Nephrotic Syndrome
Nephritic Syndrome
Mixed Bag
GI Bleeding Part 1
GI Bleeding Part 2
100
This level of proteinuria defines nephrotic syndrome.
>3.5 g/day
100
Hematuria, hypertension, and AKI with less than 3.5 g/day proteinuria
Nephritic syndrome
100
“Frothy urine” is caused by this process
Proteinuria
100
First step in management of GI bleed
Stabilization (ABCs)
100
Another name for Black tarry stool
Melena
200
Most common nephrotic syndrome in children; associated with recent infection and podocyte effacement
Minimal change disease
200
Occurs 2–4 weeks after strep infection with low C3 and “lumpy bumpy” deposits
Post-streptococcal glomerulonephritis
200
“Tram-track” GBM appearance
Membranoproliferative glomerulonephritis (MPGN)
200
Type of IV access needed
Two large-bore IVs
200
Elevated BUN/Cr ratio suggests this
Upper GI bleed
300
Nephrotic disease associated with HIV and sickle cell disease; shows segmental sclerosis.
ocal segmental glomerulosclerosis (FSGS) 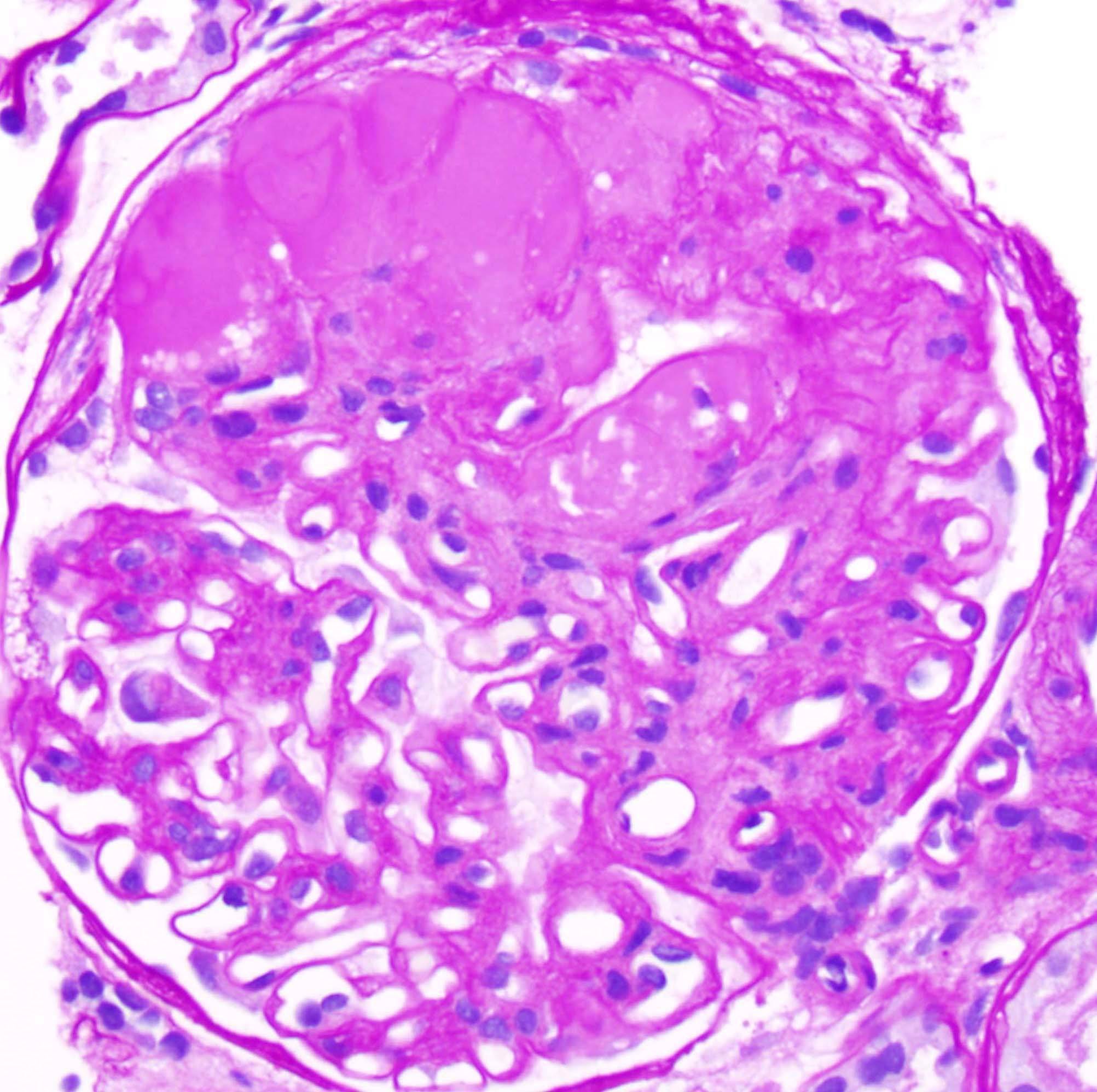
300
Hematuria shortly after URI or GI infection with normal complement levels
IgA nephropathy
300
A patient with active GI bleeding is normotensive and not tachycardic but is on a chronic medication that blunts the expected physiologic response.
Beta blocker
300
Medication for suspected variceal bleed
Octreotide
300
A patient with hematemesis after a night of heavy alcohol use and repeated vomiting
Mallory-Weiss tear
400
Associated with anti-PLA2R antibodies and “spike and dome” appearance.
Membranous nephropathy
400

Rapidly progressive glomerulonephritis (RPGN)
-Leads to rapid kidney failure with crescents on biopsy; includes ANCA vasculitis.
400
After initial stabilization of a patient with upper GI bleeding, endoscopy should generally be performed within this time frame.
24 hours
400
Massive transfusion ratio
1:1:1 (PRBC:platelets:FFP)
400
This lesion is a dilated submucosal artery that can cause brisk bleeding with minimal mucosal defect
Dieulafoy lesion
500
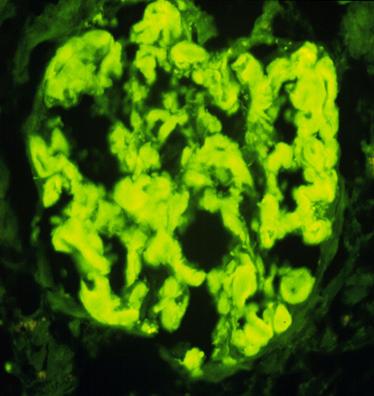
Amyloidosis
500
Hematuria, hearing loss, and eye abnormalities due to type IV collagen defect
Alport syndrome
500
A rising BUN out of proportion to creatinine in a patient with GI bleeding is due to this mechanism.
Digestion and absorption of blood proteins
500
Procedure for refractory variceal bleeding
TIPS
500
A cirrhotic patient presents with hematemesis and hypotension. In addition to resuscitation and octreotide, this class of medication must be started early to reduce mortality.
Ceftriaxone