Flag Me Down!
Necked Pics
Loosey Goosey
Neck Flex
Bio-neck-anics
Neck and Neck
Tasting Necks
100
What are the 6 Red Flags to screen for when a patient presents with neck pain?
Cervical Fracture
Upper Cervical Instability
Cerebral Artery Dysfunction
Cervical Myelopathy
Neoplastic Condition
Infectious Spinal Meningitis
100
What are considered the 3 high risk factors that mandate radiography according to the Canadian C Spine Rules?
> 65 years old
Dangerous Mechanism
Paresthesia in Extremities
100
How many degrees of freedom does a cervical vertebra have?
3 (flexion/extension, L/R rotation, L/R sidebending)
100
What muscles constitute the deep neck flexors?
Longus Colli
Longus Capitis
Rectus Capitis Anterior and Lateralis
100
What neck motions would result in an upglide?
Neck Flexion
Sidebending (contralateral side upglide)
Rotation (contralateral side upglide)
100
Your flabbergasted coworker sends a patient your way describing the patient as having a positive Upper Limb Tension Test A, positive Spurling test, and positive distraction test. Given what you know about the patient's findings and likely classification, what is the final missing exam finding that is part of the cluster?
Less than 60 degrees of ROT to involved side (Centralization or Neck Pain w Radiating Symptoms)
100
A patient arrives in the clinic with c/o neck pain accompanied by sx in the UE, name at least 2 tests/exams you would do with this patient
Spurling's/Distraction
Neural Conduction TestsNeurodynamic Tests
AROM
Pathological Reflexes
PA and UPA Glides200
Name the Red Flag: A previous patient of yours returns to PT complaining of the same neck pain of which she was just discharged for one month ago. She says that it's worsened and that her symptoms are so bad that she can't sleep through the night. As you take her through the physical exam, you are stumped at the lack of pattern her symptoms are presenting in.
Neoplastic Condition
200
True or False: In a patient w Clinical Instability, radiographs are instrumental in identifying and diagnosing.
False
200
What are the 2 major upper cervical spine ligaments?
Alar Ligament (limits ROT of C2 on C1)
Cruciform Ligament (keeps dens from traveling posteriorly)
200
What is the common functions of the hyoid muscles (omohyoid/sternohyoid/sternothyroid/thyrohyoid)?
Depression of larynx, hyoid bone, and floor of mouth
200
A patient presents with pain on the right side of their neck during R sidebending, what other motions may be painful?
Neck Extension
R Rotation
200
Name that classification: A 17 year old student comes into the clinic with c/o neck pain that came on after a long night of last minute studying for her SATs. She describes having difficulty turning her head to look over her right shoulder. She denies any radiating symptoms and describes the pain to be elicited on the right side of her neck with inflammatory motions.
Neck Pain w Mobility Deficits or Mobility Deficits
200
How would a PT rule out a Upper Cervical Instability?
Alar Ligament Testing
Sharp-Purser Test
300
What is the cluster for Cervical Myelopathy?
Age > 45
(+) Hoffman's Reflex
(+) Babinski Reflex
(+) Inverted Supinator Reflex
Gait Deviation
300
What is one indication for an MRI of the C Spine?
Degenerative Disc Disease
Soft Tissue/Bony Tumors
Spinal Cord Pathology
Spinal Infections
Congenital Spinal Abnormalities
300
What would Rib 8 articulate with?
TP and superior facet of T8
Inferior facet of T7
300
What is the common innervation of the muscles that contribute to motion of the TMJ?
Mandibular Division of the Trigeminal Nerve (CN 5)
300
A patient c/o L sided neck pain, when they are actively demonstrating their flexion ROM you notice that their chin deviates to the left. What is the significance of this deviation?
L sided hypomobility
300
Name that classification: Your significant other comes in complaining excessively of a headache; you instruct them to drink water and take ibuprofen (because you're busy studying). As they complain, they mention that the headache worsens with looking down and feels like it "climbs up the side" of their neck and into their head. They proceed to walk around the room, refusing to move their head around because "it hurts."
