PAEDS HOSPITAL POLICY
Airways & Breathing
Difficult DKA's
HANDED-OVER
Coworkers & Colleagues
100
What's the mg/kg range for Paracetamol?
15-20mg/kg!
100
Stridor noise is made during what part of respiration?
Inspiration! Though children with impending respiratory collapse or post exercise can have a biphasic stridor.
100
Where can you find the protocol to manage a Paediatric DKA?
100
What's the acronym we use to hand over patients to the ward?
.transfer ed
(If you don't have this, you an import the original from Anita Fenech or a form fillable version from Dylan Dickerson)
100
Which now-retired EN used to host fabulous cooked breakfasts in the tearoom?
EN Gary Eastham!
200
What's the special cohort you CANNOT nurse initiate medications for in paediatrics?
Neonates!
200
You want to start High-Flow (HHFNC) for a respiratory child in Paediatrics. They weigh 16kg.
How many LPM should you set the flow to?
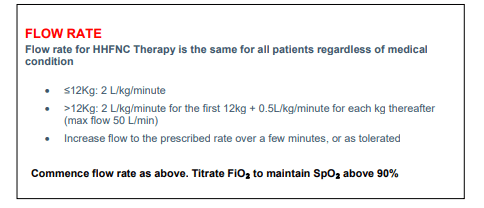
This gives us an answer of 26 LPM
See the below protocol for more information
Humidified High Flow Nasal Cannula Therapy- Paediatric
200
What are the three main molecules/values that we manage by giving intravenously in a DKA?
Potassium (K+)
Insulin (Which drives down serum K+ & Glucose)
Glucose
200
Where do you document an ISBAR handover?
In the Discharge/Transfer Tab
200
Which ED Nurse & NPC duo organise the majority of our social events within ED?
Glenn & Sarah!
300
You take a VBG from an adult patient.
PH 7.41
CO2 45
HB 112
K+ 2.9
Lactate 4.2
What's the first thing you should do?
Call a CRT!
A lactate of >4.0 is a CRT/MET call per policy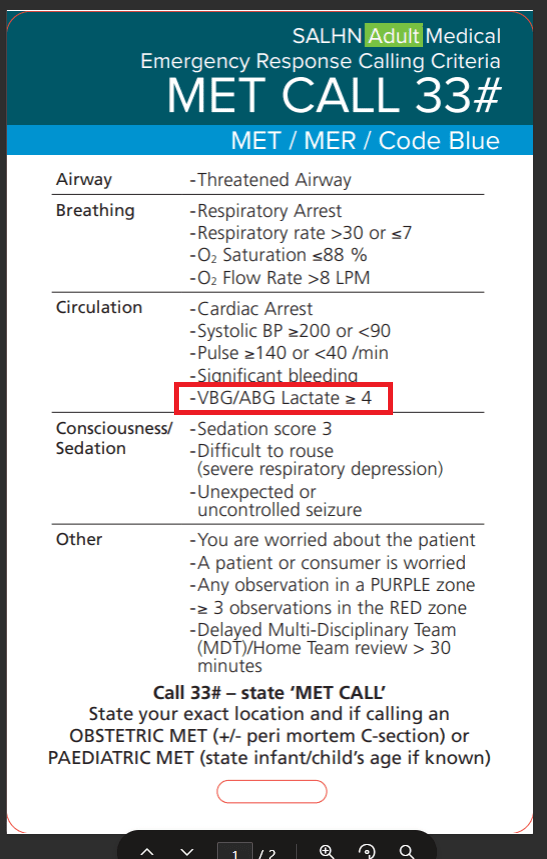
300
When a patient in respiratory distress begins grunting, they are attempting to naturally generate what phenomenon in their lungs?
PEEP! (Positive-End Expiratory-Pressure)
If your patient is trying to make or improve their own PEEP, this is a very late sign of significant respiratory deterioration.
This patient is extremely unwell, and requires escalation.
300
In Diabetes type 1, the body cannot produce enough insulin to meet demand. How does this happen?
Beta Cells within the Islet of Langerhans inside of the Pancreas are destroyed through an autoimmune process. (Or something to that effect)
300
LIGHTNING ROUND
EACH TABLE SELECT ONE VOLUNTEER
ONE BUZZER - FOUR CONTESTANTS.
FASTEST WITH A CORRECT ANSER WINS THE ROUND.
10 ROUNDS AVAILABLE.
THE PERSON WITH THE MOST ROUNDS WINS DOUBLE POINTS FOR THIS QUESTION FOR THEIR TEAM - WRONG ANSWERS HAVE NO PENALTY
START WITH YOUR HANDS BEHIND YOUR BACK, YOU CAN MOVE WHEN I SAY GO.
