Acute Kidney Injury
Prerenal vs ATN
ICU AKI
Renal Replacement Theory
Hyponatremia
Hypernatremia
Potassium Disorders
Acid-Base Mastery
Daily Double
0
IF ANSWERED CORRECT CAN DOUBLE YOUR CURRENT SCORE: A patient with severe chronic hyponatremia is correcting too rapidly despite attempts to slow treatment.
What are desmopressin and D5W?
Board Pearl: DDAVP clamp therapy is a favorite nephrology board concept.
200
According to KDIGO, this isolated laboratory change is sufficient to diagnose AKI.
What is an increase in serum creatinine of at least 0.3 mg/dL within 48 hours?
Board Pearl: You do not need oliguria or a doubling of creatinine.
200
This structure is responsible for approximately 65–70% of sodium and water reabsorption.
What is the proximal tubule?
Point: Most important tubular segment on the boards.
200
Recent large ICU studies have shown that timing of this therapy - early vs late - does not improve mortality outcomes in patients with AKI.
What is renal replacement therapy?
200
This mnemonic summarizes the classic indications for emergent dialysis in critically ill patients.
What is AEIOU?
• Acidosis
• Electrolyte abnormalities
• Ingestions
• Overload
• Uremia
200
A patient with a serum sodium of 118 mEq/L presents with seizures and obtundation. Treatment?
What is an indication for immediate hypertonic saline therapy?
Board Pearl: Symptoms, not the sodium level itself, drive urgency of treatment.
200
Hypernatremia almost always represents a deficit of this substance.
What is free water?
Board Pearl: Hypernatremia is fundamentally a water problem, not a sodium problem.
200
A patient with CKD presents with a potassium of 6.8 mEq/L. What is the earliest ECG manifestation of hyperkalemia?
What are tall, narrow, peaked T waves.
Board Pearl: Hyperkalemia progresses from:
• Peaked T waves
• Shortened QT interval
• PR prolongation
• QRS widening
• Sine wave
• Ventricular fibrillation/asystole
200
A patient presents with:
• pH = 7.25
• HCO3 = 12 mEq/L
This formula is used to determine whether respiratory compensation is appropriate.
What is Winter's Formula?
PaCO2 =(1.5×HCO3)+8 ± 2
Board Pearl: Every intensivist should know Winter's Formula cold. It is the most commonly tested compensation equation.
400
A 75-kg patient produces 25 mL/hour of urine for 8 hours. By KDIGO criteria, he meets this stage of AKI.
What is Stage 1 AKI?
Calculation:
25 mL/hr ÷ 75 kg = 0.33 mL/kg/hr
Less than 0.5 mL/kg/hr for >6 hours = Stage 1.
400
This urine sodium value strongly supports prerenal azotemia.
What is urine sodium less than 20 mEq/L?
400
The most common cause of intrinsic AKI in the ICU.
What is acute tubular necrosis?
Incidence 40–88% among intrinsic causes.
400
A patient with septic shock develops AKI requiring dialysis. He is receiving norepinephrine and vasopressin and remains hypotensive despite resuscitation. This modality is preferred.
What is CRRT?
Board Pearl: CRRT is preferred in hemodynamically unstable patients because fluid and solute removal occur gradually.
400
A patient with pneumonia has:
• Serum Osm = 265 mOsm/kg
• Urine Osm = 550 mOsm/kg
• Urine Na = 60 mEq/L
• Appears euvolemic
What is SIADH?
Board Pearl: Euvolemic hypotonic hyponatremia with inappropriately concentrated urine.
400
A patient has:
• Na = 160 mEq/L
• Serum Osm = 325 mOsm/kg
• Urine Osm = 100 mOsm/kg
• Polyuria
This diagnosis should be suspected.
What is diabetes insipidus?
400
A patient presents with:
• Potassium 7.2 mEq/L
• QRS duration 180 ms
• Muscle weakness
What is the first medication that should be administered?
What is intravenous calcium gluconate?
Board Pearl: Calcium does not lower potassium. It stabilizes the cardiac membrane and should be given first when ECG changes are present.
400
A patient has:
• pH 7.28
• HCO3 12
• PaCO2 40
Winter's Formula predicts a PaCO2 of approximately 26. This disorder is also present.
What is a concurrent respiratory acidosis?
Board Pearl: If measured PaCO2 is higher than predicted, respiratory compensation is inadequate and a second disorder is present.