Cervicogenic Headache or Neck Pain with Headache or Reduce Headache
300
If a patient in the clinic presents with neck pain and associated dizziness, how would the PT proceed in order to determine the origin of the dizziness?
CAD Test
Swivel Test (r/o mechanoreceptors, visual system, and vestibular system)
400
You and your CI have just finished an initial exam on a patient with neck pain. While discussing the patient, your CI exclaims that she was shocked at how many of that 5 D's And 3 N's the patient presented with. You panic and agree, but what are those again?
Dizziness
Diplopia (double vision)
Dysphagia (trouble swallowing)
Dysarthria (motor speech disorder)
Drop Attacks
Ataxia (slurred speech, stumbling, falling, and incoordination)
Nausea
Numbness
Nystagmus (uncontrolled eye movements)
400
What is considered a dangerous mechanism according to the Canadian C Spine?
Fall from > 3 feet OR 5 stairs
Axial Load to Head
MVC High Speed (> 100 km/hour)/Rollover/Ejection
Motorized Recreational Vehicles
Bicycle Struck/Collision
400
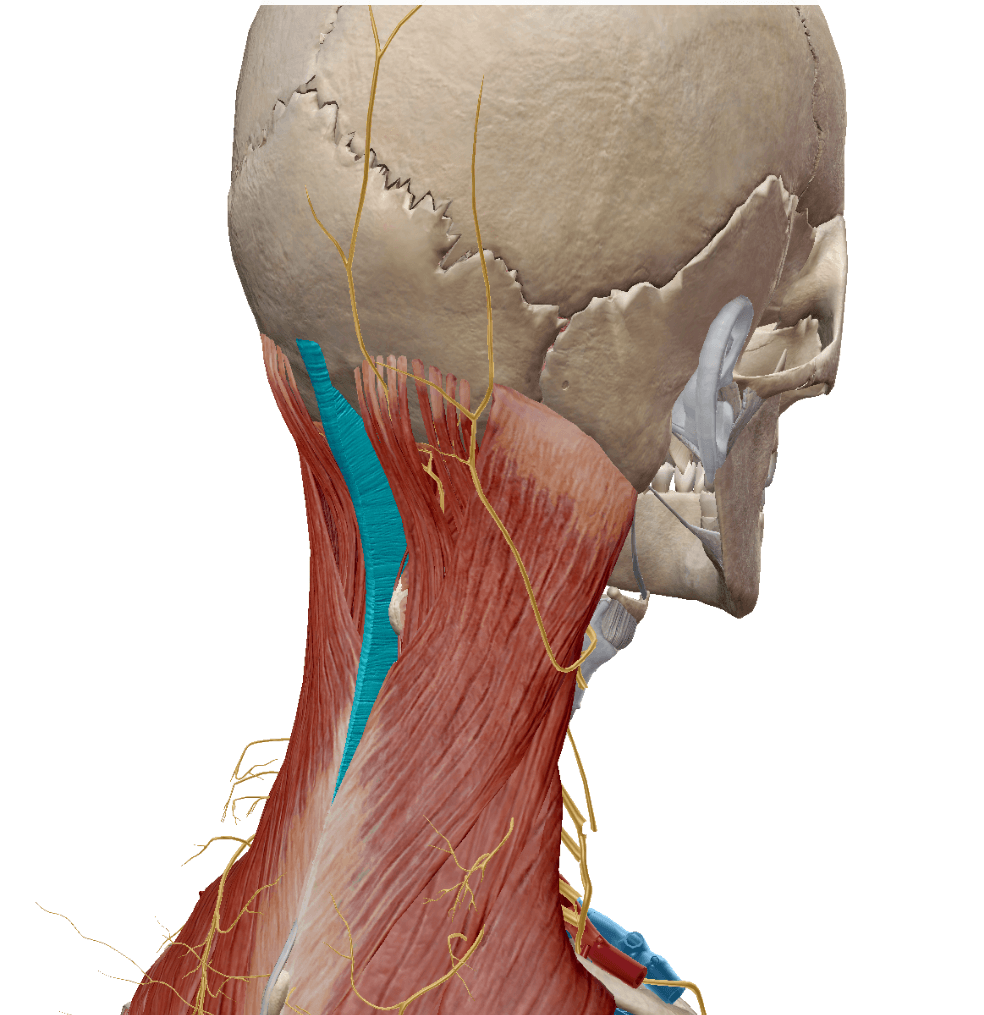
What is the highlighted structure?
