Pathophysiology
S/S
Treatment
Protocol
Potpourri
99
Name 2 other names (non brand) for acetaminophen
N-acetyl-paraaminophenol
- Paracetamol
- APAP
99
What investigations should you do for an acetaminophen overdose
- 4 hour acetaminophen level
- INR, AST/ALT, Cr
- Salicylate, etoh
- ECG
- Maybe: VBG, electrolytes, urea, glucose, ext lytes, pregnancy test, osmolality
99
If you have a patient with AST/ALT elevation 18 hours after presumed acetaminophen ingestion but with an undetectable acetaminophen level. Do you treat with NAC? What side effect are they at increased risk for?
- Yes
- Anaphylactoid reaction
99
When should a patient with acetaminophen toxicity receive vitamin K?
In patients with acute liver failure (INR approaching 5)
5-10mg IV daily for 1-3 days
99
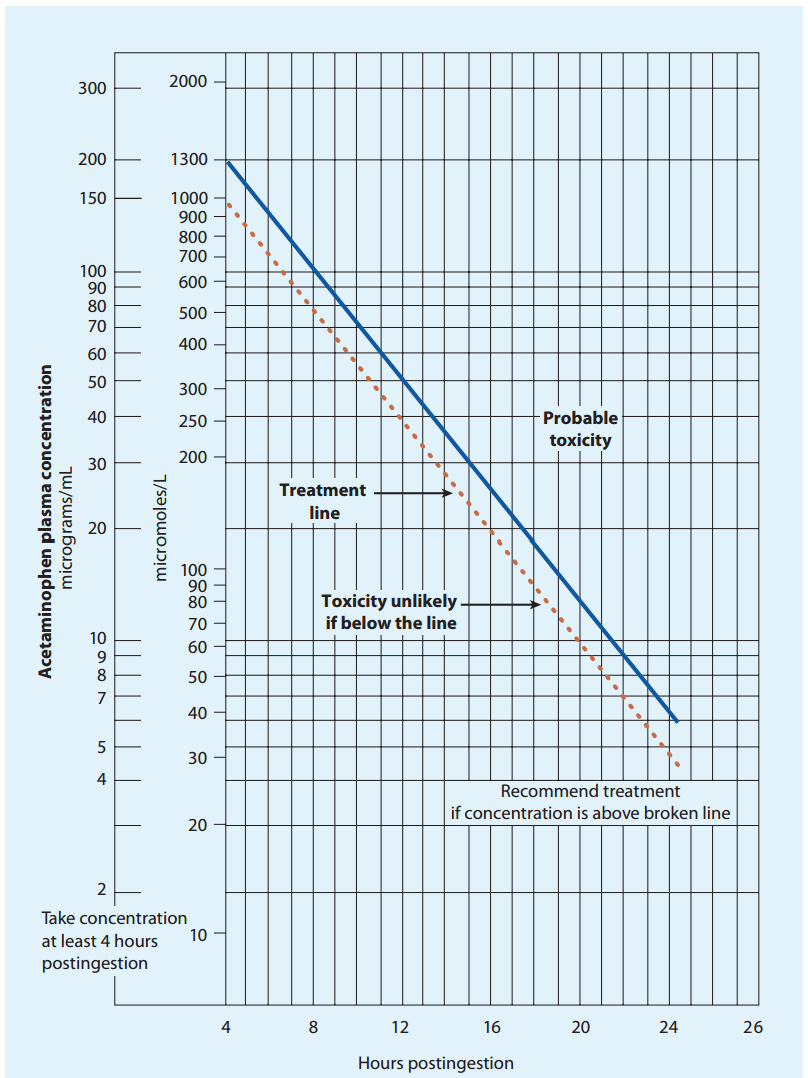
Why do we do acetaminophen levels at 4 hours?