YOUR QUESTION IS - THINGS YOU WOULD DOCUMENT IN A HANDOVER
300
WHO'S THAT ED NURSE?
Which ED nurse received an award from SALHN on their work for the LGBTQIA+ experience within the department?
It's Liana!
400
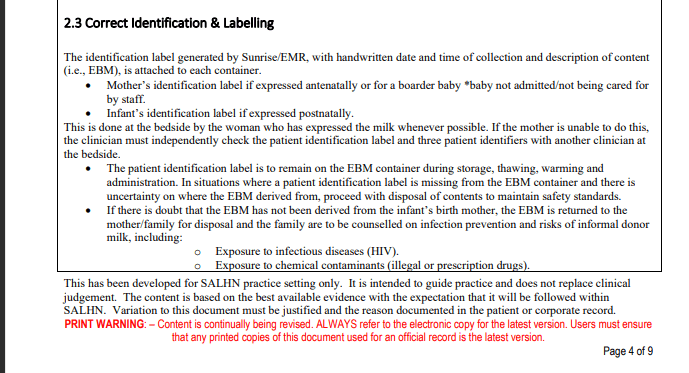
What's the process for the labelling and storage of Expressed Breast Milk? (EBM)
400
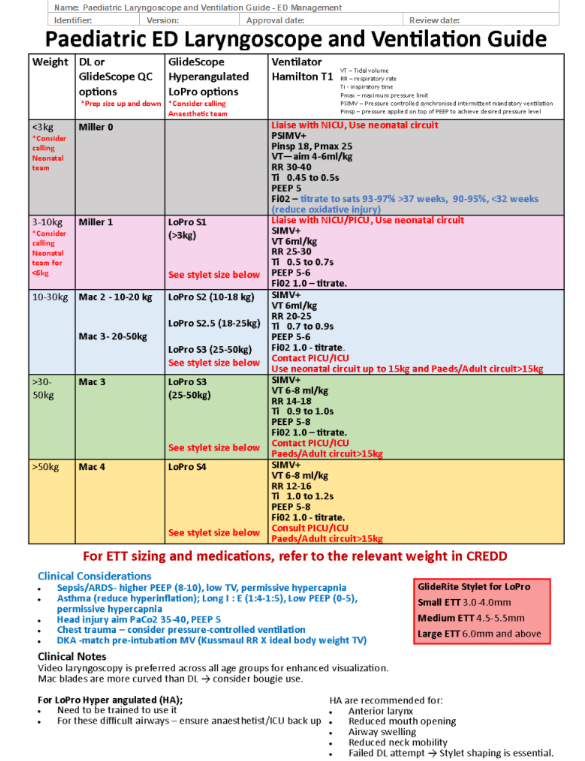
For a 20kg child how many Mls/Kg should you aim for when targeting an accurate TV on the ventilator?
6ml/kg! And a bonus plug for the new ventilation guide in resus.
400
Name the three main pathophysiological mechanisms that will actually kill a DKA patient.
1. Dehydration due to osmotic shift
2. Hypo/Hyperkalaemia
3. Cerebral Oedema
400
You are nursing a patient in S14 with a Nurse Special for delirium. You perform an ISBAR handover and a PSA arrives to take handover. Do they stay in ED, follow the patient, or something else? What do you need to do next for the Nurse Special?
Every situation is different.
Contact the Shift Co-Ordinator for clarification re: allocation.
400
Which ED Nurse was once on the front cover of the SALHN Resuscitation Workbook?
Barry Stark!

500
You receive a 3 YO child into P02. They are Alert, Crying and moving all four limbs independently.
What's their GCS? AND Where's the specific place it should be recorded?
They are GCS 14 - Children lose 1 point for crying which is equivalated as "Confused"
It should be recorded in the Paediatric GCS heading in sunrise!
500
Due to a nasty case of bronchiolitis, you need to insert an NG into a three month old child.
The child has a history of laryngomalacia, severe reflux and spent several days in NICU for jaundice at birth.
Per the protocol - can you as nursing staff insert an NG? Why/why not?
NO - severe gastro-oesophageal reflux is a contraindication. Always thoroughly check the patient history prior to inserting an NG.
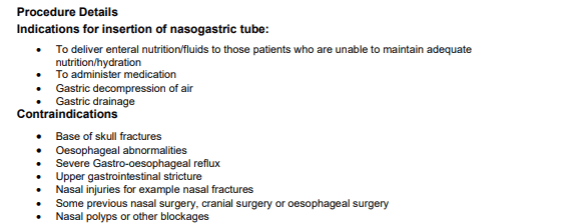
For a bonus 500 points - why is reflux a contraindication?
