Penicillin me softly
SOB stories
Murder on the Orientation Express
Urine trouble
What's Pneu
200
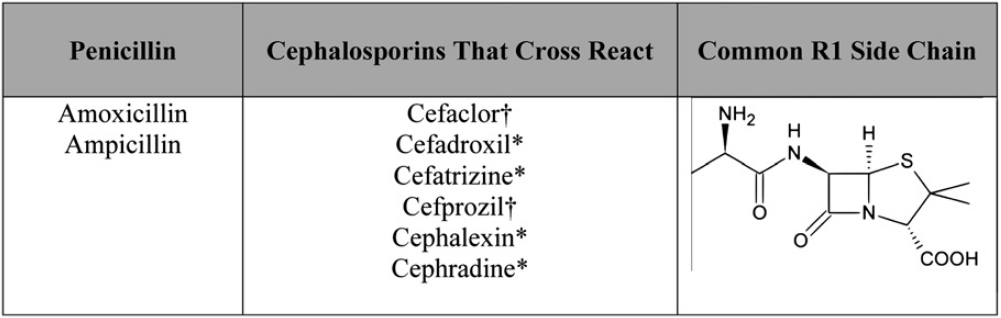
Draw the portion of penicillin the cross reacts with beta lactams
R
200
Why do you target an SpO2 > 88% rather than 92% in patients with COPD?
Hypoxic pulmonary vasoconstriction OR Haldane effect
NOT hypoxic drive
200
When can you go over cap?
Bouncebacks
200
This imaging is required to diagnose pyelonephritis
None!
200
Interpret this ABG:
Ph 7.3, PCO2 80, PO2 100, Bicarb 28
Acute Respiratory Acidosis (partially compensated)
Acute: Bicarb rises by 1/10 CO2
Chronic: Bicarb rise by 1/2.5 CO2

400
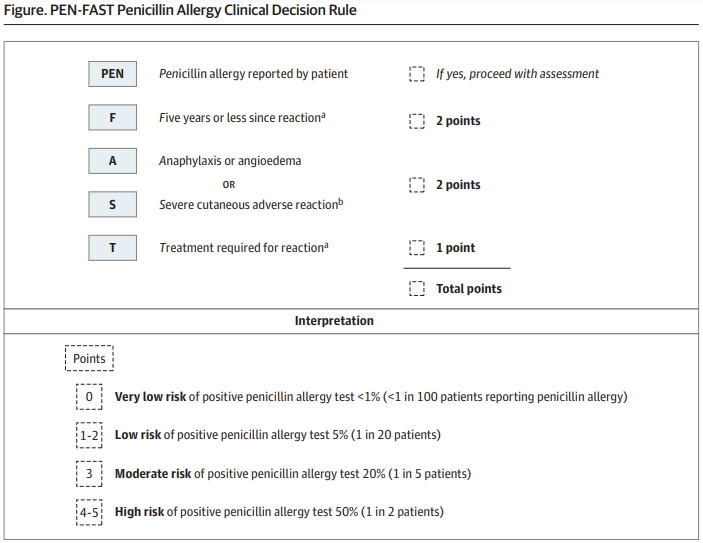
If my patient reports a penicillin allergy, I will use this clinical decision rule to evaluate their risk of positive penicillin allergy test
400
Name 2 contraindications to non-invasive positive pressure ventilation
Can't protect the airway
High aspiration risk
Concern for C-spine injury or recent surgery
400
When does individualized pre-rounding start?
September
400
You should get a renal ultrasound over a CT A/P for evaluation of pyelo in this patient population
What are pregnant patients?
400
Name 2 reasons for a falsely low procalcitonin in a true bacterial infection
Immunocompromise
Closed-space infection (abscess, empyema)
Intracellular bacteria - legionella, mycoplasma etc
600
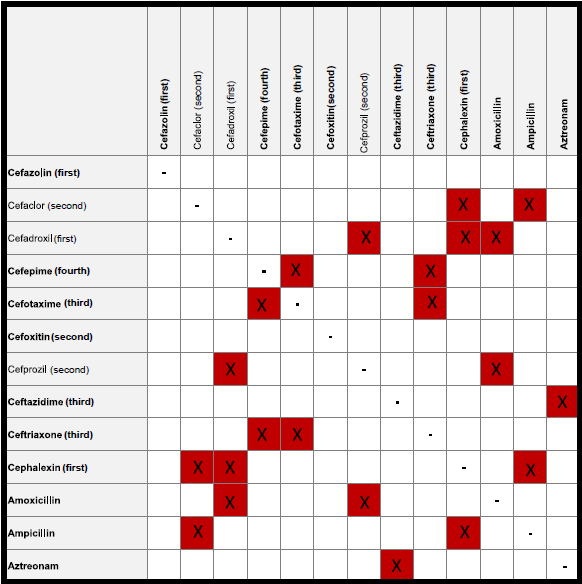
Name 3 cephalosporins that do NOT cross react with penicillin
600
Name two mechanisms by which positive pressure ventilation improves oxygenation in acute decompensated heart failure.
