Shape Shifter
Clues in the History
After Hours
Timing is Everything
Collateral Damage
100
A 56-year-old man with uncontrolled diabetes comes to ER with:
severe unilateral facial pain
headache
fever
nasal congestion with bloody discharge
swelling around the left eye + diplopia
See the picture .
Question
What is the immediate management?

mucormycosis
Start IV Liposomal Amphotericin B immediately
Urgent ENT + Ophthalmology consult
Emergency surgical debridement ( do not delay
100
A patient presents with rapidly progressive cellulitis within 24 hours after a cat bite.
Gram stain shows gram-negative coccobacilli.
Most likely organism?
Pasteurella multocida
100
A 55-year-old man is admitted for elective cholecystectomy.
He is: Afebrile , BP and HR stable
No chills or rigors , No central line
Normal oxygen saturation
Blood cultures were taken in ED because of mild leukocytosis.
At 2:30 a.m., the microbiology lab calls you:
“One blood culture bottle is positive. Gram stain shows gram-positive cocci in clusters. The organism has been identified as Staphylococcus aureus.”
The patient is clinically stable and only one blood culture bottle is positive.
What will you do next?
Start empiric IV antibiotics immediately
Because Staphylococcus aureus is never a contaminant.
Empiric choice
IV Vancomycin
Covers MRSA + MSSA until sensitivities are available.
Repeat blood cultures
Take 2 new sets from different sites before or soon after antibiotics
100
A 42-year-old man, 2 months post renal transplant, presents with:,Fever for 5 days
Fatigue, malaise ,No urinary symptoms ,No cough, no diarrhea
Creatinine slightly rising
Vitals: T 38.4°C BP stable
Labs: WBC low (3.0 ×10⁹/L) ,Platelets low ,Mild transaminitis
Urine analysis: clean
Blood cultures: pending
CXR: normal
What is the MOST likely infection?
CMV infection / CMV disease
100
When to hold anti tb ?
•patient with symptoms of hepatitis:
Stop all TB drugs and perform LFTs:
a) AST or ALT or bilirubin ≥ 3 times upper limit of normal (ULN): wait for resolution of symptoms, perform LFTs weekly and restart TB treatment when LFTs are < 3 times ULN.
b) AST, ALT and bilirubin < 3 times ULN and mild symptoms (no jaundice): restart TB treatment, closely monitor the patient and perform LFTs weekly. Continue TB treatment as long as LFTs levels remain < 3 ULN and there are no signs of worsening hepatitis.
•Patient without symptoms of hepatitis, but elevated LFTs:
a) AST or ALT ≥ 5 times ULN or bilirubin ≥ 3 ULN: stop all TB drugs and perform LFTs weekly. Restart TB treatment when LFTs return < 3 times ULN.
b) AST and ALT < 5 times ULN and bilirubin < 3 ULN: continue TB treatment and perform LFTs weekly
200
What the indication to start Anti fungal in febril neurtorpenia
Empirical antifungal therapy and investigation for invasive fungal infections should be considered for patients with persistent or recurrent fever after 4–7 days of antibiotics
200
A 42-year-old butcher in Saudi presents with painless skin lesion on the hand after slaughtering animals. Started as a papule → vesicle → now a black eschar with massive surrounding edema. He is afebrile.
Question
What is the most likely diagnosis and immediate management?
Diagnosis: Cutaneous anthrax ( bacillus anthrax )
Immediate management:
Start antibiotics immediately (don’t wait for culture)
Ciprofloxacin PO or Doxycycline PO
If systemic signs / extensive edema / face/neck involvement → IV Ciprofloxacin + additional agents (e.g., clindamycin/linezolid) + consider antitoxin if severe
Dx confirmation: swab from lesion for culture/PCR, blood cultures if systemic
Key clue: painless black eschar + huge edema + animal exposure/
200
70-year-old man is admitted under orthopedics for an elective total knee replacement planned for tomorrow.
He is:AfebrileHemodynamically stableNo dysuriaNo urinary frequency or urgencyNo suprapubic pain
No flank painNormal mental status
A routine pre-operative urine culture was sent on admission.
At 1:30 a.m., the orthopedic team contacts you and says:
“The urine culture result just came back.
It is growing an k. pneumonia XDR.
Orthopedics calls you and asked What abx to be started ?
