Pathophys That Gets Your Pressure Up
The Great Kidney Detective
Contrast and Effect
License to Stent
Return of the Bypass
Fast and Fibromuscular
Aorta Know Better
100
Angiotensin II acts on the adrenal cortex to stimulate secretion of this hormone.
What is aldosterone?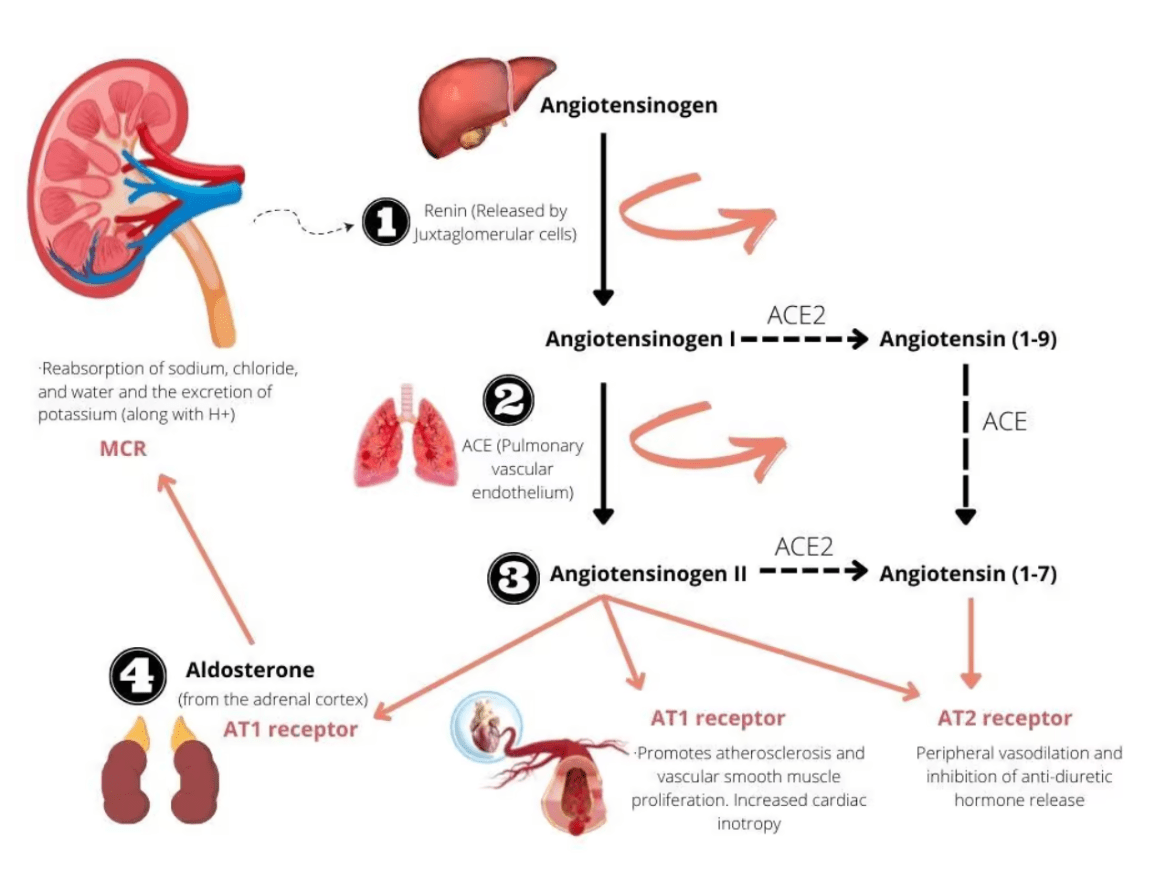
100
ACE inhibitor leading to acute kidney failure hints at this underlying anatomy/process?
What is bilateral RAS or a solitary functioning kidney with RAS?
100
This modality is the gold standard for diagnosing RAS.
What is digital subtraction angiography (DSA)?
100
Flash pulmonary edema in bilateral RAS is an indication for this therapy.
What is renal artery revascularization?
100
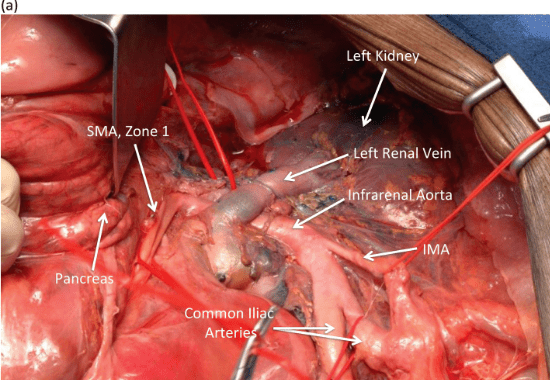
Name two possible sources for inflow for renal artery reconstruction.
