Asthma
Asthma Cont.
Topics Cont.
Topics Cont.
More Topics
100
What causes Asthma?
Triggers:
Air Pollutants
Aerosol sprays
Cigarette smoke
Exhaust fumes
Oxidants
Perfumes
Sulfur dioxides
Allergen Inhalation
Animal dander (e.g., dogs, cats, mice, guinea pigs)
Cockroaches
House dust mite
Molds
Pollens
Drugs
Aspirin
β-Adrenergic blockers
NSAIDs
Food Additives
Beer, wine, dried fruit, shrimp, processed potatoes
Monosodium glutamate
Sulfites (bisulfites and metabisulfites)
Tartrazine
Occupational Exposure
Agriculture, farming
Industrial chemicals and plastics
Laundry detergents
Metal salts
Paints, solvents
Wood and vegetable dusts
Pulmonary
Sinusitis, allergic rhinitis
Viral URI
Other Factors
Exercise and cold, dry air
GERD
Hormones, menses
Stress
Biological Considerations
Men
Before puberty, asthma affects more boys.
Boys most likely to have less severe symptoms by late teen years.
Women
In adulthood, asthma affects more women.
Between 40 and 60 years of age, have a higher incidence and severity.
Women who present to the emergency department are more likely to need hospitalization.
Have a higher overall mortality.
100
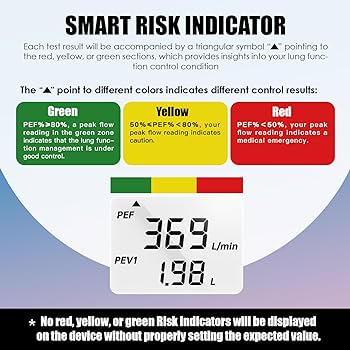
Peak flow rate measurements & meanings
A chart of the asthma action plan. The chart shows three sections, green zone, yellow zone, and red zone. The green zone shows four columns with doing wee, daily medications medicines, how much to take, and when to take it. Yellow zone shows asthma is getting worse with quick-relief medicine for first and second doses. The red zone shows a medical alert and at the bottom of the chart, it shows the danger signs. The green zone shows doing well: no cough, wheeze, chest tightness, or shortness of breath during the day or night. Can do usual activities and if a peak flow motor is used, peak flow: more than 80 percent or more of my best peak with my best peak flow. It also shows daily medications medicine, how much to take, and when to take them. Yellow zone shows asthma is getting worse: cough, wheeze, chest tightness, or shortness of breath, waking at night due to asthma, can do some, but not all usual activities with peak flow. The red zone shows a medical alert with very short or breath or quick-relief medicines have not helped, cannot do usual activities, or symptoms are same or get worse after 24 hours in yellow zone with peak flow: less than. It also shows take this medicine and then call your doctor now column. The danger signs at the bottom show trouble walking, and talking due to shortness of breath, lips or fingernails are blue. The rightward thick red arrow shows the quick-relief medicines and goes to the hospital.
100
How to identify poor airway clearance
Signs of poor airway clearance include:
Visible secretions in the airway (endotracheal tube, mouth, etc.)
Increased respiratory rate or frequent coughing
Sudden decrease in oxygen saturation levels
Suspected aspiration of secretions
Increased peak airway pressures on the ventilator
Audible adventitious breath sounds over the trachea or bronchi (wheezing, crackles, etc.)
Increased work of breathing
Monitoring respiratory status, oxygen levels, and sputum production can help identify when a patient is having difficulty clearing their airway of mucus and secretions. Interventions like suctioning, chest physiotherapy, and nebulizer treatments may then be needed to facilitate airway clearance.
100
What patients need to know about cystic fibrosis?
Patients with cystic fibrosis (CF) need to understand the following key points about their condition:
1. CF is a genetic, life-long disease that primarily affects the lungs and digestive system. It causes thick, sticky mucus buildup that leads to breathing difficulties and malnutrition.
2. Consistent daily treatments are crucial, including airway clearance techniques, inhaled medications, pancreatic enzymes, and a nutritious high-calorie diet.
3. Preventing and aggressively treating lung infections is vital to preserve lung function. Antibiotics and hospitalization may be required.
4. CF can impact fertility, so genetic counseling is recommended before planning a pregnancy.
5. Regular exercise, staying well-hydrated, and maintaining good mental health are important for overall well-being.
6. Lifelong care from a multidisciplinary CF team is essential for monitoring the condition and adjusting treatments as needed.