Preload reduction (reduces pulmonary capillary hydrostatic presssure, reducing worsening of pulm edema)
Prevention of alveolar collapse at end-expiration (incresed FRC)
Decreased LV afterload (increased intrathoracic pressure reduces transmural pressure, which reduces LV strain)
600
Who does a bounce-back admission, and at what time does it change?
Floor team that was caring for pt before 1 PM
PRAT after 1 PM
600
This is the first line treatment (with duration) for acute complicated UTI in the outpatient setting
Ciprofloxacin 500mg BID for 5-7 days
OR
Levofloxacin 750mg daily for 5-7 days
600
According to the IDSA, when is it appropriate to cover for anaerobes in suspected aspiration pneumonia?
Why has this changed?
Abscess/empyema.
Newer data shows low prevalence of anaerobic infections, possibly due to demographic shifts/better dentition.
800
You have 30 seconds to pull up the beta lactam cross reactivity chart on your phone
Residency Files -> Helpful Links -> ID Resources
800
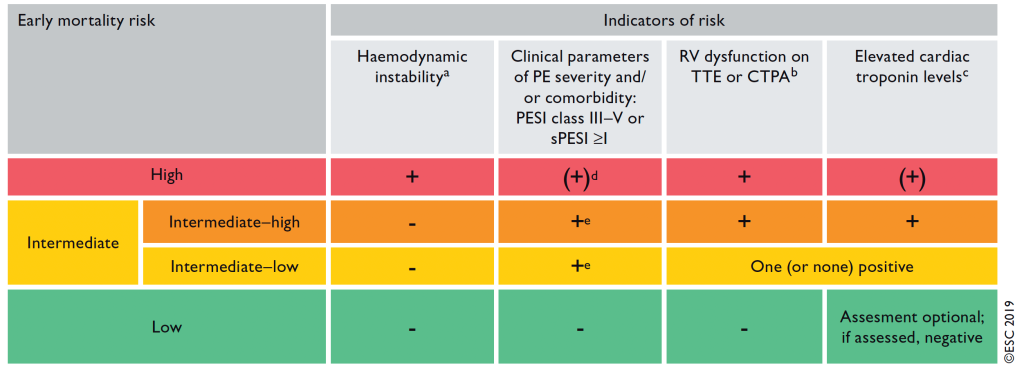
What three things make a pulmonary embolus intermediate-high risk?
Who should you involve with most pulmonary emboli when at PMPMC?
Elevated PESI/high risk comorbidities
Signs of RHS on echo/CTA
Elevated troponin
PERT - Pulm embolus response team - have been shown to decrease mortality
800
What are the time frames that dictate who you staff new admissions with on PRAT.
Before 3pm: Present to attending for the team patient is going to
3-6pm: Attending on Call (expected to see patient that day)
After 6pm: Attending on Call (see schedule. Different on Thurs/Fri)
800
What changed in the IDSA guideline definition of complicated UTI?
Redefined by where the infection is and how systemic it is, not by who the patient is
Any infection extending beyond the bladder is complicated
Male, pregnant, diabetics, immunocompromised patients are no longer automatically complicated
800
What are the three most common sites for nocardia infection?
Lung, brain, skin (in that order)


1000
Monobactams (aztreonam) does not cross react with cephalosporins EXCEPT this one
ceftazidime
1000
On BIPAP/Ventilator which parameters most impact
Ventilation (3) and
Oxygenation (2)
Ventilation - Minute ventilation (AKA RR x Tidal Volume), IPAP-EPAP
Oxygenation - FiO2, EPAP
1000
What is the process for punting admissions to ADS?
Call your attending
Have your attending talk to ADS attending
1000
What are the three antibiotics to treat simple cystitis if you are concerned about MDR organisms?
Nitrofurantoin
Fosfomycin
Pivmecillinam
1000
Empiric treatment and treatment duration for isolated pulmonary nocardia infection
Bactrim + imipenem/amikacin/ceftriaxone/cefotaxime
6 months