More Topics
Topics Cont.
Shock
Injuries
Even More Topics
100
When managing a patient with a central venous catheter (CVC), it's crucial to:
Assess the insertion site regularly for signs of infection like redness, swelling, drainage, or pain. Monitor for catheter dislodgement.
Maintain sterile technique when accessing the line or changing dressings to prevent infection. Use proper flushing techniques.
Ensure line patency by flushing per protocol and avoiding excessive force when flushing to prevent catheter rupture or air embolism.
Change tubing, caps, and connectors according to facility policy to limit bacterial growth.
Provide meticulous catheter site care and educate the patient on proper hygiene.
Report any signs of catheter dysfunction, occlusion, or suspected infection promptly.
Continuous monitoring and adherence to best practices are essential to prevent serious CVC-related complications like infection, thrombosis, or air embolism. Timely removal when no longer needed reduces risks.
100
How do you know if a PPI is working?
To know if a PPI is working effectively, look for improvement in symptoms like heartburn, regurgitation, and difficulty swallowing. Healing of esophageal inflammation or ulcers on endoscopy also indicates the PPI is adequately reducing acid. Adjustments may be needed if symptoms persist despite PPI therapy.
100
Types of shock
The main types of shock are:
1. Hypovolemic shock - caused by significant blood or fluid loss, leading to decreased circulating volume.
2. Cardiogenic shock - resulting from impaired cardiac output due to conditions like heart attack or heart failure.
3. Distributive shock - caused by abnormal distribution of blood flow, such as in sepsis, anaphylaxis, or neurogenic shock.
4. Obstructive shock - occurs when blood flow is obstructed, like in pulmonary embolism, cardiac tamponade, or tension pneumothorax.
Proper identification of the type of shock is crucial, as management strategies differ based on the underlying cause. Prompt treatment is essential to prevent cellular hypoxia, organ damage, and potential fatality.
100
Response to a heat injury
Heat Exhaustion
Prolonged exposure to heat over hours or days
Leads to heat exhaustion
Clinical syndrome characterized by
Fatigue
Light-headedness
Nausea/vomiting
Diarrhea
Feelings of impending doom
Tachypnea
Tachycardia
Dilated pupils
Mild confusion
Ashen color
Profuse diaphoresis
Hypotension and mild to severe temperature elevation (99.6º to 104º F [37.5º to 40º C]) due to dehydration
