Adrenaline
Airway
Axial
Are we going to...?
Agglomeration
100
1:100,000
The concentration of push dose epi
100
This device traditionally is used for anterior airways and allows one to feel the tracheal rings when inserted properly.
Bougie
100
This is the traditional anterior landmark for needle thoracostomy.
2/3 intercostal space midclavicular line
100
Head on MVC mod speed. +Airbags. 28 yo female unrestrained driver with c/o chest + abd pain, vss, awake, alert and fully oriented w gcs-15. Pt insisting to go to St. Luke's even after explaining Risk of not going to trauma center. What is your course of action?
Proceed to patient's choice of receiving facility.
100
The first U.S. President to be treated with a defibrillator.
Lyndon Johnson in 1972 when he had an MI.
200
During a cardiac arrest, the PCGs currently limit the doses of 1:10,000 IV Epinephrine to 4, unless this occurs.
Achieve ROSC that decompensates back into cardiac arrest.
200
Arytenoid cartilage
200
Intubated patients with tension pneumothorax will develop hemodynamic collapse more quickly than spontaneously breathing patients due to this intervention.
Positive pressure ventilation
200
MVC highway speed, prolonged extrication, 2 patients, 1 is j4. Your pt is 40ish yo male unrestrained partially ejected. CC abd pain and head pain. He is confused w GCS 12 BP 100/69 HR 108 R20 ETCO2 31 SPo2 97%
Where do you transport and what category trauma do you assign the patient?
Mercy as a "trauma alert".
re: This patient meets field level 1 criteria and hospital category 2 criteria.
200
This exam finding differentiates the FAST stroke exam from the LAMS score.
Grip Strength
300
5 ml of Epinephrine 1:1000 nebulized can be used to treat this suspected illness with this sign.
Croup with resting stridor.
300
The most appropriate sedative to administer for airway management in a patient with status epilepticus.
Versed
300
A male patient with normal lung mechanics weighing 300 lbs and 5'11 inches tall should have a tidal volume of 6-8 ml/kg based up upon this measurement.
Ideal Body Weight
300
Husband was eating breakfast with wife at 0720 when he notices her speech sounds different. Suddenly, she stands up, stumbles, and falls. He helps her up and notices she has unsteady gait. She also says she has dizziness and double vision. Grips equal. No facial droop. Understanding that this could be a stroke, what level of stroke center does she need to go to? Where is her stroke? Do you document her "last known well" or "time of onset"?
Any stroke center. (LAMS not indicative of LVO and within TPA window)
Posterior (balance center)
Time of Onset (onset was actually witnessed)
300
This route of administration of dexamethasone (IV, PO, or IM) is most efficacious.
IV, PO and IM are all equally effective
400
This is the volume and concentration of Epinephrine to be used on a 4month old in cardiac arrest. Parents think he weighs about 10 lbs.
0.6ml of 1:10,000
400
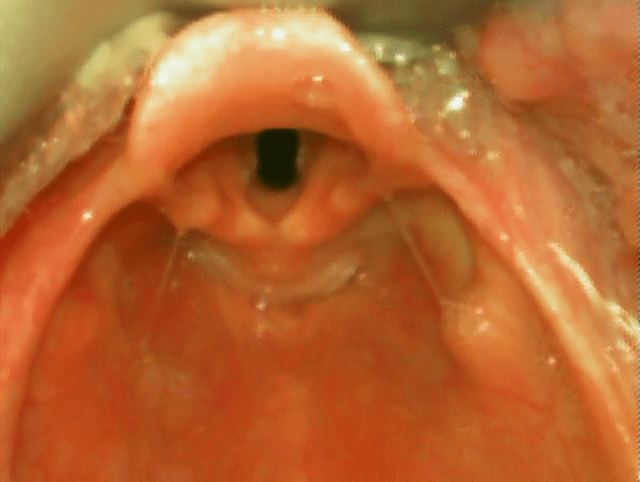
This is the narrowest part of the pediatric airway.
Cricoid cartilage. (subglottic area)
400
The liver can be as high as this anatomic landmark.
Nipple line or 7th vertebra
400
Syncope at doctor's office on Barnes West campus. You do ECG revealing elevation lead 2,3 and avf. Pt is hypotensive and somewhat confused. Rt sided ECG confirms v4R elevation. The doctor, his dermatologist, says his Cardiologist is at Barnes South, and he should go there, but he has not called them. Where do you transport?
Mercy or MoBap
Re: Barnes WC does not have cath lab. Barnes South too far with unstable patient. MoBap would be best option as his care is through BJC, but Mercy could be second destination if traffic precludes easy movement to MOBap. EMTALA does not hold a patient on that campus if services not available, and never affects EMS decision unless an accepting physician is confirmed and the patient is stable enough for the transport. Extremely rare for a 911 service!
400
The Frank Starling Curve compares cardiac output to Left Ventricular End Diastolic Pressure (LVEDP). In the prehospital setting, we perform this intervention to increase LVEDP.
