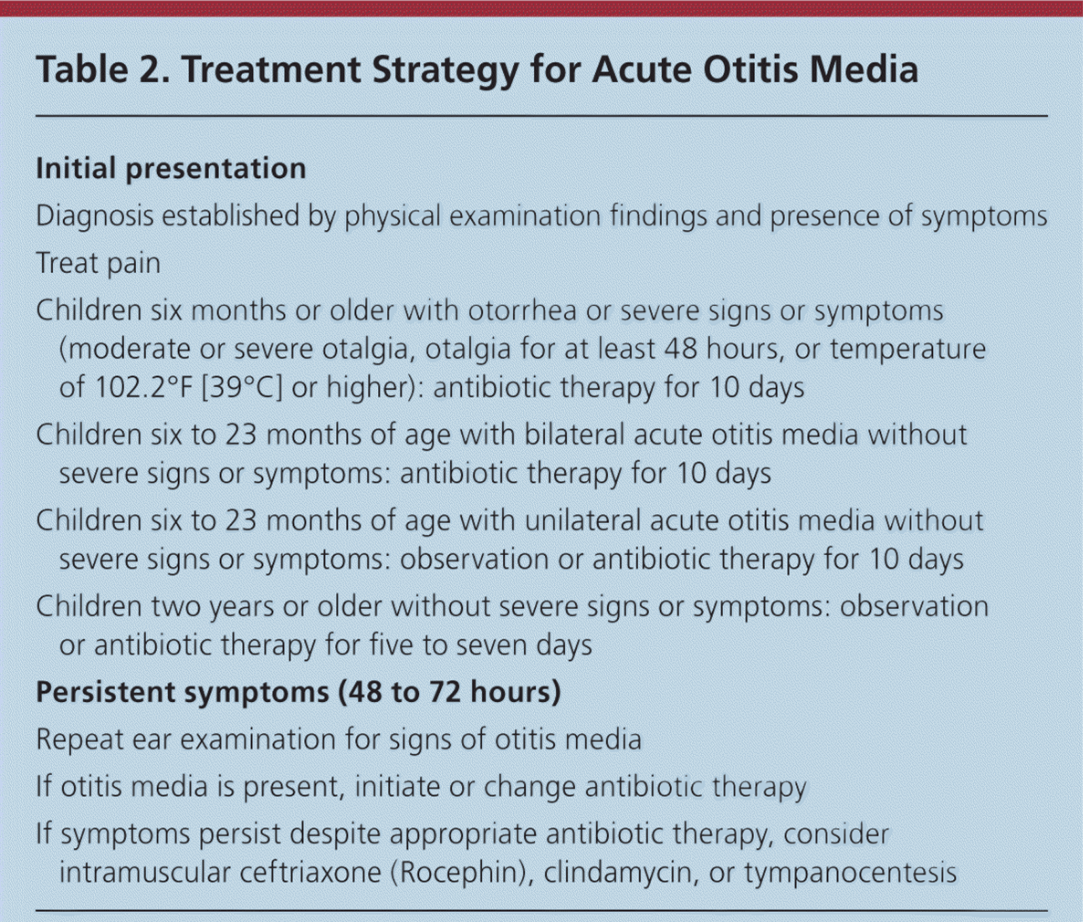
How to diagnose AOM
-Requires moderate to severe bulging of the tympanic membrane, new onset of otorrhea not caused by otitis externa,
- Or mild bulging of the tympanic membrane associated with recent onset of ear pain (less than 48 hours) or erythema
200
What are the common cause of acute sinusitis ( viral and bacterial)
•Often caused by an upper respiratory tract infection generally of viral origin
•Rhinovirus
•parainfluenzal virus
•influenza virus
• •
• Bacterial infection: most common etiological agents
•Streptococcus pneumoniae
•Haemophilus influenzae
•Moraxella catarrhalis
200
What is mastoiditis? what is the clinical manifestation?
•Purulent exudate collects in the mastoid air cells-> pressure that may result in erosion of the surrounding bone and the formation of abscess-like cavities that are usually evident on CT
•
•Symptoms:
•Pain
• Erythema
•Swelling of the mastoid process along with displacement of the pinna and acute middle-ear infection symptoms
200
Describe this picture? what are its different causes?