Place patient in cool area and remove constrictive clothing
Place moist sheet over patient to decrease core temperature
Provide oral fluid
Replace electrolytes
Initiate normal saline IV solution if oral solutions are not tolerated
100
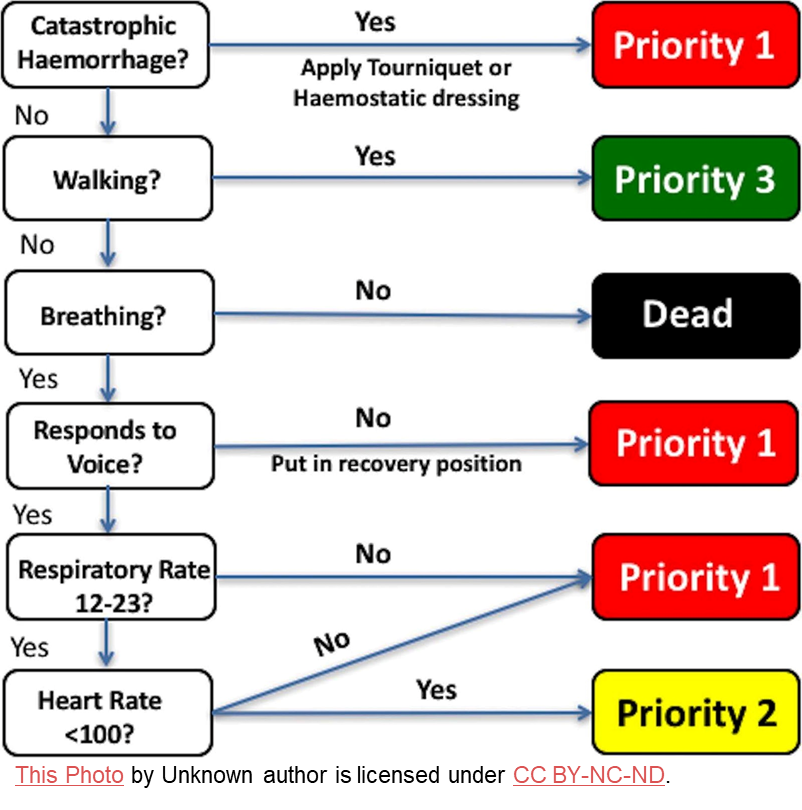
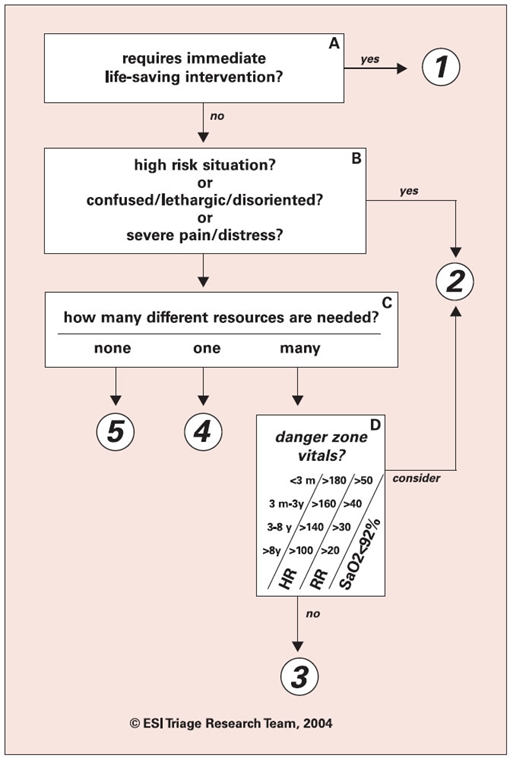
Basic principles of triage
The basic principles of triage involve rapidly assessing patients and prioritizing care based on severity and available resources. Key triage principles include:
1. Identifying life-threatening conditions that require immediate intervention.
2. Prioritizing the most critically ill or injured patients first.
3. Efficiently utilizing personnel and equipment to maximize care.
4. Periodically re-evaluating patients as conditions can change.
5. Maintaining clear documentation and communication.
Triage systems like the 5-level Emergency Severity Index help standardize the process. Effective triage ensures the right patient receives the right care in the right place at the right time.
200
How to determine that an ET tube has migrated deeper into the lung or backward out of the trachea and how you would respond if either situation occurred.
To determine if an endotracheal (ET) tube has migrated deeper into the lung or out of the trachea, assess for the following signs:
Deeper into lung: Absent or diminished breath sounds on one side, increased peak inspiratory pressures, desaturation.
Out of trachea: Gurgling sounds, inability to ventilate, severe desaturation, coughing/choking.
If the ET tube has migrated deeper into the lung, immediately remove the tube slightly until bilateral breath sounds are heard. Confirm proper depth with chest x-ray.
If the ET tube has migrated out of the trachea, it is a life-threatening emergency. Stay with the patient, call for help, attempt to reinsert the tube if possible while providing bag-valve-mask ventilation and 100% oxygen. If unsuccessful, be prepared to perform an emergency surgical airway.
Continuously monitor tube position and secure it properly to prevent dislodgement. Promptly communicate any concerns to the healthcare team.
200
Triage
200
Response to hypotension/hypovolemic shock
For hypovolemic shock caused by significant blood or fluid loss, the key initial responses are:
1. Control any active bleeding or sources of fluid loss.
2. Initiate fluid resuscitation with isotonic crystalloid solutions like normal saline or lactated Ringer's. Give 20 mL/kg fluid boluses and reassess after each bolus.