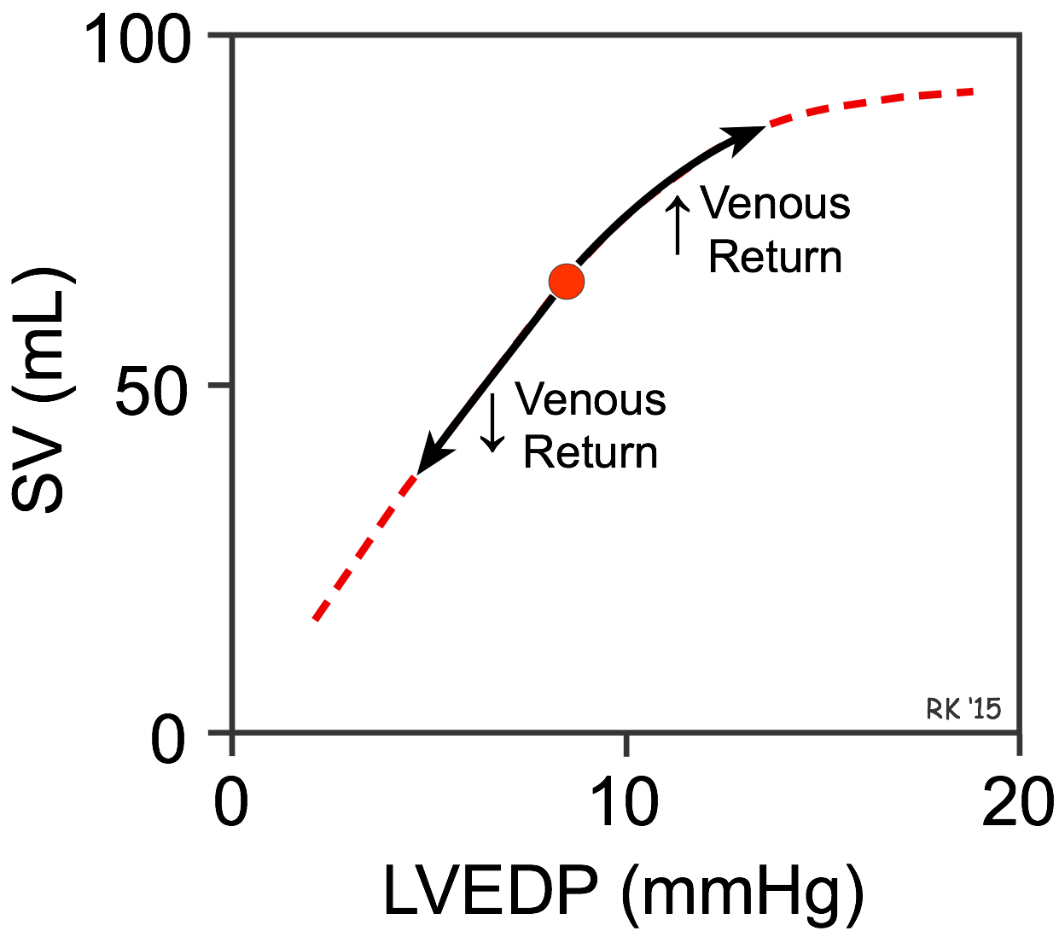
Fluid bolus
500
What receptors does Epinephrine act on?
Alphas and Betas
500
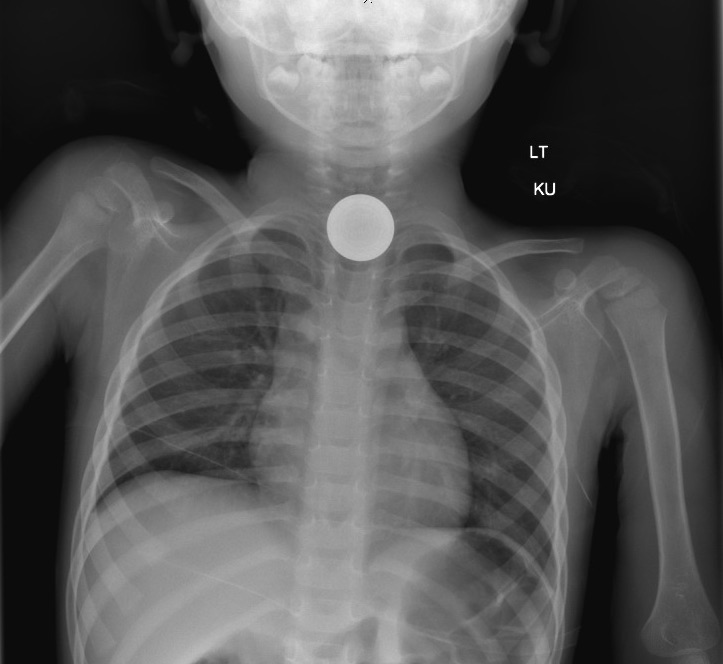
Esophageal foreign body
500
This syndrome occurs after violent retching and presents with severe chest pain.
Boerhaave Syndrome
500
Pt 57 yo male fine when went to bed around 2200, last night, but wife went to see why he was still in bed at 0900. She finds him nearly obtunded, flaccid on left side. Strong grip rt side. No movement to lt hand. Pronounced facial droop. He will look for you when you call his name, but his response is slow and his eyes to not track together. Vitals stable with blood glucose of 198. Only history is hypertension/hyperlipidemia for which he is moderately compliant. Where do you transport and why?
Closest stroke center with clot retrieval services unless more than 15 min beyond level 1 stroke center. re: outside TPA window with LKW around 11 hours and LAMS - 5
500
Term for clot retrieval in large vessel strokes
Endovascular Thrombectomy