- Late enough that peak absorption and distribution has occured
- Earlier the better for treatment
- Level at 4, 6 h if extended release
200
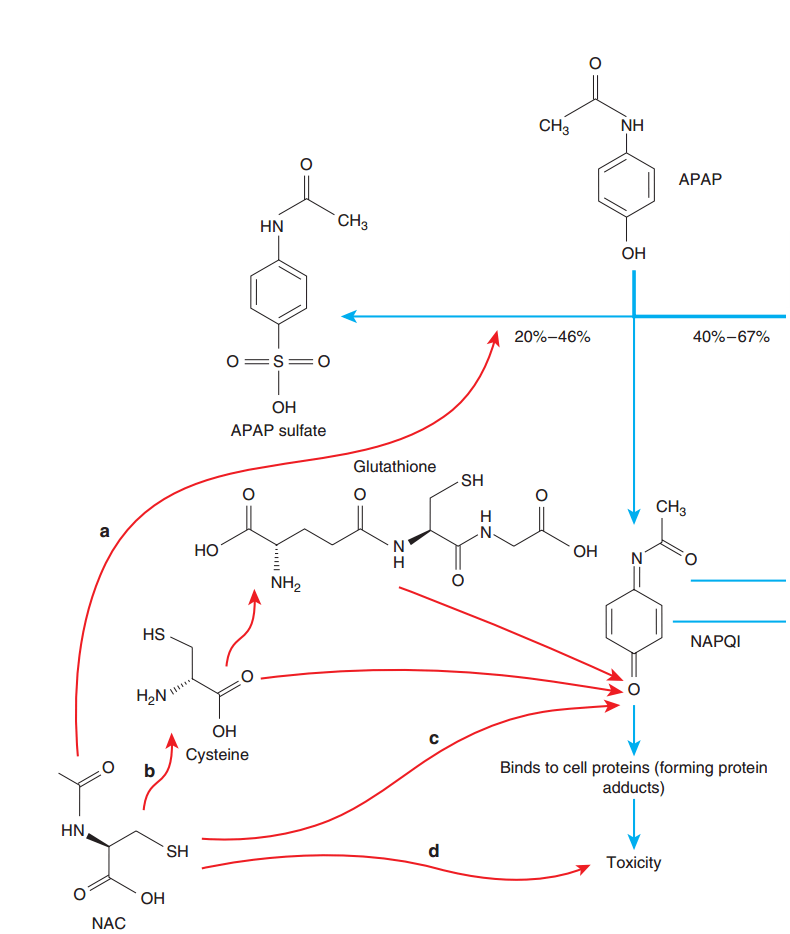
In overdose how is acetaminophen metabolized, why is this a problem?
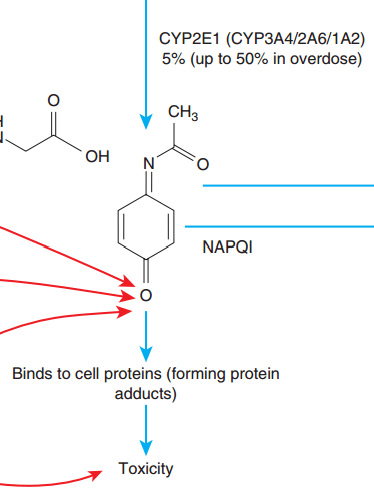
200
If you could only do AST or ALT which one would you do?
AST, rises faster
200
Name a treatment for Acetaminophen toxicity other than AC, NAC or Fomepizole
- Dialysis (APAP >5960 + altered LOC + acidosis)
- PLEX (perhaps if meets criteria for liver transplant but not a candidate) - removal of inflammatory mediators, liver support
200
NAC is nearly 100% effective if started before __ hours
8 hours
200
A patient ingested acetaminophen between 0200-0600
Acetaminophen level at 1000 = 700
Do you treat with NAC?