200
What is this xray finding called? what diagnosis is it characteristic of?
300
what is the treatment of AOM
What is first line?
Children less than 2year old?
Most resolve within 1 week: can be observe
if no improvment after 48h to 72hr then antibiotic
Amoxicillin remains DOC
•5 to 7 days for uncomplicated
•Longer courses ( 10 days) should be reserved for complicated cases or for children <2 years old
•For patients with known and severe allergy to β-lactam antibiotics: Can use a Macrolide
300
What are some clinical manifestation of acute sinusitis? give at least 3
•Nasal drainage and congestion
•Facial pain or pressure
•Headache
•Thick, purulent or discolored nasal discharge
•Often thought to indicate bacterial sinusitis
•Occurs early in viral infections such as the common cold
•Other nonspecific symptoms
cough, sneezing, and fever
•Tooth pain
most often involving the upper molars: associated with bacterial sinusitis
300
What is the treatment of mastoiditis?
•Cultures of purulent fluid should be performed
•Initiate empirical therapy against organisms associated with acute otitis media
•severe or prolonged courses: S. aureus and gram-negative bacilli (including Pseudomonas)
• Most treated conservatively with IV antibiotics
•Surgery (cortical mastoidectomy)
•Reserved for complicated cases
•If conservative treatment has failed
300
a 22 year old male college student present to the office with complaints of pharyngitis, fever, fatigue and lymphadenopathy.
what diagnosis is on your top differential? how do you diagnosis it? treatment? and what precaution do you discuss with the patient
infectious mononucleosis
- diagnosis: get good history, physical exam (splenomegaly, rash( urticarial or pethechial) , cervical lymphadenopathy)