Nuchal Ligament (expansion of supraspinous ligament in the C spine --> very well developed here)
400
If a patient presents with poor postural control, what muscles would you potentially target? (Name at least 3)
Mid and Lower Traps
Lats
Levator Scap
Rhomboid Minor/Major
Erector Spinae Group
400
What serves as a "protective barrier" against disc herniations in the cervical spine?
uncovertebral joints/joints of Luschka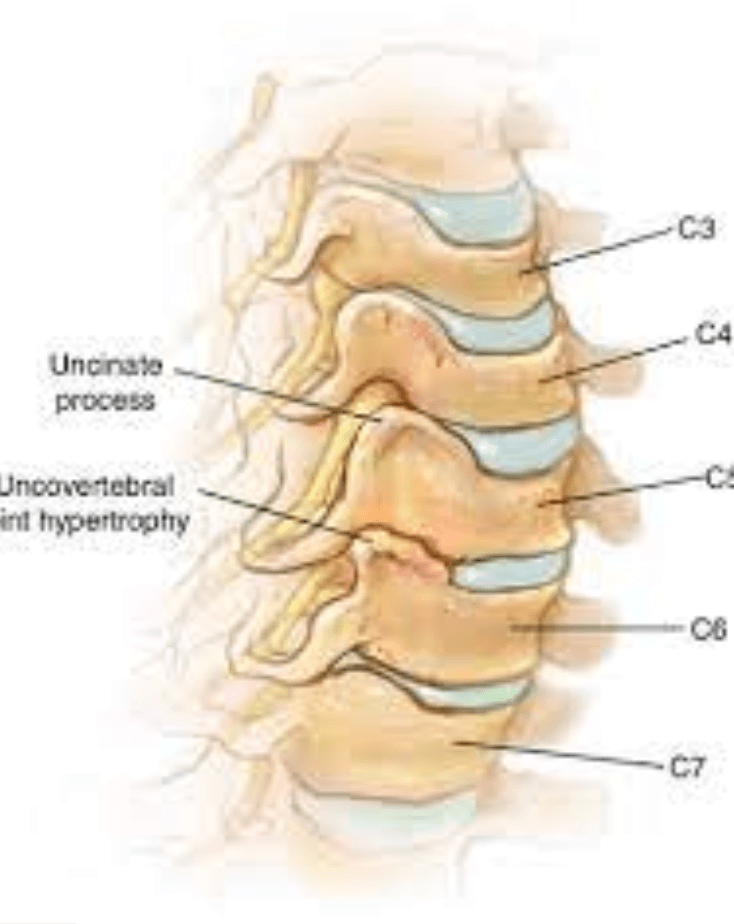
400
Name that Classification: A patient presents to PT complaining of high levels of pain, they demonstrate a "jerky" quality of motion. The patient also reports intermittently experiencing UE symptoms. When asked what decreases their symptoms, the patient reports sitting in their recliner and putting their feet up after a long day.
C-Spine Clinical Instability or Neck Pain w Movement Coordination Impairments
400
A patient demonstrates limited R sidebending with accompanying R sided neck pain, what type of manual PT might be appropriate?
Downglide at that segment (if tolerated)
Upglide at that segment on L side
BIL UPA?
500
Name the Red Flag: A patient presents to PT s/p a fall down a flight of stairs with resultant neck pain. During the physical exam, they demonstrate tenderness over the C spine and severely limited ROM. As you look over their exam intake form, you notice that they have been taking steroids for the last few months and have a family history of osteoporosis.
