Gastro
General IM
Cardiology
Pulmonology
ID
100
45-year-old female presenting with gradual onset of fatigue, itchy skin, jaundice and melanin hyperpigmentation of the skin, hepatomegaly. Labs show elevated ALP, GGT and TB. Normal AST and ALT. Positive antimitochondrial antibodies. History of smoking. What is a diagnosis?
Primary biliary cholangitis (accept primary biliary cirrhosis)
100
Patient with T2DM, HTN and stable systolic dysfunction is prescribed naproxen to control her osteoarthritis pain in his hands. Within 2 weeks, he develops:
- New onset weight gain
-Paroxysmal nocturnal dyspnea
- Orthopnea
- Lower extremity edema
Heart failure exacerbation due to NSAIDs
100
Patient with history of MI presents with days to weeks of:
-Fatigue
-Recurrent chest discomfort
-Fever
-Leukocytosis
-Pericardial friction rub
CXR: increased cardiac silhouette
Dressler Syndrome
-DX: clinical + echo
-Tx: Aspirin + Colchicine; short course systemic steroids for refractory cases
100
What’s the Diagnosis?
Patient admitted to coronary care unit s/p acute MI with right internal jugular central venous catheter. On arrival to unit develops:
- Chest pain, dyspnea, and confusion
- Decreased BP with decreased in SBP >10mmHg with inspiration
- Tachypnea
- Distended neck veins
- Diminished breath sounds on the right
- CXR: Shift of mediastinum to left
Tension Pneumothorax
100
Middle aged patient presents with several weeks history of fever, arthralgias, new diastolic murmur at the right upper sternal border. Blood cultures show Streptococcus gallolyticus. Echo showing large vegetation on the aortic valve.
What additional study should the patient receive?
Colonoscopy
20-30% chance of having colon cancer
200
Older patient with multiple diverticula presents with bloating, watery diarrhea, dyspepsia and weight loss. Labs show macrocytic anemia, high folate and vitamin K, low B12, low vitamin D. DEXA scan showed T-score less than -2.5. UGI with SBFT showed delayed motility. Lactulose breath test is abnormal with early rise in hydrogen production. What is the diagnosis
Small intestinal bacterial overgrowth (SIBO)
200
Healthy patient presents after working outdoors for hours with acute onset of lacrimation and salivation, miosis, vomiting, urination, bradycardia, fasciculations, motor weakness and bronchospasm. What is a diagnosis
Organophosphate poisoning
DX: Clinical +/- Empiric Atropine 1 mg (reverses sxs)
Tx: decontamination if topical exposure + respiratory support + atropine injections
200
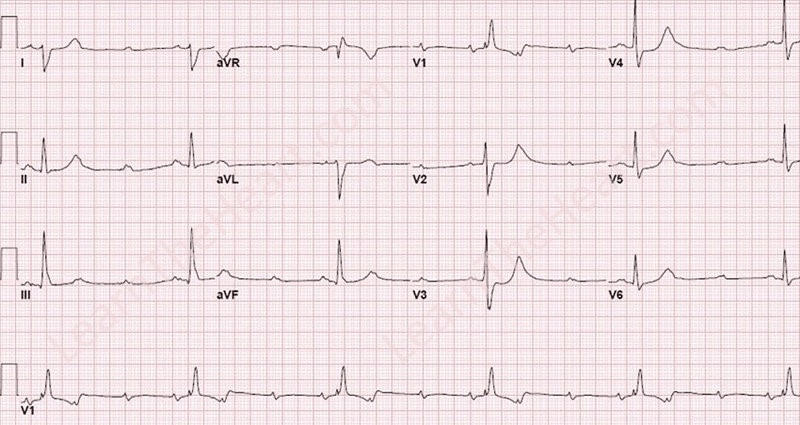
What’s the Diagnosis?
A male patient with known bicuspid aortic valve presents with:
- Increased BP in arms
- Diminished femoral pulses
- Decreased BP in the lower extremities
- ECG: LVH
- CXR:
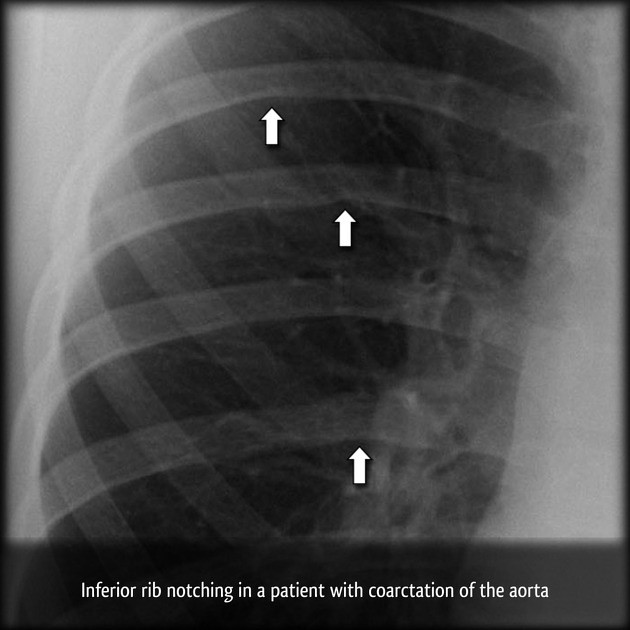
Coarctation of the Aorta
200
Young patient with PMH of recurrent sinusitis, pneumonia presents with chronic exertional dyspnea, cough with purulent sputum. Sputum Gram stain: Gram-positive cocci in clusters and gram-negative rods. Sputum gross Staphylococcus aureus. What is the diagnosis?