7. While CF is a challenging disease, many patients can live into adulthood with proper care and an optimistic outlook.
The key is adhering to the prescribed treatment plan, maintaining open communication with the healthcare team, and being proactive about managing CF's effects.
100
Methods to determine correct placement of an ET tube
There are several methods to confirm correct endotracheal (ET) tube placement:
1. Observe for symmetric chest rise and fall with ventilations.
2. Auscultate for equal breath sounds bilaterally and no sounds over the epigastrium.
3. Use an end-tidal CO2 detector or capnography - presence of exhaled CO2 confirms tracheal placement.
4. Obtain a chest x-ray to visualize tube position in the mid-trachea about 2-4 cm above the carina.
5. Note stable or improving oxygen saturation levels after intubation.
6. Continuously monitor the patient's respiratory status and tube position.
Proper ET tube placement is critical to ensure effective ventilation and oxygenation. Use multiple confirmation methods initially and with any change in patient status or tube position.
200
Treatment & Side Effects
Controller Drugs
Corticosteroids
Short-acting β2 adrenergic agonists (SABA)
Maintenance, Reliever and Alternate Reliever Drugs (MART)
Anticholinergics
Short-acting muscarinic antagonist (SAMA)
ipratropium (Atrovent HFA)
Can be monotherapy.
Produces bronchodilation within minutes.
Side effects: Headache, dry mouth, dizziness, palpitations.
Long-acting muscarinic antagonist (LAMA)
β2 adrenergic agonists
Use with caution in patients with heart problems.
Both SABAs and LABAs may cause increased BP and heart rate, central nervous system stimulation, and dysrhythmias.
Short-acting β-adrenergic agonist (SABA)
albuterol (Proventil HFA, Ventolin HFA, Proair HFA)
Produces bronchodilation within 5 minutes; effects last 2–5 hr.
Oral tablets (long-acting, extended release) not for acute situation.
Side effects: Tremors, headache, tachycardia, nausea.
MDI may be more effective than nebulizer as drug delivered more quickly to the lungs.
Use with caution in patients with cardiac disorders because of ↑ BP and heart rate, CNS stimulation, and ↑ risk for dysrhythmias.
Epinephrine (Primatene Mist HFA)
Sold OTC.
Side effects: tachycardia, ↑ BP.
Do not take with MAO inhibitors.
levalbuterol (Xopenex, Xopenex HFA)
Response occurs within 15 minutes of administration, and peak effect in 90 min.
Do not use if solution discolored.
Side effects: Tremors, headache, rash
Long-acting β-adrenergic agonist (LABA)
In asthma: Never use as monotherapy. Use in combination with ICSs.
Should not be the first or only drug used to treat asthma.
Should be added to the treatment plan only if other drugs do not control asthma.
Do not use to treat wheezing that is getting worse.
formoterol (Foradil Perforomist)
Side effects: Tremors, tachycardia, GI distress.
Use with caution in diabetes, can increase glucose levels.
salmeterol (Serevent Diskus)
Do not use more than twice daily.
Side effects: Tremors, tachycardia, muscle pain, cold symptoms.
Helps prevent exercise-induced asthma in those with persistent asthma.
200
Pulmonary Embolism Response & S/S
Response:
A pulmonary embolism (PE) is a blockage in one or more arteries in the lungs, usually caused by a blood clot that travels from another part of the body, most commonly the deep veins in the legs (deep vein thrombosis).
S/S:
The main signs and symptoms of pulmonary embolism include:
Sudden shortness of breath
Chest pain that may worsen with deep breathing
Rapid breathing and heart rate
Coughing, sometimes with bloody mucus
Leg pain or swelling, indicating a deep vein thrombosis
Dizziness, lightheadedness, or fainting
Fever
Anxiety or sense of impending doom
The symptoms can range from mild to severe depending on the size of the clot and degree of lung involvement. Larger clots can lead to low blood pressure, bluish skin, and even sudden death. Prompt medical attention is crucial if pulmonary embolism is suspected.
200
CVP what high and low rating means and how to respond
A high central venous pressure (CVP) reading, typically above 8-12 mmHg, indicates fluid overload or right ventricular failure. Respond by limiting IV fluids, administering diuretics if appropriate, and considering causes like heart failure, pulmonary hypertension, or fluid overload. A low CVP below 0-5 mmHg suggests hypovolemia. Respond by giving IV fluids to improve preload and assessing for bleeding, dehydration, or other causes of volume depletion. Trends are important - isolated high or low readings may not accurately reflect volume status. Monitor the patient's overall clinical picture when interpreting CVP values.