Correct On-Call Approach (Stepwise)
Step 1: Assess the patient clinically
Personally review the patient
Confirm absence or presence of UTI symptoms
Step 2: Decision based on symptoms
If the patient is ASYMPTOMATIC
DO NOT start antibiotics
200
A 45-year-old man, renal transplant recipient, presents 6 months post-transplant for routine follow-up.
He feels well, with no fever, no dysuria, and no graft pain.
Labs show: Serum creatinine increased gradually from 105 → 165 µmol/L over 4 weeks
WBC normal , CRP normal
Urinalysis: No leukocytes ,No nitrites ,Mild proteinuria
Tacrolimus level: therapeutic
Urine culture: negative
Question:
What is the most likely diagnosis?
BK virus nephropathy
6 months post–renal transplant → peak time for BK virus
Gradual rise in creatinine (weeks, not days)
No fever, no pain, no dysuria → argues against infection
Normal WBC & CRP → not rejection or bacterial infection
Urine culture negative
Mild proteinuria → common in BK nephropathy
Tacrolimus level therapeutic → toxicity less likely
200
What abx well known to cause tendon rupture
Fluroquinolones
300
A 35-year-old HIV-positive man (CD4 40 cells/µL, not on ART) presents with 2–3 weeks of progressive headache, fever, and blurred vision. He has nausea and confusion but minimal neck stiffness.
CT brain is normal.
Lumbar puncture shows opening pressure 35 cm H₂O, lymphocytic pleocytosis, low CSF glucose, elevated protein, and positive cryptococcal antigen in CSF.
What is the management ?
Cryptococcal meningitis treated with urgent therapeutic lumbar punctures + amphotericin B and flucytosine, followed by fluconazole, with delayed ART initiation.
300
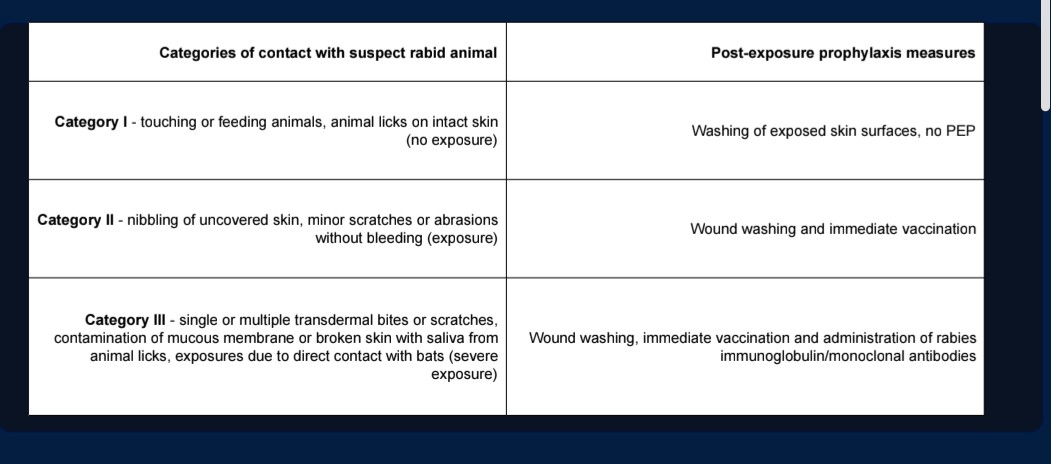
A 27-year-old man presents to the emergency department 2 hours after being bitten by a stray dog on his left leg.
The dog was unvaccinated and ran away.
The bite caused bleeding puncture wounds.
The patient has no prior rabies vaccination.
He is otherwise healthy.
Question
What is the Post-Exposure Prophylaxis (PEP) for rabies?
300
It’s 2:20 AM.
The ICU nurse calls you urgently.
Patient:60-year-old man Known ESRD on hemodialysis Has a tunneled dialysis catheter
Admitted with pneumonia, on IV antibiotics Now the nurse reports:
Temperature 39.4°C Blood pressure 85/50 mmHg
Heart rate 120 On vasopressors
Redness and purulent discharge around the catheter exit site
Blood cultures were just sent, results pending.
The nurse asks:
“Doctor, should we wait for cultures or adjust antibiotics?”
What is the most important step in management?
remove the lines
Source control comes first
Antibiotics alone are not enough.
300
A 55-year-old man underwent renal transplant 3 weeks ago.
He presents with: Fever ,Dysuria ,Suprapubic discomfort
Vitals are stable.
Urinalysis shows pyuria.
Creatinine is mildly increased compared to baseline.
Question:
What is the most likely infection in this patient?