500
A 14 year old boy with known poorly Type-2 diabetes presents on the background of a recent illness with a BGL of 37.9 on a VBG, polyuria, polydipsia and fatigue. Ketones are 0.2.
What's the presentation? - and how does the treatment differ from standard DKA?
Hyperglycaemic Hyperosmolar Syndrome!
Similar to DKA, but without the ketosis, and commonly only in T2DM. Treatment revolves around more fluid resuscitation, less insulin, though both will still be required.
500
You've got a patient in North 3 who has been admitted to 5B. They're RWT, and have a green allocated bed, but you can't get in touch with the 5B shifty to hand over. What's the next step?
ED Nurse escort up to the ward for a FACE TO FACE handover
500
ED Consultant Phil Aplin is an avid participant in which sporting activity?
Cycling!
600
Children are often difficult to obtain blood pressures on. Per policy, given that blood pressure is an extremely late sign of deterioration in children, is there a requirement to obtain a blood pressure for paediatric patients?
YES - the observations policy within SALHN *does not* exclude children from having blood pressures.
Informally, some clinicians may permit discharge/admit if one normal BP is recorded, however we should aim for BP's on children as standard for all other patients.
600
What are the 4 Considerations of the AMAX 4 Resuscitations for ASTHMA?
A - ?
M -?
A - ?
X - ?
4 - ?
(I will accept ANY of the X's - but will provide an additional 600 BONUS points if you can name them all)

600
You are managing a Paediatric DKA in Resus 5. You complete initial fluid resuscitation and repeat a VBG. Blood Glucose is now 14.5.
Potassium is now 3.9
PH is 7.38
Insulin is running at 0.1 units/hr
NaCl 0.9% + 40mmol K+ is running in the background.
What needs to happen next in terms of fluids for this patient?
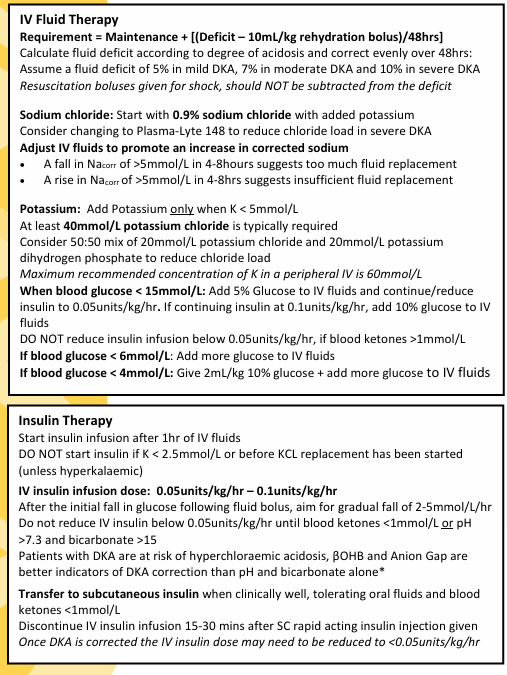
Per the protocol, we must ADD 5% glucose to the current infusion - See below.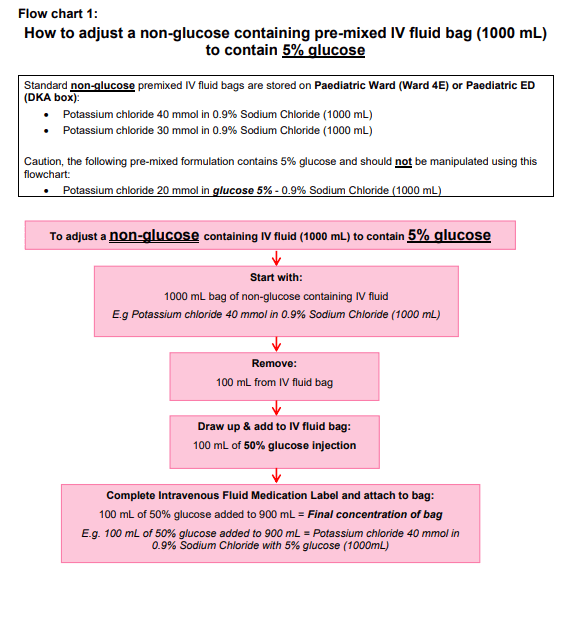
600
Do we enter a Triage Document for a direct admission to an adult ward?
No!
600
Which ED Consultant originally authored the policy we use to sedate aggressive patients? (Acute Behavioural Disturbance in Adults: Medication Management Protocols)
Jake Mallon