200
Methods to determine correct balloon pressure of an ET tube
There are a few methods to determine the correct endotracheal tube cuff pressure:
1. Minimal Occlusive Volume (MOV) Technique: Inflate the cuff until you no longer hear an air leak around the tube during inspiration. Then use a manometer to confirm the cuff pressure is 20-30 cmH2O.
2. Palpation Method: Palpate over the trachea and inflate the cuff until no air leak is felt during inspiration. Confirm pressure is 20-30 cmH2O with a manometer.
3. Direct Measurement: Use a cuff pressure manometer to directly measure and adjust the cuff pressure to 20-30 cmH2O.
The goal is to maintain a cuff pressure high enough to seal the airway and prevent aspiration, but low enough (20-30 cmH2O) to avoid tracheal mucosal damage from over-inflation. Routinely monitor and document cuff pressures.
300
Treatment Cont.
Corticosteroids
hydrocortisone (Solu-Cortef)
methylprednisolone (Medrol, Solu-Medrol)
prednisone
Oral preferred over IV.
Side effects: hyperglycemia, fluid retention.
May take 2 weeks for results to be seen in severe COPD exacerbation.
Take oral dose in morning with food or milk.
High dose may cause GI distress.
Long-term therapy requires vitamin D and calcium supplements to prevent osteoporosis.
Long-term steroid therapy: discontinue gradually to prevent adrenal insufficiency.
Inhaled
beclomethasone dipropionate (Qvar)
May not see effects until after at least 2 weeks of regular treatment.
Side effects: Headache, hoarseness.
budesonide (Pulmicort Flexhaler)
May not see effects until after at least 2 weeks of regular treatment.
Side effects: Headache cold symptoms.
ciclesonide (Alvesco)
Side effects: Cold symptoms, nose bleeds.
fluticasone (Flovent HFA, Flovent Diskus)
Rinse mouth with water or mouthwash after use to prevent oral fungal infections.
Side effects: Headache, cold symptoms.
Spacer device with MDI may decrease incidence of oral candidiasis.
May not see effects until after at least 2 weeks of regular treatment.
mometasone (Asmanex HFA, Asmanex Twisthaler)
May not see effects until after at least 2 weeks of regular treatment.
Leukotriene modifiers
Leukotriene receptor antagonist
montelukast (Singulair)
Do not use in acute attack.
Can be used to prevent wheezing and SOB caused by asthma during exercise.
Side effects: Headache, fatigue, dizziness, GI distress.
zafirlukast (Accolate)
Do not use in acute attack.
No specific side effects.
Take at least 1 hr before or 2 hr after meals.
Contraindicated in cirrhosis.
Affects metabolism of oral warfarin (drug ↑ prothrombin time).
Leukotriene inhibitor
zileuton (Zyflo, Zyflo CR)
Do not use in acute attack.
Do not crush, chew, or cut tablets.
Monitor liver enzymes.
May interfere with metabolism of warfarin and theophylline.
Changes in sleep pattern and behavioral abnormalities reported.
Methylxanthines
IV agent: aminophylline (second-line therapy)
Oral: theophylline
Side effects: CNS stimulation, headache, tachycardia, dysrhythmias, nausea, vomiting, altered glucose levels.
Nicotine ↑ metabolism of methylxanthines in liver (dosage increase needed for those who smoke).
Many drug interactions.
Taking drug with food or antacids may help GI effects.
Very limited use.
300
Treatment of PE
The main treatments for pulmonary embolism (PE) are:
Anticoagulants (blood thinners) - These are the primary treatment to prevent further clot formation. Options include low molecular weight heparins like enoxaparin initially, followed by direct oral anticoagulants (DOACs) like apixaban, rivaroxaban, or dabigatran for long-term use.
Thrombolytics - For severe, life-threatening PEs, medications like alteplase can help dissolve clots quickly. However, they carry a risk of bleeding.
Surgical/Interventional - Massive PEs with hemodynamic instability may require catheter-based therapies to remove clots or surgical embolectomy. Inferior vena cava filters can also be placed to trap clots.
Supportive care - Supplemental oxygen, IV fluids, vasopressors, and other measures are used to stabilize patients while treating the underlying clot.
The goals are to improve oxygenation and blood flow, prevent clot extension, and reduce the risk of recurrence. Prompt treatment is crucial to prevent complications.