What are the infrarenal aorta, supraceliac aorta, hepatic artery, splenic artery, or iliac vessels?
100
First‑line treatment for renovascular hypertension due to FMD.
What is balloon angioplasty without stenting?
100
The renal arteries originate from this segment of the aorta at approximately which vertebral level.
What is the abdominal aorta at the level of L2?
200
Angiotensin I is converted to the active vasoconstrictor angiotensin II by this enzyme - and it's found in highest concentration where.
What is angiotensin-converting enzyme (ACE), mainly in the pulmonary endothelium?
200
Before diagnosing renovascular hypertension, you must exclude this hormonal mimic.
What is primary hyperaldosteronism?
200
On duplex, RAR greater than this value indicates greater than 60% stenosis?
What is RAR>3.5?
200
A 70‑year‑old man has asymptomatic 50 % unilateral renal artery stenosis incidentally found on angiography during an aortic stent graft. What is the appropriate management?
What is no intervention—optimize medical therapy and monitor blood pressure and renal function?
200
The renal artery that usually originates from a more posterolateral position on the aorta.
What is the left renal artery?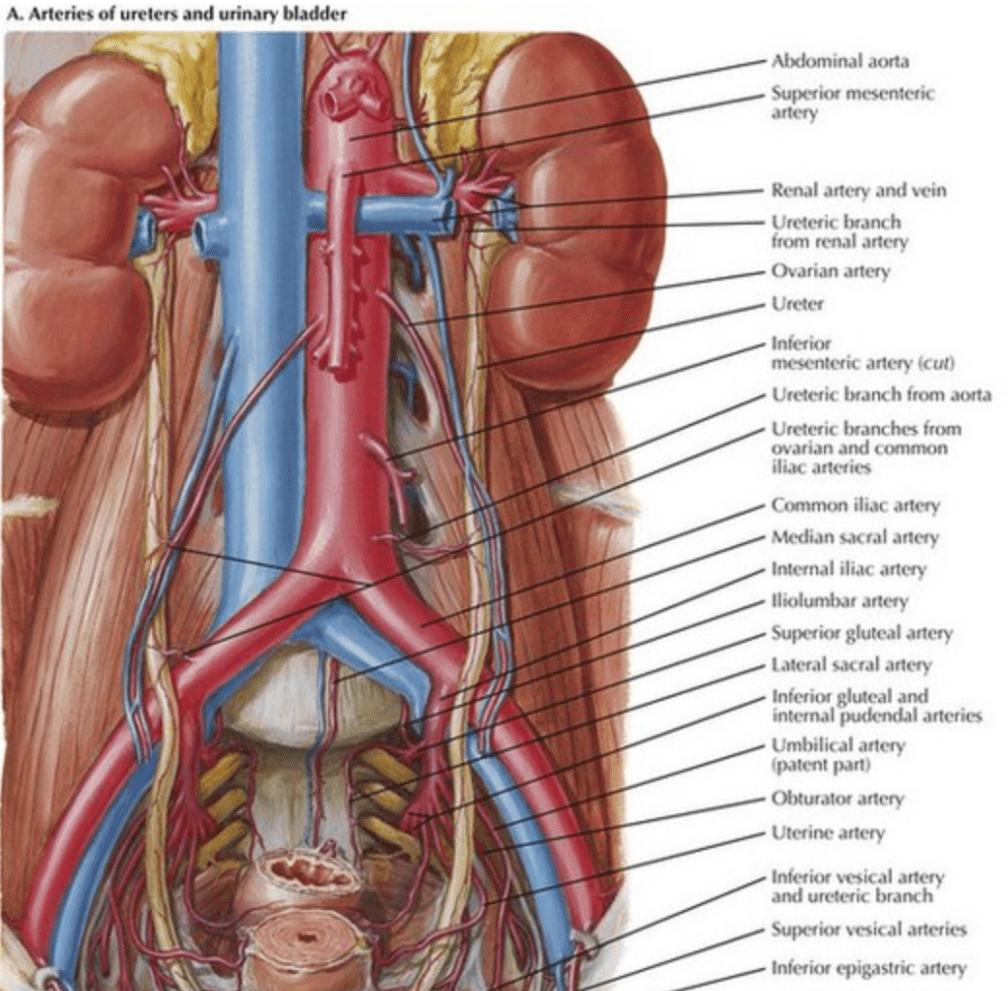
200
These three extrarenal arteries commonly show FMD manifestations.