CBC with differential and heterophile test ( eg monospot test or EBV specific antibody testing) and diagnostic eval for strep infection by culture or antigen testing
labs abnormalities:
: CBC: look for absolute or relative lymphocytosis, increase atypical lymphocytes and CMP: elevated transaminase
- treat: supportive,
don't give acyclovir
if have impending airway obstruction give corticosteroid and refer to ENT
precaution: return to spotn noncontact gradually restart in 3 weeks from symptoms onset
for contact sport or activities associated with increased intrabdominal pressure- minimum wait of 4 weeks after illness onset
300
What are the clinical manifestation of epiglotitis?
•Onset is rapid: less than 24 hour
•Marked by:
• High fever
•Toxic appearance
•Dysphonia
•Dysphagia
•Severe sore throat followed by respiratory distress
•Drooling while sitting forward
•Inspiratory stridor and retractions of the chest wall
400
How to diagnose acute otitis externa and how to treat it?
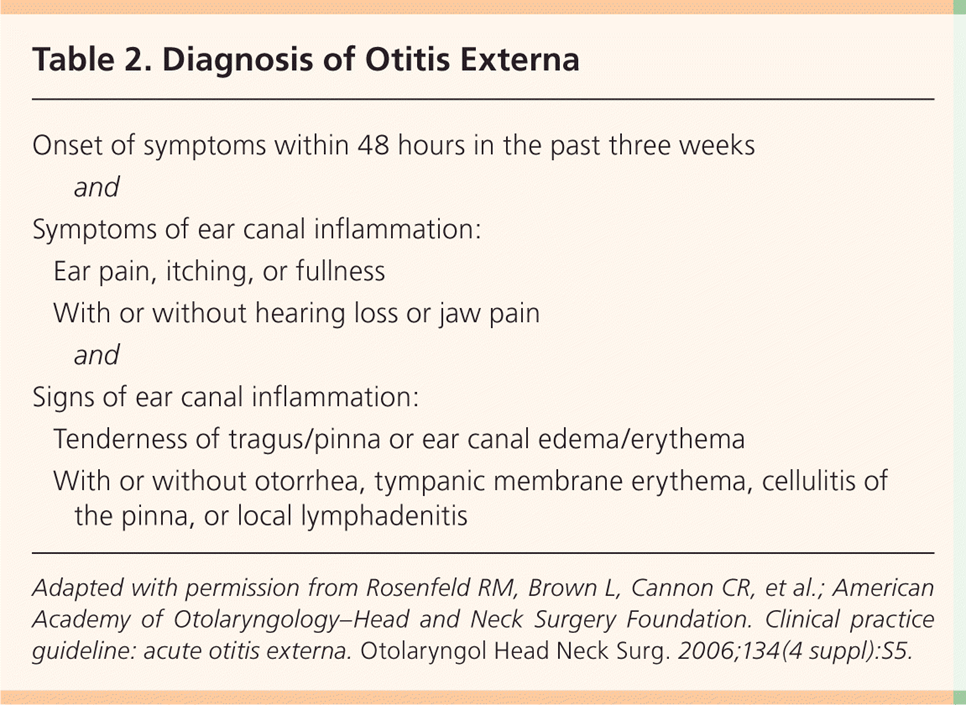
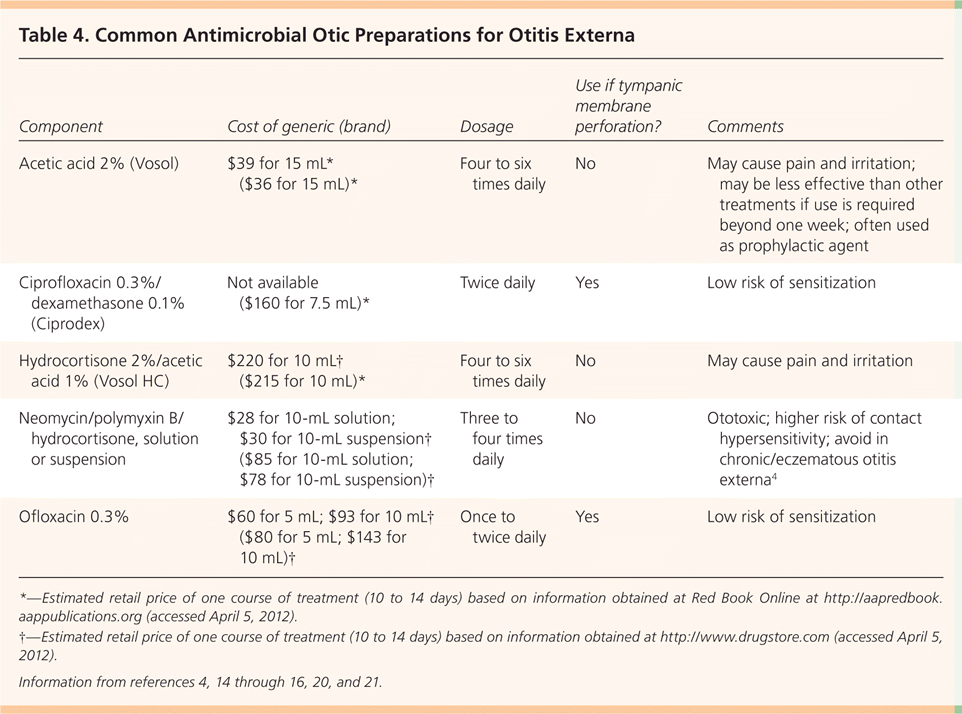
Acute localized otitis externa
Acute diffuse otitis externa: swimmer's ear
Chronic otitis
Invasive otitis externa



400
What is the management of acute sinusitis?
•Viral sinusitis typically lasts for 7 to 10 days
•Facilitate sinus drainage – oral and topical decongestants, nasal saline lavage
•Bacterial sinusitis is more persistent (after 7 days)
•Antibiotic treatment
•Amoxicillin/clavulanate (Augmentin)
•Fluoroquinolones and macrolide antibiotics (if PCN allergic)
•The recommended length of antibiotic therapy is 10 days, based on a randomized controlled trials (RCTs).