Urinary Tract Infection
300
A neutropenic patient on broad antifungal therapy develops acute kidney injury, hypokalemia, and hypomagnesemia.
Which drug most likely caused this?
A. Voriconazole
B. Caspofungin
C. Fluconazole
D. Amphotericin B
Amphotericin B
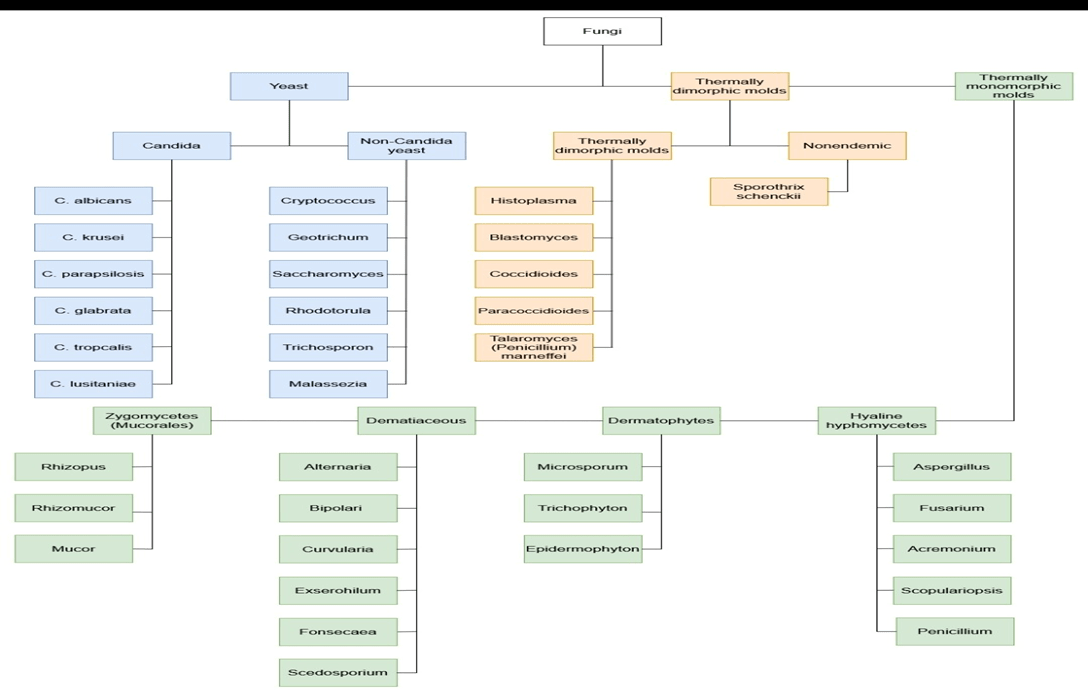
400
classification of fungi
400
32 years old male pt from jazan He works as a shepherd. Over the past week, several sheep on his farm died suddenly, and there has been a recent increase in mosquitoes after heavy rain.
On examination: Temperature: 39.7°C
Conjunctival injection Mild jaundice
No focal chest findings
Investigations Platelets: low
AST/ALT: markedly elevated
Bilirubin: elevated
Creatinine: rising
Malaria smear: negative
Blood cultures: negative
Most likey diagnosis ?
Rift Valley fever
Transmission
- Mosquito bites (Aedes, Culex)
- Direct contact with infected animals:
- Blood, tissues, aborted fetuses
- Slaughtering / handling livestock
- NOT human-to-human
Heavy rain → mosquito bloom → outbreaks
Fever + hepatitis + thrombocytopenia + livestock deaths after heavy rain = Rift Valley Fever
400
58-year-old man is admitted with suspected MRSA pneumonia and was started on IV vancomycin.About 20 minutes into the first vancomycin infusion, the nurse calls you urgently and reports: Sudden flushing and erythema over the face, neck, and upper chest
Patient complains of itching No shortness of breath
No wheezing No lip or tongue swelling Blood pressure: stable Oxygen saturation: 98% on room air
Question
What is the most likely diagnosis and how to prevent it
Red Man Syndrome
low the infusion rate
Infuse over ≥ 1–2 hours
400
A 52-year-old man, 7 weeks after orthotopic heart transplantation, presents with fever, fatigue, and worsening shortness of breath.
He is on tacrolimus, mycophenolate, and prednisolone.