What are coronary, carotid, and cerebral arteries?
200
To gain exposure of the left renal artery and supraceliac aorta for a splenorenal bypass, what named maneuver must you perform in order to gain adequate exposure? Which peritoneal attachments are divided first?
What is the Mattox maneuver (left medial visceral rotation)? What are the white line of Toldt and splenorenal and phrenicolic ligaments?
300
A 55-year-old woman with newly diagnosed hypertension starts an ACE inhibitor and her creatinine doubles within a week. Duplex demonstrates bilateral RAS. Why did her kidney function deteriorate?
What is reversal of angiotensin II-mediated efferent arteriolar constriction, dropping glomerular filtration pressure across both kidneys?
300
An intrarenal resistive index (RI) > 0.8 implies what two clinical points about kidney status and treatment response?
What is parenchymal damage and poor expected BP or renal function improvement after revascularization?
300
A 45‑year‑old woman with hypertension undergoes DSA. Images reveal multiple focal dilations separated by narrowing along the mid‑renal artery. How would you describe these findings?
What is a classic “string‑of‑beads” appearance consistent with fibromuscular dysplasia?
300
Restenosis after stenting most often occurs within this postoperative window.
What is approximately the first 6–12 months?
300
While preparing a hepatorenal bypass, your exposure through the hepatoduodenal ligament reveals a small artery left of the common bile duct. Which vessel have you identified? Once this vessel is dissected, through which anatomic route is the graft passed to reach the right renal artery?
What is the hepatic artery? What is behind the duodenum (posteriorly in a retroduodenal tunnel)?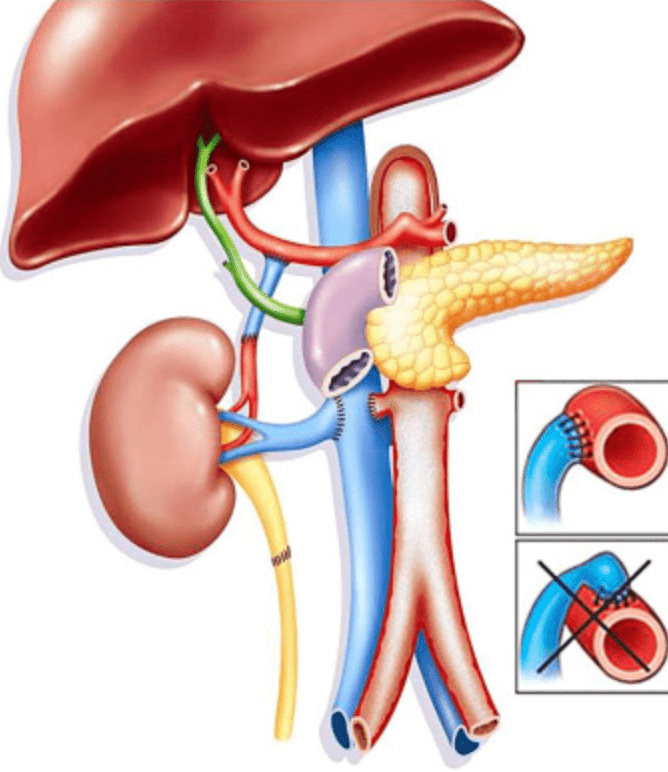
300
Stenting is avoided in FMD because of these two key reasons.
What are young patient age and high restenosis rates?
300
The left renal vein receives drainage from these two additional veins before entering the IVC.
What are the left gonadal and left adrenal veins?
400
A 63 year old woman with unilateral RAS has normal creatinine but significant left ventricular hypertrophy on Echo. What pathophysiologic pathway links the renal artery stenosis to her cardiac remodeling?
What is chronic angiotensin II driven vasoconstriction and afterload increase, stimulating myocardial hypertrophy and fibrosis?
400
You perform a renal vein renin assay and obtain these results: right = 12 ng/mL/h, left = 4 ng/mL/h, IVC - 6 ng/mL/h. Which kidney is diseased, and what ratio supports intervention?
What is the right kidney (right : IVC ≈ 2 : 1 > 1.5), indicating a functionally significant right renal artery stenosis?
400
A 66‑year‑old woman’s CTA shows bilateral 50 % stenoses. You’re uncertain if they’re physiologically significant. These two complementary studies can help determine if the lesions cause functional flow limitation.
What is a captopril renal scan or a renal vein renin assay to assess physiologic significance?
- During a captopril renal scan, angiotensin I–converting enzyme is inhibited, causing an acute decrease in angiotensin II, leading to constriction of the efferent arteriole and a decrease in the GFR. The test is positive when the GFR ratio between sides is increased to greater than 1.5:1.