Cystic Fibrosis
200
Older, hospitalist, diabetic patient with history of heart failure presents with fever, cough, confusion, hypoxemia. CXR showing lobar consolidation. Blood culture showing gram-positive cocci in chains. Sputum Gram stain and culture showing gram-positive cocci in lung chains.
What is the etiology (organism) of the pneumonia?
Group B streptococci (GBS) or Streptococcus agalactiae
now recognized as the bonafide etiology of severe pneumonia in older patients with unique features: high rate of coexisting bacteremia, often with confusion, and predilection for hospitalized patients with hx of HF or DM
300
40-year-old male presents with recurrent duodenal ulcers, diarrhea, retrosternal burning, weight loss. Serum gastrin is > 1000 pg/mL (normal 25–29 pg/mL). What is the diagnosis?
Zollinger-Ellison syndrome (ZES)
300
Patient presents with chronic nasal congestion, worse in the spring and fall. On exam swollen and beefy red nasal mucosa. What is the diagnosis?
Rhinitis medicamentosa
300
 Patient with history of coronary heart disease presents with:
Patient with history of coronary heart disease presents with:
- Recent onset lightheadedness and feeling as if “about to pass out”
- Decreased exercise capacity
- HR < 40
- No JVD
- Cannon a waves
- EKG: narrow QRS rhythm with dissociated, regular interval P waves
3rd Degree atrioventricular block (Complete heart block)
Key points:
- Cannon a waves = AV dissociation
- Narrow QRS means junctional escape in this case
- Tx: Pace maker
300
Patient with AML undergoing bone marrow transplant develops cough and dyspnea without fever. CBC ANC less than 500 for the past 14 days. CXR with no acute changes. HRCT of chest: Nodules with surrounding ground glass infiltrates (halo sign) or an air crescent sign or simple consolidation. What is the most likely diagnosis?
Invasive pulmonary aspergillosis
300
21-year-old sexually active female presents with vaginal discharge. She requests STI screening. Cervical swab is performed and PCR is positive for chlamydia and negative for Neisseria gonorrhea. What treatment and dose should be given?
Azithromycin 1g PO x 1 or
Doxycycline 100 mg PO bid x 7 days
or levofloxacin 500 mg daily x 7 days
Retest all individuals at 3 months not as test of cure but because of high rates of reinfection. Notify and treat sexual partner
400
Patient with lactose intolerance or anorexia presents with cheilitis, glossitis, low hemoglobin hematocrit with normal MCV and MCHC, and seborrhea. What is the diagnosis?
Riboflavin (B2) deficiency
400
Runner presents with gradual onset of pain and paresthesia between his 3rd and 4th toes with standing and walking, reproducible with palpation. What is the diagnosis?
Morton Neuroma
Dx: Mulder sign = clicking evidence when squeezing with metatarsal joints and palpating the interdigital space
Tx: shoe inserts, strength exercises
400
What’s the Diagnosis?
A patient who injects drugs presents with 1-week history of:
- Fever, cough and pleuritic chest pain
- Abdominal pain and fullness
- Increased JVP, more marked with inspiration; prominent jugular “v waves”
- Faint holosystolic murmur at midsternum
- Pulsatile hepatomegaly
- Lower extremity edema
- CXR: diffuse nodular pulmonary infiltrates
Tricuspid endocarditis causing tricuspid regurgitation
400
Patient presents 2 years after major inhalation exposure to pool chemicals with chronic productive cough for months to years. PE: Crackles at the bases. Sputum Gram stain: Multiple gram-positive and gram-negative organisms. Sputum culture: Gram-negative enterics including Proteus. What is the diagnosis?
Bronchiectasis
400
Several patients who swim at the same local swimming pool developed acute, self resolved pain, watery diarrhea, crampy abdominal pain. Stool O&P: No ova or parasites. Stool modified acid-fast: 4 to 6 micrometer pink cysts. What is the Diagnosis?
Cryptosporidium
Tx: immunocompetent - not needed.
ART for HIV/AIDS
Nitazoxanide if therapy is needed.
500
Health-conscious patient who takes multiple medical vitamins and supplements presents with alopecia, diffuse myalgia and bone pains, ataxia and hepatosplenomegaly. What this is the diagnosis?
Chronic Vitamin A overdose
500
Patient in his 30s develops long history of anxiety and agitation with poor social relationships, rapid involuntary movements, declining problem-solving skills and poor orientation to goals, intact memory. What is the diagnosis?
Huntington Disease
500
Patient with history HLD, HTN is admitted for inferior STEMI. He receives fibrinolytics. on Day 3, he develops:
-Acute Dyspnea
-Low BP
-Bilateral rales + JVD
-Hyperdynamic precordium with new systolic murmur at apex
Papillary Muscle Rupture
DX: Echo
TX: Surgery after medical stabilization (afterload reduction + IABP or inotrope)
500
Young male from southern state who frequently walks barefoot during the summers presents with 5 days of fever, dry cough and chest discomfort. Leukocytosis with eosinophilia. Sputum: Charcot-Leyden crystals. CXR: Migrating pulmonary infiltrates. Which is a diagnosis?
Loffler syndrome
500
Patient with known he malignancy and a central venous catheter presents with fever, blood cultures from catheter showing gram-positive rods, identified as Corynebacterium jeikeium. What drug should be prescribed?
IV Vancomycin
-the only effective treatment for C. jeikeium.