•Corticosteroids
•Intranasal corticosteroids are used in combination with antibiotics
•If do not respond to antibiotics, may need sinus aspiration or lavage
400
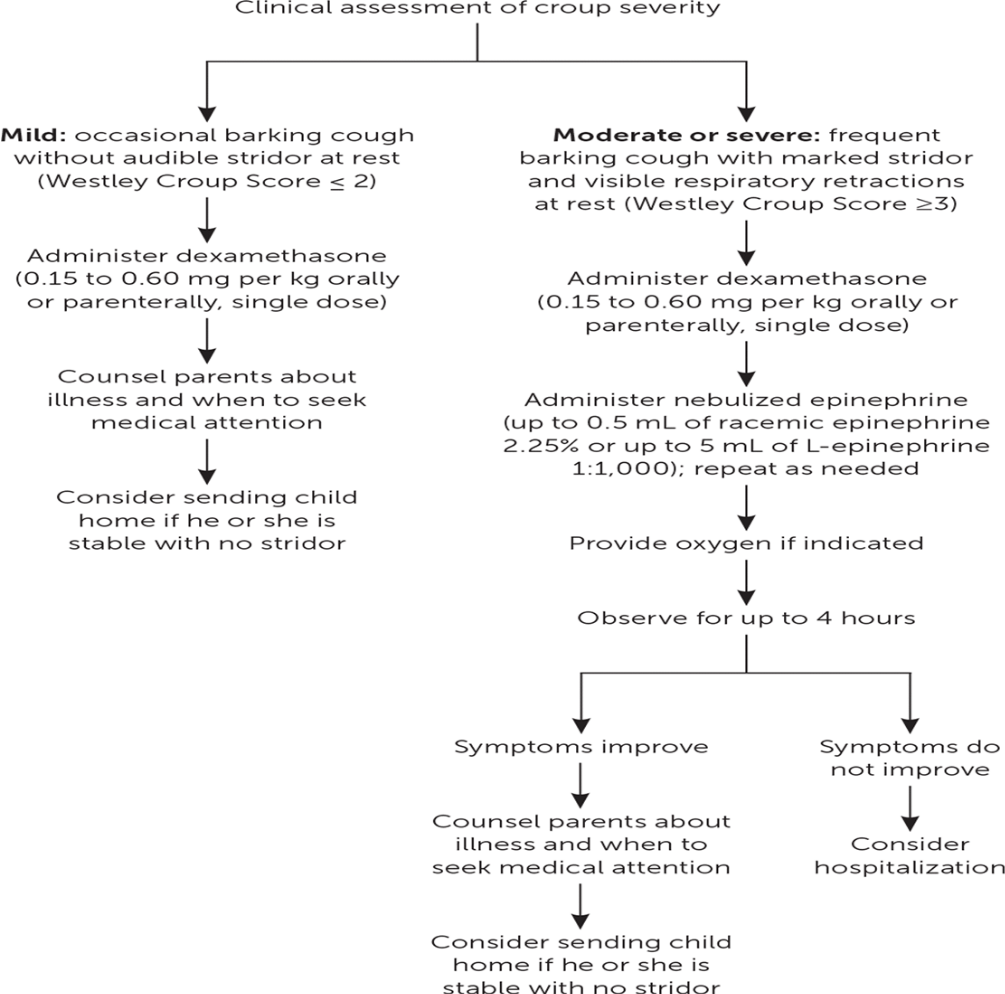
What is Acute laryngotracheobronchitis?
What is its presentation?
what is the management?