300
What it means to zero an arterial line (basically) and what you zero it to (what is your reference point)
Zeroing an arterial line means calibrating the pressure monitoring system to atmospheric pressure as the reference point or "zero" level. This is done by opening the line to room air and observing that the monitor reads zero mmHg. The reference point is the level where the arterial catheter transducer is located, which should be kept level with the patient's phlebostatic axis (around the 4th intercostal space at the midaxillary line). Proper zeroing ensures accurate blood pressure readings by accounting for atmospheric pressure and positioning.
300
How to manage a patient with an ET tube on a ventilator (not the machine, what to watch for with the patient)
When managing a patient with an endotracheal (ET) tube connected to a ventilator, closely monitor the following:
Tube position - Ensure the ET tube remains properly positioned by assessing for bilateral breath sounds, symmetrical chest rise, stable oxygen saturation, and absence of air entry over the epigastrium.
Airway patency - Watch for signs of airway obstruction like increased respiratory rate, use of accessory muscles, or sudden desaturation, which may require suctioning.
Ventilator synchrony - Observe for patient-ventilator dyssynchrony and signs of air trapping, which increase the risk of barotrauma.
Oral care - Provide frequent oral hygiene to prevent ventilator-associated pneumonia.
Sedation and pain control - Assess and manage anxiety, agitation, and pain appropriately to avoid self-extubation.
Neurovascular status - Routinely check for signs of limb ischemia if the ET tube is secured with ties.
Hemodynamic status - Monitor vital signs, oxygenation, and ventilation for any acute changes requiring intervention.
Timely communication of any changes or concerns to the healthcare team is crucial for safe patient management.
400
Treatment Again
Monoclonal antibodies
Anti-IgE
omalizumab (Xolair)
Dose and frequency based on total IgE levels and pre-treatment weight.
Total IgE levels elevated up to 1 year after therapy stopped; do not use as a guide for dosing drug.
Side effects: Dizziness, joint pain, fatigue
Pain, burning at injection site, anaphylactic reaction possible.
Give only under direct medical supervision every 2–4 weeks.
Anti-interleukin 5
mepolizumab (Nucala)
Add-on therapy in patients with severe asthma attacks despite receiving other asthma drugs.
Give only under direct medical supervision every 4 weeks.
Side effects: Headache, back pain.
Hypersensitivity reactions have been known to occur hours and days later.
reslizumab (Cinqair)
Add-on therapy in patients receiving other asthma drugs.
Given every 4 weeks as an IV infusion over 1 hr.
Risk for anaphylactic reactions.
Phosphodiesterase inhibitors
Combination preparations
SAMA/SABA
ICS/LABA
budesonide/formoterol (Symbicort)
fluticasone/salmeterol (Advair Diskus or HFA)
mometasone furoate/formoterol fumarate (Dulera)
Do not use in acute attacks.
Long-term therapy only.
Side effects: Headache, cold symptoms.
Rinse mouth after using.
LAMA/LABA
400
What is cystic fibrosis?
Cystic fibrosis (CF) is an inherited, chronic disease that affects the lungs, digestive system, and other organs. It is caused by mutations in the CFTR gene, which regulates the movement of chloride ions across cell membranes. This leads to the buildup of thick, sticky mucus that clogs the airways and obstructs digestive enzymes. The main symptoms include persistent coughing, wheezing, poor growth, and recurrent lung infections. While there is no cure, treatments aim to clear mucus from the lungs, control infections, and address nutritional deficiencies. With early diagnosis and proper management, many individuals with CF can live into adulthood.
400
Complications of having an arterial line
Potential complications of having an arterial line include:
Hemorrhage - This can occur if the catheter dislodges or the line disconnects. Monitor the arterial waveform and use proper connections to avoid this.
Infection - Strict sterile technique is required when inserting and maintaining the line to prevent infection.
Thrombus formation - Blood clots can form in the catheter, obstructing blood flow. Flushing the line regularly helps prevent this.
Neurovascular impairment - The catheter can compromise blood flow to the extremity, causing coolness, pain, paralysis. Check distal pulses hourly.
Ischemia/necrosis - Severely reduced blood flow can lead to tissue death and potential limb loss if not promptly treated.
Close monitoring of the line, limb perfusion, and strict aseptic technique are crucial to prevent and detect these serious complications early. Immediately report any concerns to the healthcare provider.
400
Managing a patient on a mechanical ventilator involves close monitoring and an interprofessional team approach.