Cervical Fracture
500
A patient presents to PT with neck pain and absolutely refuses telling you what their MOI is, he consistently responds with "yo, it was epic" (you are suspecting some sort of head trauma at this point). During the exam, the patient is able to attain 40 degrees of left and right ROT, would you recommend imaging?
Yes
(<45 degrees of L and R ROT indicates radiography)
500
This specialized ligamentous structure is an extension of the Posterior Longitudinal Ligament
Tectorial Membrane
500
The traps, innervated by CN 11 (Accessory), make up the most superficial later of back muscles; what 3 actions does this muscle perform?
Upward Scapular Rotation
Scapular Retraction/Adduction
Scapular Depression
500
What are the actions of the upper cervical spine during L sidebending?
Occipital condyles roll left and glide right
Axis rotates L under Atlas
500
Name that Classification: A patient presents to PT s/p MVA after being cleared by the ED via extensive imaging. He complains of severe neck pain and his NDI score reflects a high level of disability; as you begin your exam, you notice he does not tolerate any increased pressure to the neck area and is too guarded to participate in any ROM measurements.
Pain Control Classification
500
A patient demonstrates diminished sensation over the pad of the third finger, if you suspected a neural conduction pattern what myotome and reflex would be affected?
Elbow Extension
Elbow DTR
600
Name the Red Flag: A PT aide previously employed by your clinic returns home from college over their spring break and are presenting to you (their favorite PT) with complaints of neck pain. As you begin the examination, you notice he is sweating a fair amount but reports feeling cold and demonstrates stiff AROM. He complains for the 10th time that his head hurts.
Infectious Spinal Meningitis
600
A patient presents to PT s/p a simple rear end with resultant neck pain. She reports that she only started feeling the pain 6 hours after the accident and does not have any midline C spine tenderness. would you recommend imaging?
No
(Because of simple rear end, delayed pain onset, and no midline C spine tenderness)
600
How would you describe where the C5 nerve root exits the spinal cord?
Between C4 and C5 (above the vertebra for which it is named)
600
What are the functions of the Splenius Capitis and Cervicis?
Neck Extension (BIL contraction)
Ipsilateral Rotation (unilateral contraction)
600
What are the normative values for total craniocervical region of flexion, extension, sidebending, and rotation? (partial credit available)
Flexion: 45 - 50
Extension: 85
Axial Rotation: 90
Sidebending: 40
600
Your coworker is describing to you a patient with neck pain involving Mobility Deficits; as you are picturing this patient's AROM in your head, which would you imagine to be restricted/limited as compared to their non-affected side?
Lateral Flexion/Side Bending
Rotation
600
What are the 5 components of the Erhard Protocol for Traction Treatment?
Intermittent
30 seconds on/10 seconds off
Patient positioned in 15 - 30 degrees of flexion
Start at 15 - 20 lbs (increasing 1 - 2 lbs/visit)
Duration = 15 minutes
700
Name the Red Flag: A patient presents to PT with neck pain that came on gradually three months ago. Her primary complaint is difficulty with picking up small items due to intense numbness and tingling. She says this feeling gets worse when she's cloud gazing with her son. You run an upper extremity neural screen and, while myo and dermatomes are normal, her reflexes are astoundingly strong!
Cervical Myelopathy
700
A 68 year old patient presents to PT s/p a fall. As you gather a history, the patient describes the fall as being from a surface approximately 3.5 feet off the ground. Would you recommend imaging for this patient?