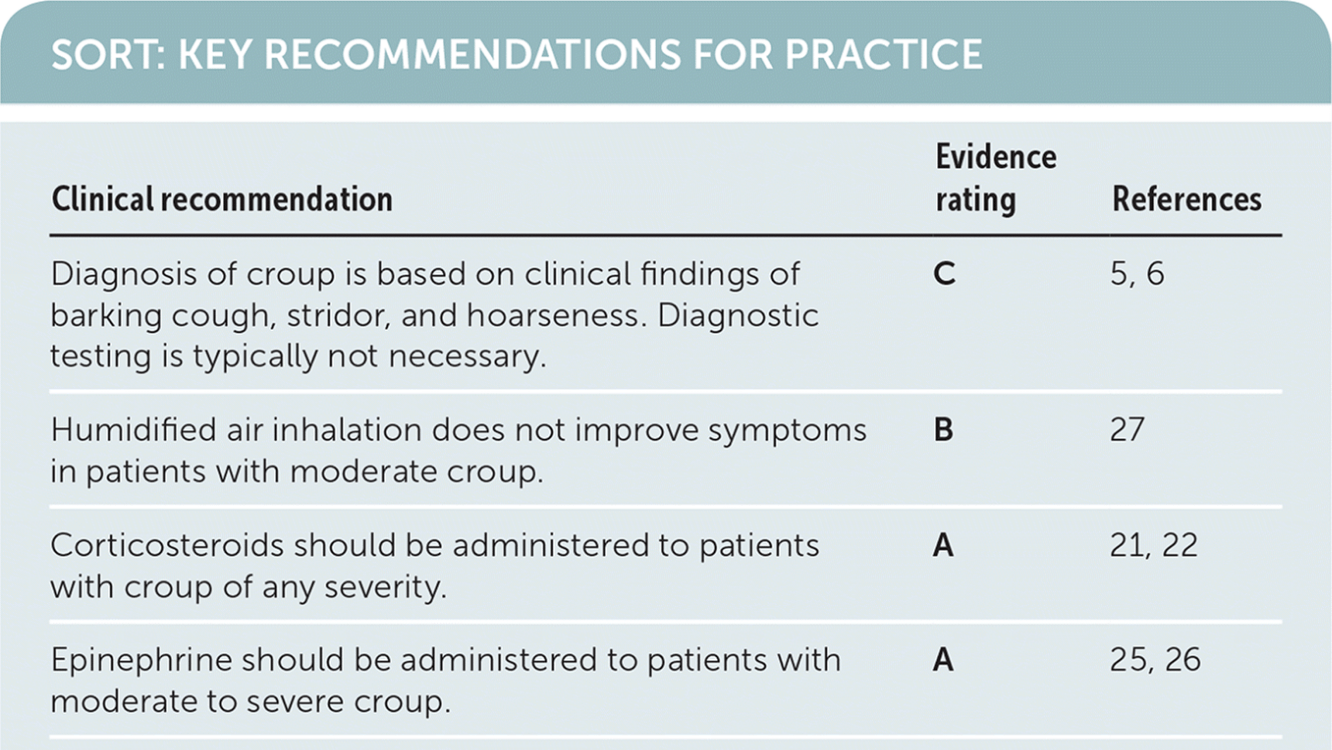
Croup
•Viral infection that consists of inflammation in the subglottic area.
•Etiology: parainfluenza viruses, influenza A, B viruses, respiratory syncitial virus, adenovirus, rhinovirus, enterovirus, and rarely, Mycoplasma pneumoniae.
•Symptoms: hoarseness, seal-like barking cough, inspiratory stridor
•CXR: steeple sign (narrowing of larynx and trachea below level of glottis)
•Therapy: humidification, good supportive care (hydration, analgesics, avoid smoking in house, keep child’s head elevated), corticosteroids
400
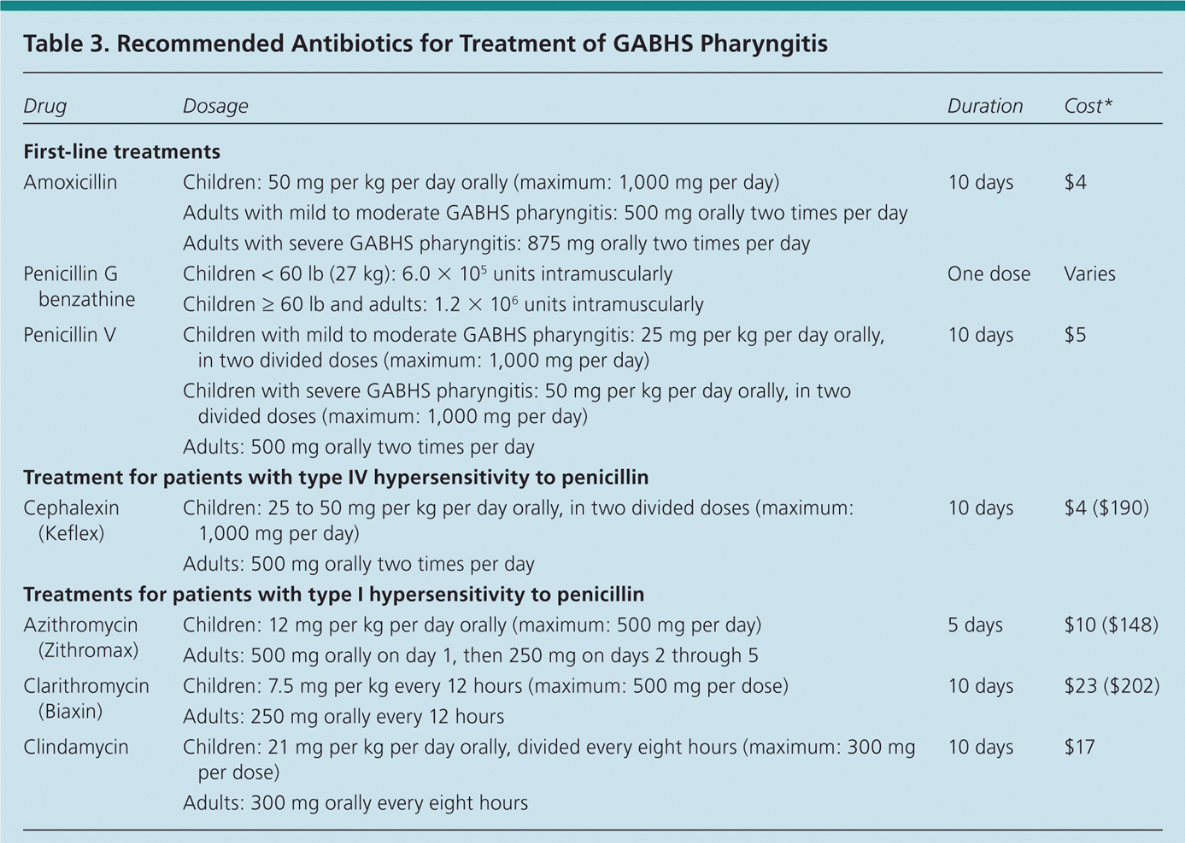
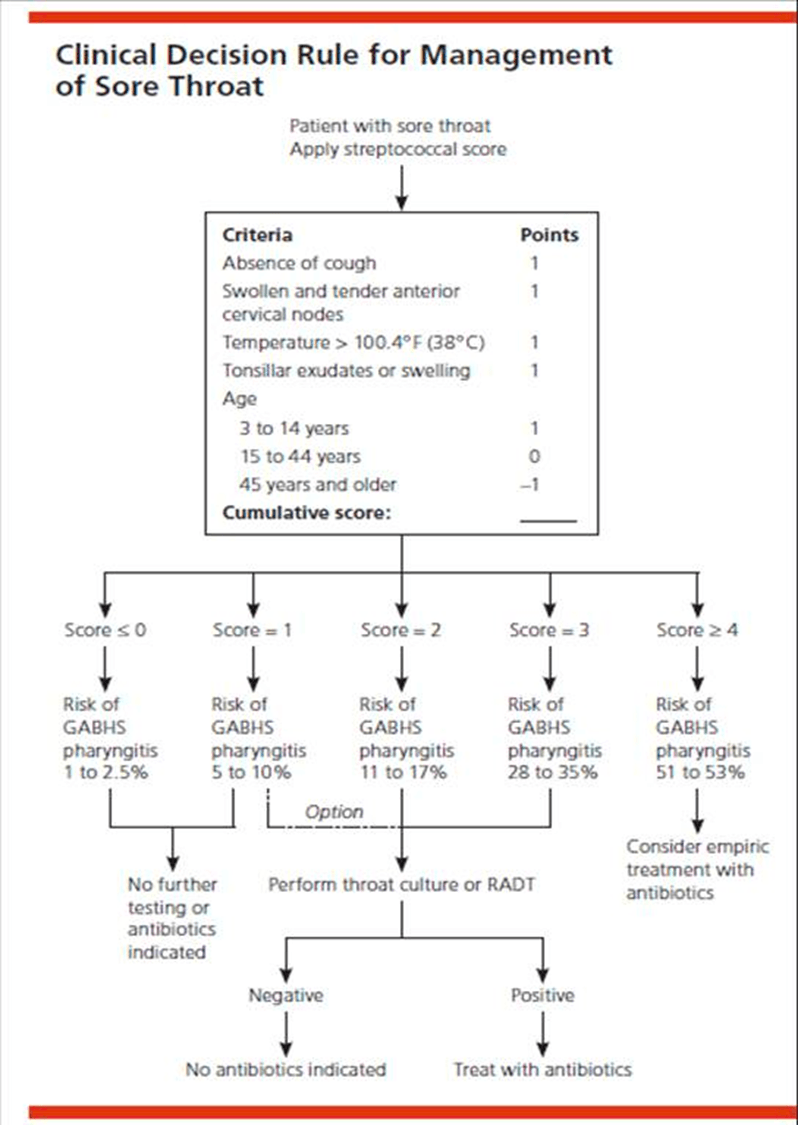
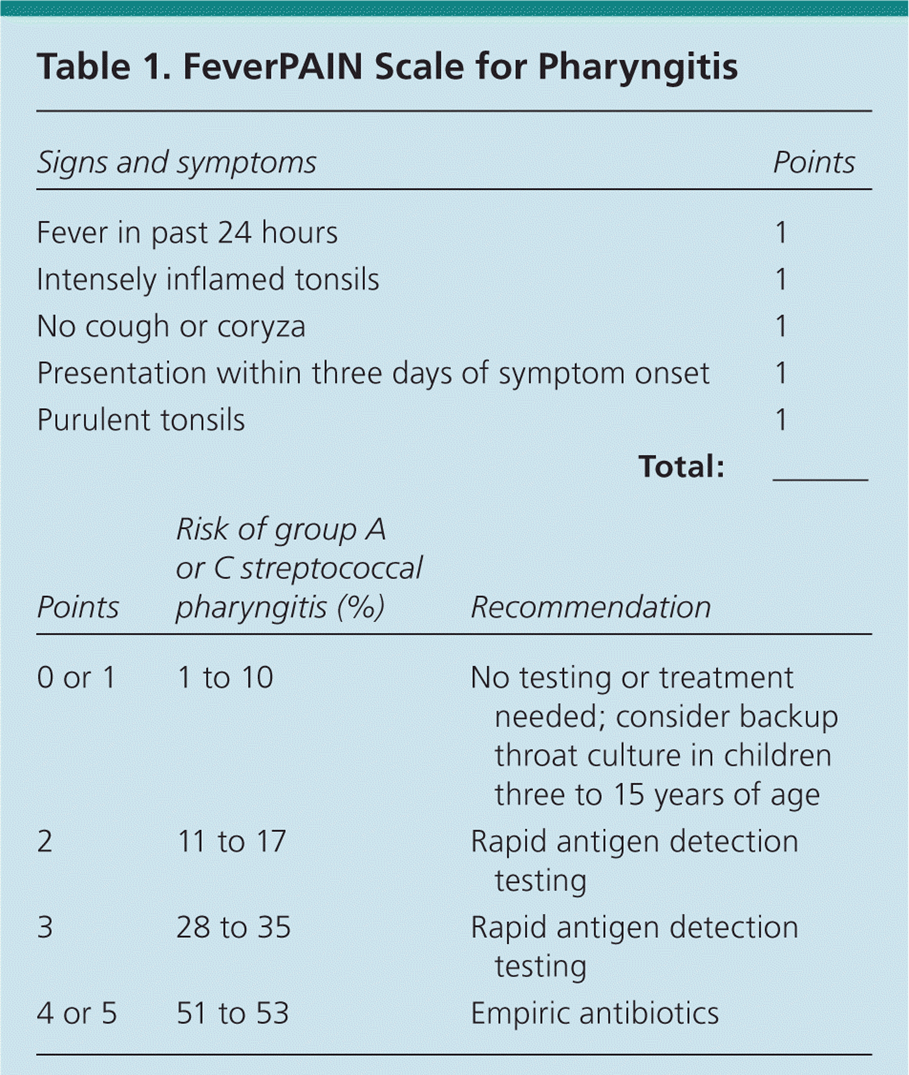
What is the treatment of pharyngitis?