Airway and Breathing: Assess breath sounds, chest rise, airway patency, and ventilator synchrony. Provide oral care and suction as needed. Monitor oxygenation and ventilation parameters.
Hemodynamics: Frequently evaluate vital signs, perfusion status, and any cardiovascular changes requiring intervention.
Neurological: Assess sedation levels, pain, and any need for neuromuscular blockade. Implement measures to prevent self-extubation.
Nutrition and Elimination: Ensure adequate nutritional support and monitor intake/output, bowel sounds, and gastrointestinal function.
Mobility and Positioning: Implement protocols for turning, range of motion, and positioning to prevent complications.
Psychosocial: Address the patient's anxiety, comfort needs, and involve family. Explain procedures and provide emotional support.
Continuous interprofessional communication and monitoring are crucial to rapidly identify and manage any changes in the patient's condition. Timely interventions can prevent complications.
500
Determining Effectiveness of Treatment:
To determine the effectiveness of asthma medications, healthcare providers typically assess:
Symptom control - Monitoring frequency and severity of coughing, wheezing, shortness of breath, and nighttime awakenings.
Need for rescue medication - Tracking use of short-acting bronchodilators like albuterol for quick relief.
Lung function tests - Measuring peak flow rates or FEV1 values before and after treatment.
Exercise tolerance - Evaluating ability to perform normal activities without asthma symptoms.
Frequency of asthma attacks/exacerbations - Counting number of episodes requiring oral steroids or hospitalization.
Side effects - Watching for potential adverse effects like thrush, hoarseness, or growth suppression in children.
Regular follow-ups, adjusting medication doses, and reviewing inhaler technique help ensure optimal asthma control. The goal is to achieve and maintain well-controlled asthma status.
500
What does cystic fibrosis do?
Cystic fibrosis (CF) is a progressive genetic disorder that primarily affects the respiratory and digestive systems. In the lungs, CF causes thick, sticky mucus buildup that clogs the airways, leading to chronic lung infections, inflammation, and eventual lung damage. In the digestive system, CF disrupts the normal function of the pancreas, preventing the release of enzymes needed to break down and absorb nutrients from food properly. This results in malnutrition, poor growth, and other gastrointestinal issues. CF can also impact the reproductive system, sweat glands, and other organs. While treatments have improved, CF remains a life-threatening condition without a cure.
500
What to monitor in a patient with an IABP.
When using an intra-aortic balloon pump (IABP), it's crucial to monitor for the following potential complications:
Vascular injury and compromised distal circulation - Assess neurovascular status of the extremity frequently for signs of ischemia like coolness, delayed capillary refill, pain, or paralysis. This is an emergency requiring prompt intervention.
Thrombosis and embolism - The IABP can cause platelet destruction and thrombus formation, leading to embolic events. Monitor for weak/absent distal pulses.
Limb ischemia - The IABP balloon can temporarily occlude blood flow to major arteries like the subclavian, renal, or mesenteric arteries. Watch for decreased urine output or absent bowel sounds.
Infection - Patients are prone to local or systemic infections with IABP use. Monitor for signs of infection at the insertion site or systemically.
Equipment malfunction - Be prepared to recognize and respond to IABP console alarms, gas leaks, or balloon rupture, which require immediate removal.
Frequent assessments, monitoring the arterial waveform, and prompt reporting of any concerns are essential to prevent serious IABP-related complications.
Vascular injuries
Thrombus and embolus formation
Thrombocytopenia
Peripheral nerve damage
Ischemia to periphery, kidneys, bowel
Infection
Mechanical complications
Improper timing of balloon inflation
Balloon leak
Malfunction of balloon or console
500
When managing a patient on hemodynamic monitoring, it's essential to:
Continuously assess hemodynamic parameters like heart rate, blood pressure, central venous pressure, pulmonary artery pressures, cardiac output, and oxygen saturation levels. Monitor for trends over time rather than single values.
Integrate hemodynamic data with the patient's clinical presentation from physical assessments. Look for signs of adequate perfusion like mentation, skin temperature, and urine output.
Evaluate the patient's response to fluid resuscitation, vasopressors, inotropes, or other therapies aimed at optimizing hemodynamics. Make adjustments as needed based on the data.
Ensure accurate measurement techniques and troubleshoot any equipment issues promptly. Pay close attention to invasive line patency and dressing integrity.
Communicate any significant changes or concerns to the healthcare team immediately. Frequent interprofessional collaboration is key for safe management and prevention of complications.