600
A patient develops AKI after septic shock. Urine sodium is 8 mEq/L, FENa 0.5%, but urine microscopy shows muddy brown casts.
What is acute tubular necrosis?
Point: Urine sediment beats FENa. Muddy brown granular casts are one of the highest-yield AKI findings on the boards.
600
In this syndrome heart dysfunction leads to decreased kidney perfusion.
What is cardiorenal syndrome?
600
A patient with decompensated heart failure loses 4 kg after diuresis. Creatinine rises from 1.4 to 1.9 mg/dL but congestion improves. What should you do?
What is continue aggressive decongestion?
Board Pearl: A rise in creatinine with successful decongestion does not necessarily indicate a worse prognosis.
600
A patient with traumatic brain injury develops severe hyperkalemia requiring dialysis. This renal replacement modality should generally be avoided because rapid osmotic shifts may worsen cerebral edema.
What is intermittent hemodialysis (IHD)?
Board Pearl: CRRT is preferred in patients with acute brain injury, elevated intracranial pressure, or acute liver failure.
600
A patient develops hyponatremia after subarachnoid hemorrhage. Urine sodium is 80 mEq/L, urine osmolality is 700 mOsm/kg, and the patient is hypotensive with evidence of volume depletion.
What is cerebral salt wasting?
Board Pearl: The major distinction from SIADH is hypovolemia. SIADH patients are euvolemic.
600
After water deprivation testing, urine osmolality increases by 70% following desmopressin administration.
What is central diabetes insipidus?
Board Pearl: Central DI responds to DDAVP; nephrogenic DI does not.
600
A patient with severe hyperkalemia receives:
1. IV calcium
2. Regular insulin and dextrose
This is the next physiologic goal of treatment.
What is remove potassium from the body?
Board Pearl: The treatment sequence is:
1. Stabilize myocardium (Calcium)
2. Shift potassium intracellularly (Insulin ± glucose, β-agonists, bicarbonate)
3. Remove potassium from the body (Diuretics, binders, dialysis)
600
A patient has:
• Na = 140
• Cl = 100
• HCO3 = 10
Calculate the anion gap.
What is 30?
AG = 140 − (100+10) = 30
Board Pearl: An AG ≥12 is abnormal and should trigger evaluation for GOLDMARK causes.
800
This urinary index is preferred over FENa in a patient receiving loop diuretics.
What is FEUrea?
Board Pearl: FEUrea <35% supports prerenal physiology. Diuretics can invalidate FENa.
800
This urine sediment finding is most characteristic of ATN.
What are muddy brown granular casts?
800
This finding is an independent predictor of mortality in critically ill patients with ATN.
What is positive fluid balance?
Even modest fluid accumulation worsens outcomes.
800
A 100-kg patient is prescribed CRRT with an effluent rate of 2000 mL/hour. This delivered dose is considered adequate according to current recommendations.
What is 20 mL/kg/hour?
Calculation: 2000 ÷ 100 = 20 mL/kg/hr
Board Pearl: Standard CRRT dosing is approximately 20–25 mL/kg/hr. Higher doses have not improved mortality.
800
This is the first-line treatment for most patients with chronic SIADH who are asymptomatic or mildly symptomatic.
What is free water restriction?
Board Pearl: Treat the underlying cause plus fluid restriction.
800
A patient develops hypernatremia while receiving lithium therapy. Urine osmolality remains low despite desmopressin administration.
What is nephrogenic diabetes insipidus?
Board Pearl: Lithium is the classic cause.
800
A diabetic patient has:
• K = 5.9 mEq/L
• HCO3 = 18 mEq/L
• Normal anion gap metabolic acidosis
• Mild CKD
• No diarrhea
What is Type 4 renal tubular acidosis?
Board Pearl: Hyperkalemia + non-anion gap metabolic acidosis = Type 4 RTA until proven otherwise.
800
A patient has:
• AG = 30
• HCO3 = 18
The delta anion gap is 18 and the delta bicarbonate is only 6. What is the disorder(s)?
What is a mixed high-anion-gap metabolic acidosis and metabolic alkalosis?
Board Pearl:
When: ΔAG > Δ HCO3, a metabolic alkalosis is hiding underneath the acidosis. This is classic in:
• DKA + vomiting
• Alcoholic ketoacidosis + vomiting
• Salicylate toxicity
1000
A patient with septic shock develops AKI. A plasma biomarker level is elevated at 250 ng/mL and suggests tubular injury, but does not establish AKI by KDIGO criteria.