400
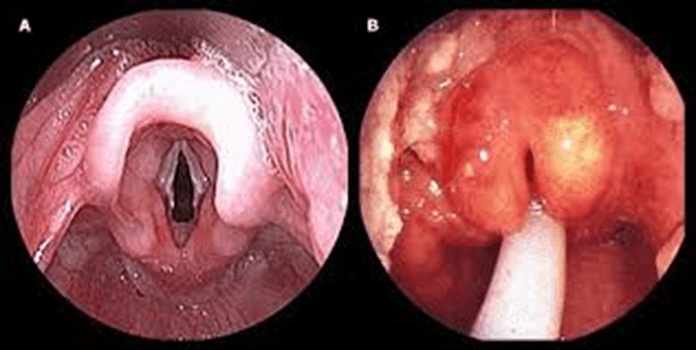
How to diagnose epiglottitis?
Clinical diagnosis:
•Direct fiberoptic laryngoscopy: "cherry-red" epiglottis facilitate placement of an endotracheal tube
• Direct visualization in an examination room (e.g., with a tongue blade and indirect laryngoscopy) is not recommended
 lateral xray: thumb print sign, don't delay treatment
lateral xray: thumb print sign, don't delay treatment
lab: mild leukocytosis, culture usually positive
500
What is Serous Otitis Media? How to treat it?
•When fluid is present in the middle ear for an extended period and in the absence of signs and symptoms of infection
• In general, acute effusions are self-limited: most resolve in 2 to 4 weeks
• In some cases, after an episode of acute otitis media :effusions can persist for months
•Often associated with a significant hearing loss
treatment
•Decongestants, and corticosteroids administered alone or in combination with an antihistamine
• Antibiotic therapy or myringotomy with insertion of tympanostomy tubes is typically reserved for patients in whom bilateral effusion:
(1) has persisted for at least 3 months
(2) is associated with significant bilateral hearing loss
500
What is this xray finding called? what diagnosis is it characteristic of?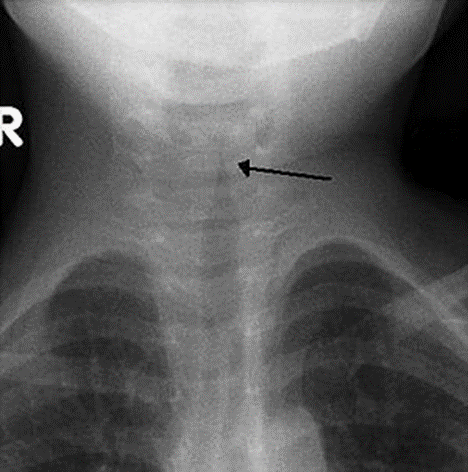
Steeple sign
croup

500
What is the classic triad of Meniere disease?
1.Episodic Vertigo
Rotatory spinning or rocking, 20 mins – 24 hours
2.Tinnitus
Maybe fluctuating or constant. May occur with vertigo, or independently.
3.Hearing loss
-Often presents EARLY, FLUCTUATES, and initially affects only the LOWER frequencies.
-Typically progresses to permanent hearing loss over 8 to 10 years
500
what are the tools to help you diagnose and manage acute pharyngitis? think algorithm
500
How to treat acute epiglottitis?
•Secure of the airway
•Intravenous antibiotics, particularly against H. influenzae
•Because of increasing ampicillin resistance
•therapy : a ß-lactam/ß-lactamase inhibitor combination or a second- or third-generation cephalosporin
•intravenous therapy with antibiotics such as: cefotaxime (100-180mg/kg/day), ceftriaxone (80-100mg/kg/day) or amoxicillin-clavulanic acid(200mg of amoxicillin/kg/day) for 7-10 days.