3. If hemorrhagic shock, transfuse packed red blood cells as needed.
4. Administer oxygen and establish monitoring.
5. Identify and treat the underlying cause.
Prompt volume replacement is crucial to restore circulating volume, preload, and perfusion pressures. Frequent reassessment is necessary to guide ongoing fluid resuscitation. Vasopressors may be required if hypotension persists despite fluid replacement. Early recognition and aggressive treatment of hypovolemic shock improves outcomes.
200
Response to heat injury
Heat Stroke
Failure of the hypothalamic thermoregulatory processes
Vasodilation, increased sweating and respiratory rate deplete fluids and electrolytes, specifically sodium
Sweat glands stop functioning and core temperature increases (>104º F [40º C])
Treatment: stabilize patient’s ABCs and rapidly reduce temperature
Cooling methods
Remove clothing
Cover with wet sheets
Place patient in front of large fan
Immerse in ice water bath
Administer cool fluids or lavage with cool fluids
Shivering: increases core temperature, complicates cooling efforts, treated with IV chlorpromazine
Aggressive temperature reduction until core temperature reaches 102º F (38.9º C)
Monitor for signs of rhabdomyolysis, myoglobinuria, and disseminated intravascular coagulation
200
Review principals or prioritization (both priority patients and priority actions)
Prioritization involves assessing and ranking patient needs based on clinical acuity and potential for adverse outcomes. Key principles include:
For priority patients:
Unstable vital signs or life-threatening conditions like airway compromise take top priority
Prioritize patients with rapidly deteriorating or time-sensitive conditions
Consider factors like comorbidities, age, and risk of complications
For priority actions:
Use the ABCs - ensure airway, breathing, and circulation first
Address any active bleeding, shock, or severe pain immediately
Provide interventions to stabilize and prevent further deterioration
Frequently reassess and re-prioritize as the situation evolves
Involve the interdisciplinary team for complex patient needs
Effective prioritization requires strong assessment skills, clinical judgment, and the ability to think critically about anticipated problems and outcomes. Safety for patients and staff is always the top concern.
300
What is PEEP?
PEEP stands for Positive End-Expiratory Pressure. It is a ventilator setting that applies positive pressure to the airway during the expiratory phase of breathing. PEEP helps keep alveoli open and increases functional residual capacity, often improving oxygenation. It is routinely used in mechanically ventilated patients, with typical settings between 5-10 cm H2O. Higher PEEP levels may be required in conditions like ARDS. While beneficial for oxygenation, excessive PEEP can impair venous return and cardiac output, so careful monitoring is necessary.
300
Response to anaphylaxis
For an anaphylactic reaction, the immediate response should be:
1. Administer epinephrine intramuscularly as the first-line treatment. Epinephrine reverses airway edema, bronchoconstriction, and hypotension.
2. Call for emergency medical assistance.
3. Maintain the airway and provide supplemental oxygen. Be prepared for potential airway compromise.
4. Initiate IV fluids like normal saline to treat hypotension and fluid extravasation.
5. Give adjunctive treatments like antihistamines (e.g., diphenhydramine) and corticosteroids.
6. Frequently monitor vital signs and be prepared to initiate CPR if needed.
The key is rapid recognition and treatment with epinephrine to prevent life-threatening respiratory and cardiovascular complications. Removing any potential allergen triggers is also important.