400
A 60‑year‑old man undergoes successful right renal artery stenting. Two months later, his BP rises and follow‑up duplex reveals PSV = 260 cm/sec across the stent. What is the likely diagnosis and management?
What is in‑stent restenosis; manage with repeat balloon angioplasty or possible re‑stenting if flow‑limiting?
400
During exposure of the left renal artery, your assistant complains of bleeding from a small posterior vessel entering the left renal vein. This vessel is often injured during dissection.
What is the lumbar branch of the left renal vein?
400
Open surgery is reserved for these select patients with FMD.
What are those with endovascular complications (aneurysm, thrombosis, dissection) or failed angioplasty?
400
Following a Cattell–Brasch maneuver, you palpate the infrarenal aorta but still cannot identify the right renal origin due to dense retroperitoneal tissue. This additional maneuver will allow for further exposure of the renal hilum.
What is complete Kocherization of the duodenum?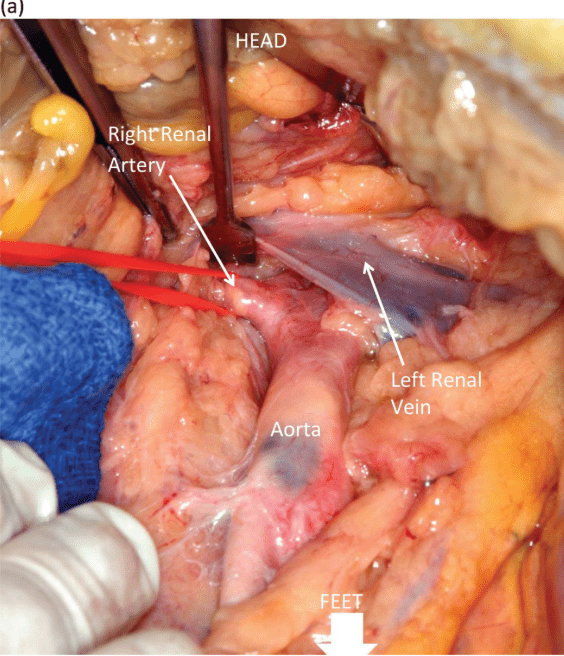
500
Renin is produced by these cells.
What are the juxtaglomerular cells?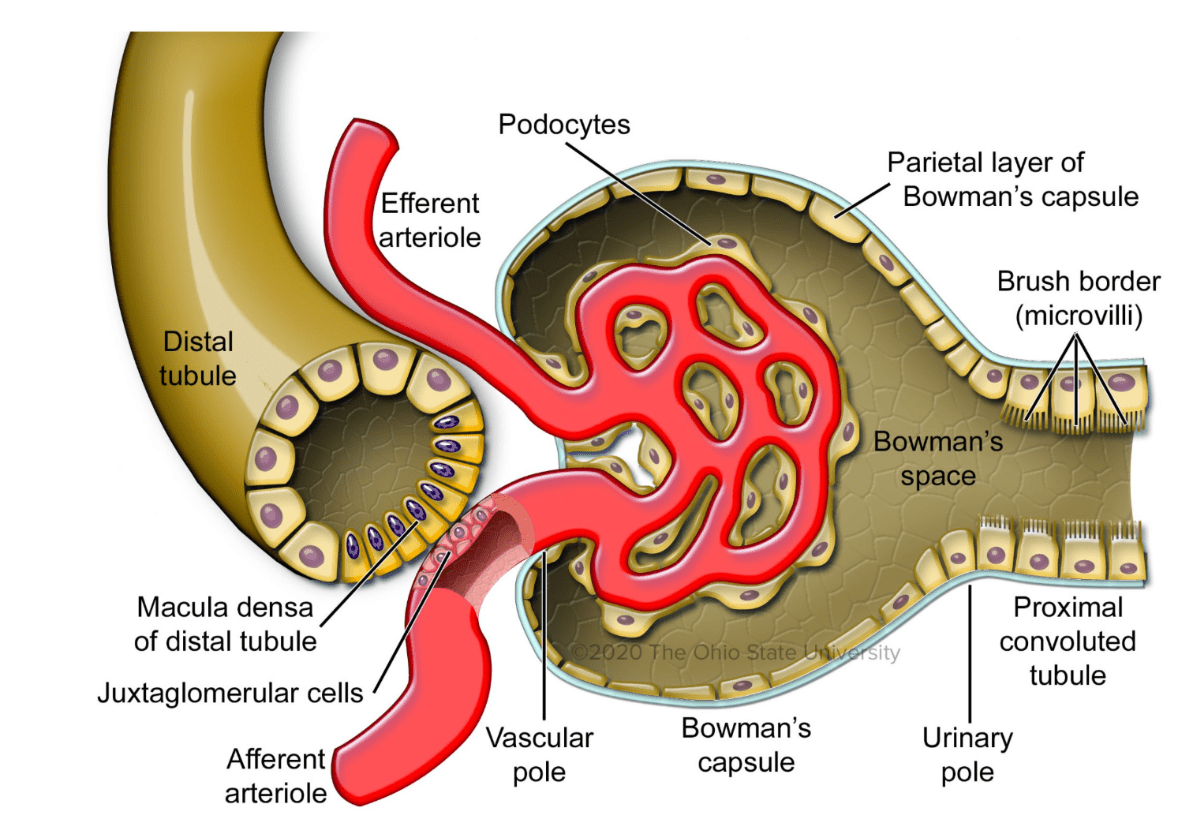
500
A 65‑year‑old man’s captopril renal scan shows a marked delay in cortical uptake and excretion on the right kidney after ACE inhibition. Interpret the physiologic mechanism behind this finding.