Investigations show:
Mild leukopenia
Elevated troponin
Echocardiography: new global left ventricular dysfunction
Coronary angiography: normal
Endomyocardial biopsy: myocardial inflammation with intracellular protozoa
Question
What is the most likely diagnosis?
Toxoplasma gondii myocarditis
400
A 35-year-old man with a history of lung transplantation is receiving long-term antifungal prophylaxis. After several months, he develops severe photosensitivity, erythematous skin lesions on sun-exposed areas, and actinic damage despite minimal sun exposure.
Which antifungal agent is most strongly associated with this adverse effect?
A. Fluconazole
B. Itraconazole
C. Posaconazole
D. Voriconazole
E. Amphotericin B
D. Voriconazole
500
A 68-year-old man is in the ICU following abdominal surgery.
He has:
Central venous catheter
On broad-spectrum antibiotics for 10 days
Persistent fever
Blood cultures grow Candida species, reported by the lab as:“Candida haemulonii – identification uncertain”
What is the likely causative organism and your immediate management
Candida auris is frequently misidentified as Candida haemulonii by routine laboratory systems.
Candida auris
a. Antifungal therapy
•Start IV echinocandin
•e.g. Micafungin
b. Source control
•Remove central line
500
A 34-year-old man presents with 5 days of high fever, severe myalgia, and headache.
He reports: Recent swimming in flood water / freshwater ,Seen rats in the area ,No recent travel
On examination: Temperature: 39.2°C m Conjunctival suffusion (red eyes without discharge) ,Marked calf muscle tenderness ,Mild jaundice
Investigations ,Creatinine: elevated
Bilirubin: elevated ,Platelets: low
AST/ALT: mildly elevated (bilirubin disproportionately high)
Most likely diagnosis
Severe complication to watch for?
Leptospirosis
Weil disease
Leptospira interrogans, Thin spirochete Reservoir: rats (also dogs, cattle)
Spread via urine-contaminated freshwater
When to suspect :Acute fever + severe myalgia (calves)
Conjunctival suffusion (red eyes, no discharge)
Exposure to flood water / swimming / sewage AKI ± jaundice Platelets low
How to diagnose
serology MAT– most common
PCR in early disease
Cultures rarely used (slow)
Weil’s disease (severe leptospirosis)
jaundice + renal failure
500
You are the medical resident on call.
A 30-year-old nurse sustains a needle-stick injury during IV cannulation.
Source patient:
HBsAg positive
Anti-HCV positive
Exposed nurse:
Completed HBV vaccination
Anti-HBs status unknown
What will you do next?
Step 1: Immediate wound care
Wash with soap and water
Step 2: Check nurse’s immunity
Send anti-HBs titer
Step 3: HBV management
If anti-HBs ≥10 mIU/mL → NO action
If anti-HBs <10 or unknown →
Give HBIG
Start HBV vaccine booster
Step 4: HCV management
NO post-exposure prophylaxis exists
Baseline HCV Ab and ALT
Follow-up HCV RNA at 4–6 weeks
Early detection → early treatment
Key Exam Pearl HCV has NO PEP — only monitoring and early treatment
500
A 52-year-old man from Philippine underwent a renal transplant 1 month ago.
He is receiving tacrolimus, mycophenolate, and high-dose steroids.
He presents with:
Progressive shortness of breath and wheezing ,Watery diarrhea and abdominal pain
Fever and hypotension
Investigations show:
Chest X-ray: bilateral diffuse infiltrates
Blood cultures: Gram-negative bacteremia (E. coli)
CBC: no eosinophilia
Sputum examination: motile larvae
What is the most likely diagnosis
Strongyloides hyperinfection syndrome
Renal transplant + high-dose steroids → classic trigger for hyperinfection
From the Philippines → endemic exposure risk
Wheezing + diffuse lung infiltrates → pulmonary larval migration
Watery diarrhea & abdominal pain → intestinal invasion
E. coli bacteremia → larvae carry gut bacteria into bloodstream
Motile larvae in sputum → diagnostic of hyperinfection
No eosinophilia → expected in severe/disseminated disease (steroids suppress it)
500
A patient with confirmed MRSA pneumonia is switched to another anti-MRSA agent due to worsening renal function.
After 48 hours:
Hypoxia worsens
Inflammatory markers improve
Repeat cultures still show MRSA
Which antibiotic choice BEST explains this failure?
Explain your answer
A. Linezolid
B. Vancomycin
C. Daptomycin
D. Ceftaroline
C. Daptomycin
lung surfactant inactivates daptomycin