300
Response to near drowning
Results when person becomes hypoxic due to submersion in substance, usually water
Drowning: death from suffocation after submersion in fluid
Immersion syndrome occurs with immersion in cold water, which leads to stimulation of the vagus nerve and potentially fatal dysrhythmias
Near-drowning: survival from potential drowning
Aggressive resuscitation efforts and the mammalian diving reflex improve survival of near-drowning victims
Treatment of submersion injuries
Correct hypoxia
Correct acid-base and fluid imbalances
Support basic physiologic functions
Rewarm if hypothermia present
Initial evaluation: ABCD
Mechanical ventilation with PEEP or CPAP to improve gas exchange when pulmonary edema is present
Deterioration in neurologic status: cerebral edema, worsening hypoxia, profound acidosis
Observe for minimum of 4–6 hours
Secondary drowning is a concern with patients who are essentially symptom free
400
How to determine if the patient has the appropriate amount of peep or if they have too much peep
To determine if a patient has the appropriate amount of PEEP or too much PEEP, monitor the following:
Appropriate PEEP:
Improved oxygenation without compromising hemodynamics
Adequate tidal volumes with acceptable peak inspiratory pressures
Bilateral equal breath sounds
Too much PEEP:
Worsening hypotension or decreased cardiac output
Increased peak inspiratory pressures
Barotrauma risk
Signs of auto-PEEP (air trapping, increased work of breathing)
The goal is to find the optimal PEEP level that recruits collapsed alveoli and improves oxygenation while avoiding adverse hemodynamic effects. Frequent assessment of oxygenation, ventilation parameters, and hemodynamic status is necessary to guide PEEP adjustments. Interprofessional collaboration is key for safe PEEP management.
400
Sepsis and septic shock
Sepsis is a life-threatening condition caused by the body's dysregulated response to an infection. It leads to organ dysfunction. Septic shock is a subset of sepsis, characterized by persistent hypotension despite fluid resuscitation, and inadequate tissue perfusion resulting in tissue hypoxia.
Key points about sepsis and septic shock:
Can be caused by bacterial, viral, fungal or parasitic infections
Clinical manifestations include fever, tachycardia, tachypnea, hypotension, altered mental status
Septic shock criteria: hypotension requiring vasopressors, high lactate despite fluids
Complications include acute respiratory distress syndrome, multi-organ dysfunction
Prompt recognition, source control, antibiotics, and hemodynamic support are crucial
Mortality risk is high, especially with septic shock, requiring intensive care management
Early identification and aggressive treatment following evidence-based protocols improve outcomes in sepsis and septic shock. An interprofessional team approach is vital.
400
Responding to human bites and animal bites
Initial treatment: clean with copious irrigation, debridement, tetanus prophylaxis, and analgesics
Prophylactic antibiotics for bites at risk for infection
Wounds over joints
Wounds less than 6–12 hours old
Puncture wounds
Bites on hand or foot
Puncture wounds left open
Lacerations loosely sutured
Wounds over joints splinted
Rabies prophylaxis essential in management of animal bites
Initial injection: rabies immune globulin
Series of five injections of human diploid cell vaccine: days 0, 3, 7, 14, and 28
500
Who should take a PPI?
Proton pump inhibitors (PPIs) should be taken by patients with:
Erosive esophagitis or severe gastroesophageal reflux disease (GERD) not responsive to other treatments
Active duodenal or gastric ulcers
Conditions causing excessive stomach acid like Zollinger-Ellison syndrome
Need for prevention of NSAID-induced or stress ulcers
500
How to respond to a choking patient
For a choking patient, take the following steps:
1. Ask "Are you choking?" If the patient nods yes or cannot speak, call for help.
2. Give 5 back blows between the shoulder blades with the heel of your hand.
3. If unsuccessful, perform 5 abdominal thrusts by placing a fist just above the navel and pulling inward and upward.
4. Alternate back blows and abdominal thrusts until the object is expelled or the patient becomes unconscious.
5. If unconscious, begin CPR, ensuring no obstructed airway before giving breaths.
6. For a pregnant or obese patient, give chest thrusts instead of abdominal thrusts.
The key is to act quickly and effectively dislodge the foreign body. Seek emergency care if the obstruction persists. Prevention through education on choking risks is also important.