Yes
700
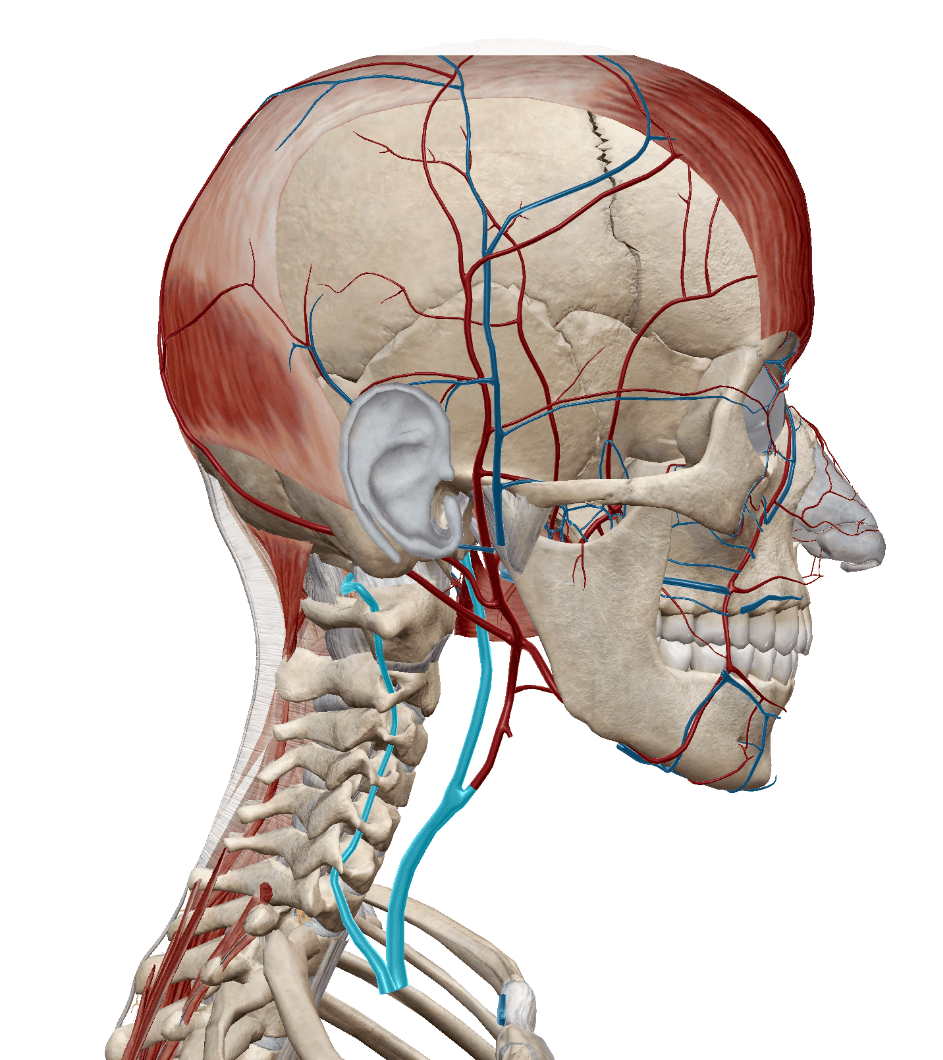
What are the 2 vessels that rise in the cervical spine to supply blood to the brain?
Vertebrobasilar Artery (extension of subclavian)
(Internal) Carotid Artery
700
In Upper Crossed Syndrome, which muscles are facilitated and which muscles are inhibited?
Facilitated: pecs, upper traps, SCM, and levator scap (also acceptable: movers)
Inhibited: neck flexors, rhomboids, lower traps, and serratus anterior (also acceptable: stabilizers)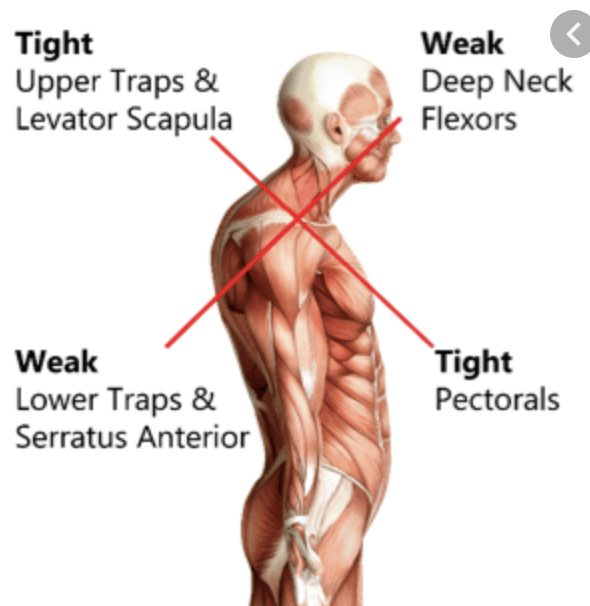
700
What about the orientation of the facets between C1 and C2 allow for that huge amount of pure rotation?