What is loss of angiotensin II–mediated efferent arteriolar constriction in the stenotic right kidney, reducing its GFR during ACE blockade?
500
During intra‑arterial DSA, you measure a peak systolic gradient of 25 mm Hg across a renal lesion. How should this gradient be interpreted?
What is a hemodynamically significant stenosis (≥ 20 mm Hg systolic or 10 mm Hg mean)?
500
You are considering renal artery stenting in a patient with unilateral 70 % stenosis, refractory hypertension, and a 6 cm kidney. According to AHA guidelines, how appropriate is intervention?
What is rarely appropriate—the kidney is likely non‑viable (< 7 cm) and unlikely to benefit from revascularization?
500
A patient undergoing right hepatorenal bypass has been systemically heparinized. Before completing the distal anastomosis, the team administers IV mannitol. The purpose of this step is to achieve this physiologic effect.
What is protection of renal function by osmotic diuresis and free radical scavenging?
500
Following revascularization for renal FMD, this schedule is used for duplex ultrasound surveillance.
What is immediately post‑procedure, every 6 months for 2 years, then annually if stable?
500
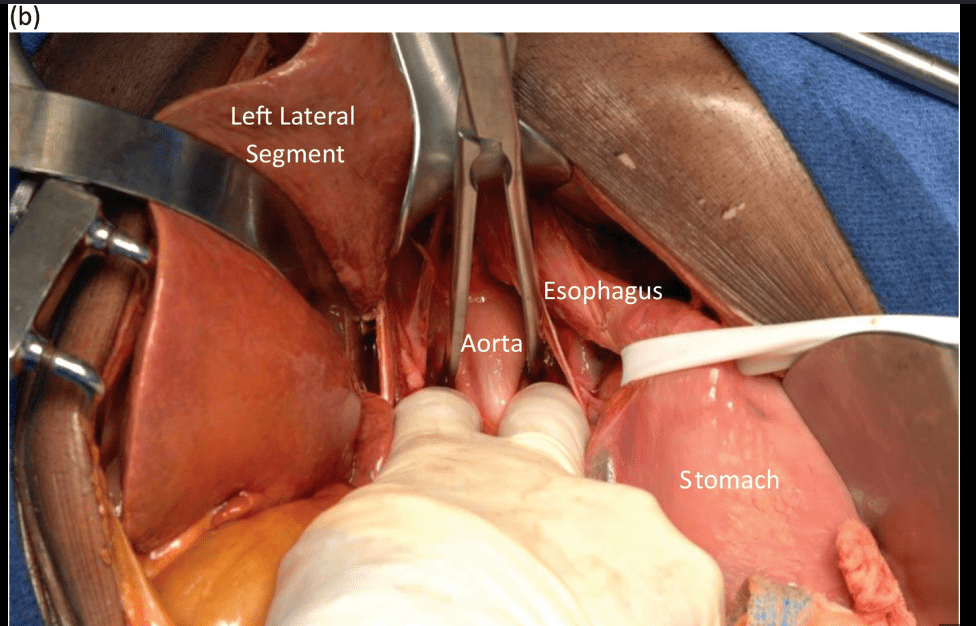
During a transaortic thromboendarterectomy for bilateral ostial RAS, you recognize that medial visceral rotation offers safer proximal control. Which side’s rotation provides quicker access to the suprarenal aorta? What other ligaments must be divided?
What is the left (Mattox) approach and the median arcuate ligament, left triangular ligament, and gastrohepatic ligament?