Yes, use earliest time of ingestion
300
In therapeutic doses, how is acetaminophen metabolized? (Name 1 of 2 pathways)
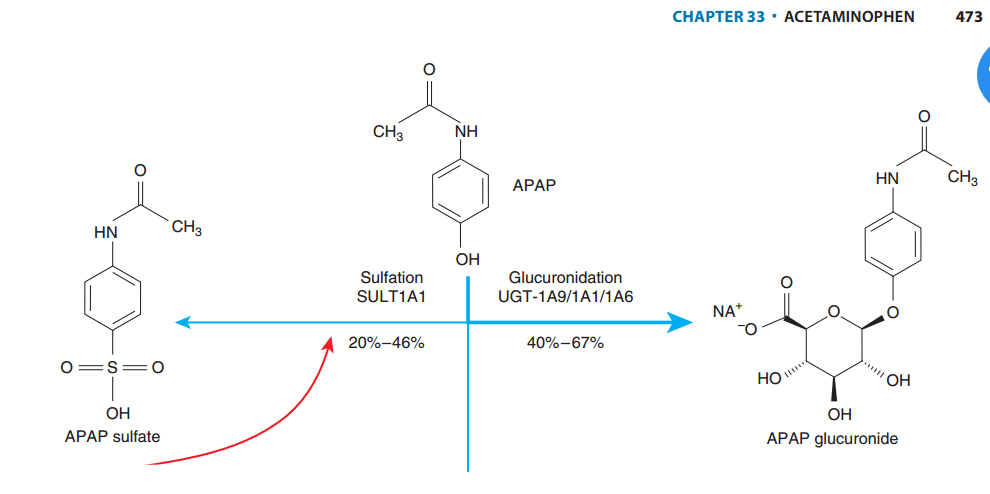
300
What is the mechanism of renal toxicity in acetaminophen overdose?
- Hepato-renal syndrome
- ATN due to local NAPQI CYP2E1 production
300
How would you determine whether a repeated SupraTherapeutic Ingestions (RSTI) requires NAC treatment
- AST/ALT above 3x ULN
- Acetaminophen above therapeutic level (>132 umol/L or 20 mcg/mL)
300
What are the stopping criteria for NAC? (5)
- Acetaminophen undetectable
- AST/ALT decreasing
- INR <2
- Cr N/decreasing
- LOC N
300
How does management differ for a pregnant patient with acetaminophen overdose?
It does not
400
How does N-AcetylCysteine treat acetaminophen overdoses (at least 2/3 ways)
- Limits formation of NAPQI (provides cysteine substrate for phase II metabolism)
- Increases capacity to detoxify NAPQI (cysteine is a substrate for glutathione needed to metabolize NAPQI)
- Treats toxicity (through nonspecific mechanisms)
400
List s/s associated with massive overdoses (at least 2)
Altered LOC, metabolic acidosis
rare: methemoglobinemia, hyperglycemia, hypothermia
Early (within 12 hours of ingestion)
Normal transaminases/hepatic function
400
Who would be the best population to give fomepizole to for acetaminophen toxicity?
- Massive overdoses (levels >3000)
- Late presentations
- Early acidosis
MOA: CYP2E1 inhibition, JNK inhibition (stops oxidant stress/mitochondrial injury)
400
What are the side effects to NAC, how can you manage them?
- Anaphylactoid reactions -> stop infusion, treat (antihistamine ?epi/steroids), resume at 1 h perhaps at reduced rate, ?PO
- Cerebral edema (from overdose) - stop infusion, neuro protection measures, hyperosmolar therapy
- N/V (from PO version)
400
What can cause a falsely elevated acetaminophen level?
Hyperbilirubinemia (> 171 umol/L), and usually in the low range (up to 200 umol/L)
500
Name 2 population who would be at higher risk for toxicity from overdose or repeated supratherapeutic ingestions
- Glutathione deficiency states (heavy ethanol users, febrile infants, catabolic post-surgical patients, anorexic patients)
- CYP- inducing medications (CYP 2E1 ex.INH) (chronic alcoholics)
500
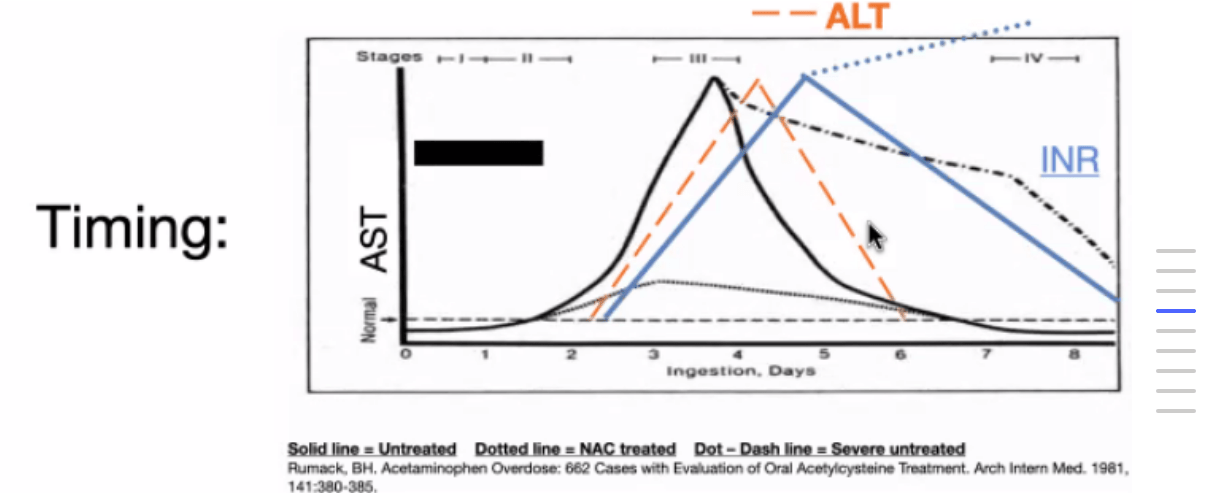
List the 4 stages of acetaminophen toxicity
Stage 1 - GI symptoms, Normal labs
Stage 2 - Onset of hepatic injury (12-36h)
Stage 3 - Hepatotoxicity (72-96h), AKI
Stage 4 - Death (ARDS, Sepsis, cerebral edema) or Recovery
500
Name 3 limitations of the Rumack-Matthew nomogram
- Limited in staggered overdoses
- When time of ingestion is note able to be determined (do earliest possible)
- Only accurate up to 24h
- IV overdoses
500
Who does not qualify for 12 hour stopping criteria
- Ingestion of XR/SR acetaminophen
- Co-ingestants that decrease gut motility (opioids, anticholinergics, NSAIDs)
- Aminotransferases or Cr abnormal at initial measurement
- INR >2 on initial measurement
500
What are the King's college criteria for liver transplant?
Arterial pH <7.3 or lactate >3 post fluid resuscitation
OR
All of:
- INR > 6.5
- Cr > 300
- Grade 3-4 encephalopathy (somnolence to stupor, confusion, gross disorientation)
600
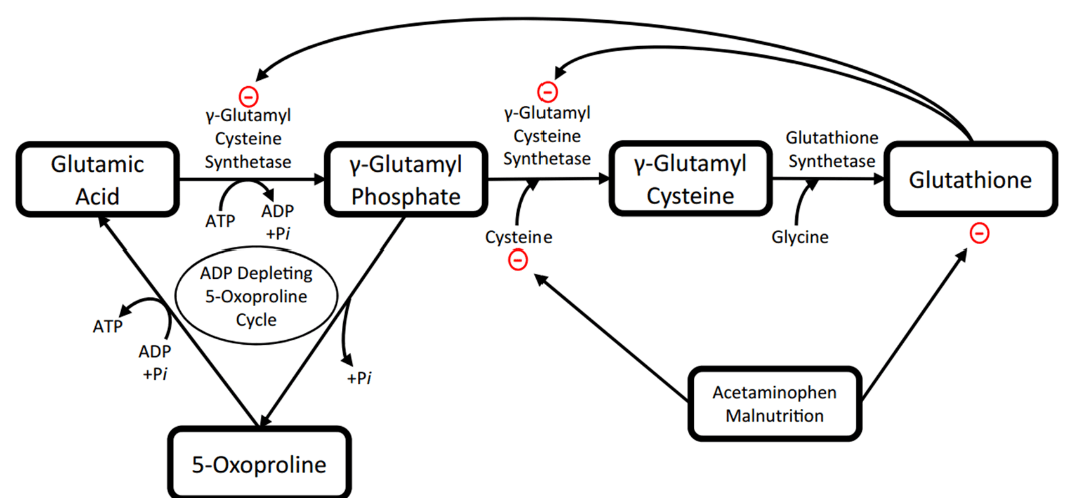
A 60 year old frail female with CKD is taking acetaminophen in therapeutic doses and presents with confusion and fatigue. Her K is low. Her pH is 7.25 with an anion gap of 17. Acetaminophen is 88. Lactate is normal.
What is the diagnosis?
Pyroglutamic Acidosis or 5-Oxoproline Acidemia
Tx: D/C acet, IV fluids, K supplemtantion, NAC?