Superior Facet of C2 is almost completely horizontal
(the orientation of segments further down are angled and therefore sidebending and rotation are difficult to separate)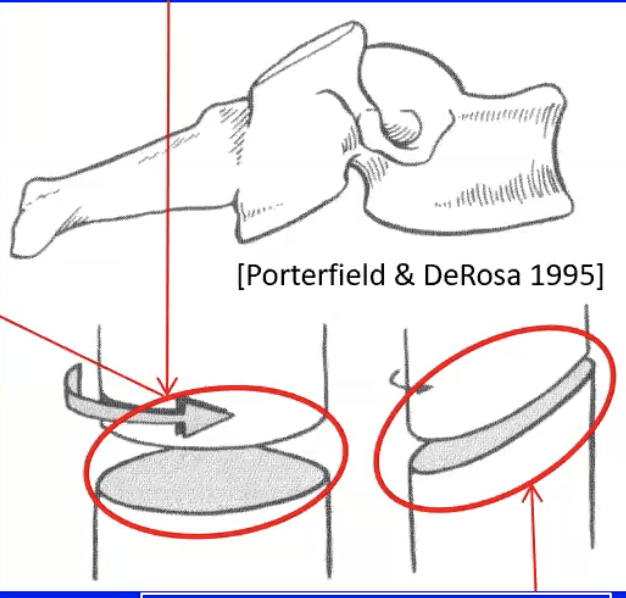
700
What are the 2 most important distinguishing diagnostic criteria according the Child's Classification for the Reduce Headache group?
Pain starts in neck and proceeds to fronto-ocular area
Unilateral Headache
700
What is the CPR used to predict success with Traction Intervention?
1. age > 55
2. (+) Neck Distraction Test
3. (+) Shoulder Abduction Test
4. (+) ULTT-A
5. Peripheralization with PA @ C4 - C7
(if at least 4 are present = rule in traction intervention)
800
Name the Red Flag: A patient presents to PT s/p MVA with resultant neck pain. He complains of feeling like his head is unstable and throwing him off balance. As you ask the patient to lie down for a part of the physical exam, but he absolutely refuses to unless he can have a pillow under his head. His most prominent exam finding is significantly decreased cervical flexion with worsening of symptoms.
Cervical Instability
800
What is the NEXUS Low Risk Criteria? (Name at least 2)
No Posterior Midline C Spine Tenderness
No Evidence of Intoxication
Normal Level of Alertness
No Focal Neurologic Deficits
No Painful Distracting Injuries
800
What 3 structures reside in the costal groove?
Intercostal Vein
Intercostal Artery
Intercostal Nerve
800
Given the actions of the sternocleidomastoid, how would you position your patient's head for an SCM stretch?
Contralateral Side bend
Ipsilateral Rotation
(along with chin tuck, cervical extension, and clavicular depression)
800
Quick! Doug sneaks up on you while you are desribing osteokinematics of the cervical spine and asks you to demonstrate with your hands the actions of the occiput on the atlas during flexion, extension, sidebending, and rotation
(demo on camera)
800
According to the OMPT, what are the agreed upon criteria for clinical instability/neck pain with movement coordination deficits? (Name at least 2)
Intolerance of Prolonged Static Postures
Better w/ External Support
Frequent Need for Self-Manip
Feelings of Instability/Shaking/Lack of Control
Frequent Episodes of Acute Attacks
Sharp Pain (often w suddent movements)
800
What is an effective test in order to isolate where in the C spine your patient's symptoms are being caused?
Craniocervical Flexion Rotation Test