What is NGAL (Neutrophil Gelatinase-Associated Lipocalin)?
Point: Predicts injury but is not part of the AKI definition.
1000
A patient has AKI with pyuria, eosinophilia, WBC casts, and recent cefepime exposure.
What is acute interstitial nephritis?
Board Pearl: Fever, rash, and eosinophilia occur together in fewer than 10% of cases.
1000
A cirrhotic patient develops AKI. Urine sodium is 8 mEq/L. Urinalysis is bland. Creatinine fails to improve after albumin challenge and diuretic withdrawal.
What is hepatorenal syndrome–AKI?
1000
This is the preferred anticoagulation strategy for CRRT because it prolongs circuit life and minimizes systemic bleeding risk.
What is regional citrate anticoagulation?
Board Pearl: Citrate is preferred over systemic heparin when feasible.
1000
A patient with chronic hyponatremia has his sodium corrected from 108 to 122 mEq/L in 12 hours. What is the risk?
What is overcorrection placing the patient at risk for osmotic demyelination syndrome (ODS)?
Board Pearl: Chronic hyponatremia should generally not increase more than 8–10 mEq/L in 24 hours.
1000
A 70-kg man has a sodium of 168 mEq/L. This equation is used to calculate his free water deficit.
What is: Free Water Deficit = TBW x (Current Na/Desired Na -1)
1000
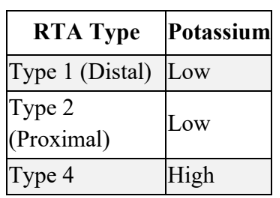
This mechanism distinguishes Type 4 RTA from Type 1 and Type 2 RTA.
What is hypoaldosteronism (or aldosterone resistance) causing impaired potassium secretion?
Board Pearl: This is one of the most commonly tested RTA differentiations on nephrology and critical care boards.
1000
A 19-year-old with depression presents with:
• pH 7.53
• PaCO2 12
• HCO3 10
What is salicylate poisoning?
Board Pearl: Salicylates produce the classic board answer: Respiratory alkalosis + high-anion-gap metabolic acidosis.
1200
BONUS: A patient on CRRT with regional citrate anticoagulation develops worsening anion gap metabolic acidosis, low systemic ionized calcium, increasing calcium infusion requirements, and a total calcium-to-ionized calcium ratio of 2.8.
What is citrate toxicity (citrate accumulation)?
Board Pearl: The next step is to discontinue citrate and switch to an alternative anticoagulation strategy. A total calcium-to-ionized calcium ratio >2.5 is highly suggestive of citrate accumulation.
1200
BONUS: Two days after rapid correction of severe hyponatremia, a patient develops dysarthria, dysphagia, quadriparesis, and altered mental status.
What is osmotic demyelination syndrome?
Board Pearl: Alcoholism, malnutrition, liver disease, and sodium <120 mEq/L increase risk.
1200
BONUS: A patient with chronic hypernatremia has his sodium corrected from 170 to 150 mEq/L in 12 hours.
What is overly rapid correction risking cerebral edema?
Board Pearl: Chronic hypernatremia should generally be corrected by no more than about 10 mEq/L per day.
1200
BONUS: A patient develops:
• Potassium 8.2 mEq/L
• QRS duration 260 ms
• Wide-complex rhythm
A colleague recommends immediate defibrillation for presumed ventricular tachycardia. What should happen first?
What is treat severe hyperkalemia producing a sine-wave pattern?
Board Pearl: Hyperkalemia can mimic ventricular tachycardia. A QRS >240 ms strongly suggests hyperkalemia, and defibrillation before correcting potassium may be ineffective or harmful.
1200
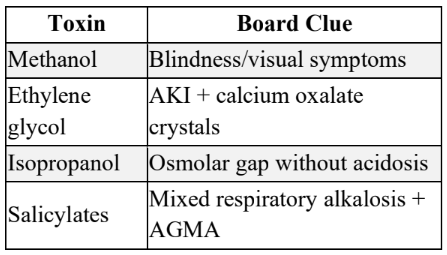
BONUS: A patient presents with:
• High anion gap metabolic acidosis
• Elevated osmolar gap
• Visual disturbances
What is methanol poisoning?
Board Pearl: The classic toxic alcohol clues: