Wild Bottom
Too Slow
Too Fast
EKGs
Post Arrest Care
100
What are the shockable arrhythmias?
Ventricular Fibrillation
Ventricular Tachycardia
100
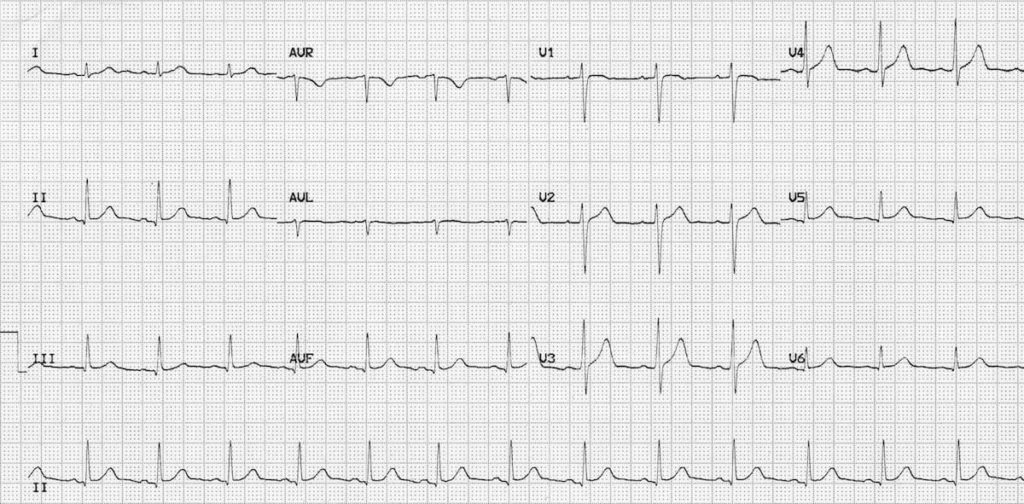
Paged: Mr. Kirby, admitted for an STEMI yesterday, is now HR 45bpm. He's fine. Just making you aware. His MI is likely located on what region of the heart
Inferior (RCA territory)
100
Rapid Response: Narrow complex tachycardia (HR 150s-160sbpm) with BP 80/50. Patient is fully awake. Repeat BP 72/41mmHg. Patient becoming confused and pulses weak. What should you do?
Synchronized cardioversion. Consider Sedation. Call EP (ASAP)
100
normal sinus rhythm
100
The Initial Stabilization Phase
Airway managements
12-lead EKG
200

Vfib
200
Ms. Harrison (84), admitted for failure to thrive, is becoming somnolent. No PMH. HR 28-32bpm. BP 101/72mmHg. What can you try first?
Atropine 1mg bolus
200
HR persistently 160s-170sbpm. BP 130/84mmHg, RR 22, 97% RA. Appears comfortable. Narrow complex, regular. Attempted carotid massage and Valsalva with no improvement. What is next?
Adenosine
200
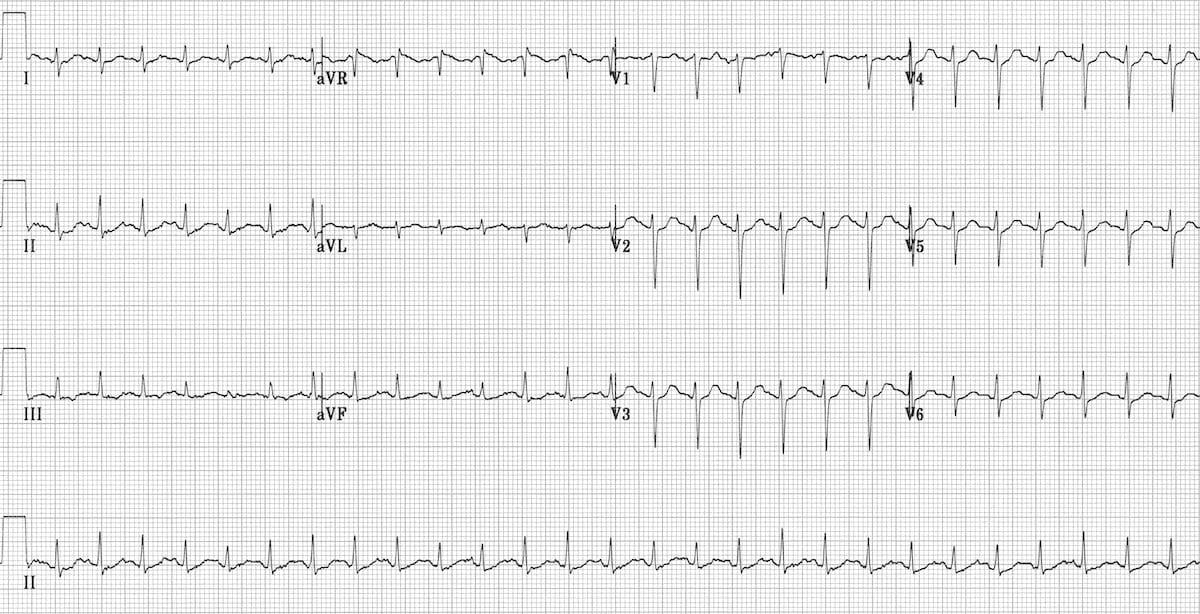
Sinus tachycardia
HR 150bpm
200
Investigations Post-Cardiac Arrest
Labs - rainbow (CMP, lactate, Blood cx). ABG after intubation
POCUS - lung (PTX), cardiac (tamponade, RV failure, volume)
Imaging - CXR, NCCT head. If not obvious, consider pan-scan
300
Reversible H's
Hypovolemia
Hypoxia
Hydrogen ion (acidosis)
Hypo-/Hyperkalemia
Hypothermia
300
Atropine did not work
Transcutaneous pacing
Dopamine infusion or Epinephrine infusion
300
True or false: Give adenosine for irregular wide-complex tachycardia or polymorphic tachycardia.
FALSE
300

Ventricular tachycardia
300
Reversible T's
Tension PTX
Tamponade Cardiac
Toxins
Thrombosis (pulmonary or coronary)
400
Recommended Joules for VF/pVT
Biphasic: 120-200J
Monophasic: 360J
400
Causes of Bradycardia with a Pulse
Myocardial ischemia/infarction
Drugs/ toxicologic (CCB, BB, digoxin)
Hypoxia
400
45yo woman with 3hours of palpitations. BP 80/50mmHg. Regular, narrow-complex tachycardia 180/min and normal QRS complex. No P waves. What are your options?
Valsalva maneuver
Carotid Massage
Verapamil
IV adenosine
400
Why is adenosine contraindicated for an irregular or polymorphic wide-complex tachycardia?
Can cause unopposed retrograde conduction through an accessory pathway leading to ventricular tachycardia or fibrillation
400
Goal SBP and/or MAP post arrest
Goal SBP >90mmHg or MAP >65mmHg
500
True or False: Amiodarone can be given for asystole/PEA.
FALSE
500

Third Degree AV block
atrial rate 85bpm
ventricular rate 42bpm
Junctional escape rhythm
500
Common SVTs (excluding AF and atrial flutter)
AVNRT
AVRT
atrial tachycardia
500
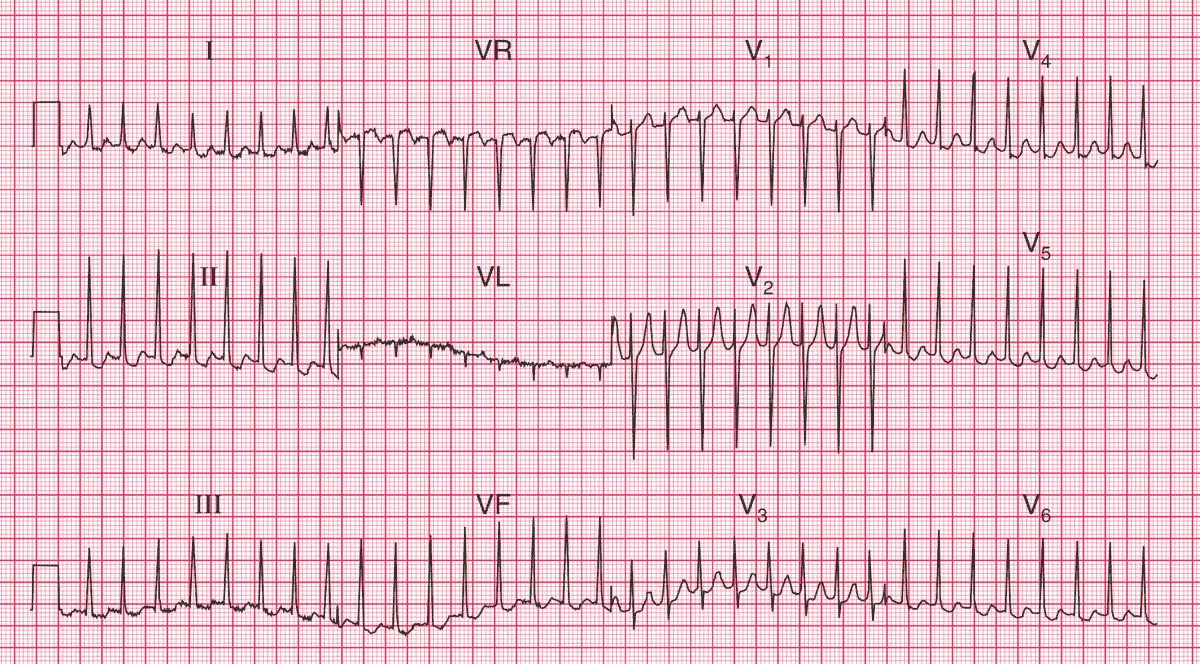
SVT - AVNRT
Termination with adenosine often suggests AV node dependence (AVNRT and AVRT). Continues P waves helps identify atrial flutter and atrial tachycardia.
500
When should targeted temperature management (TTM) be used?
ACLS - not following commands
Goal is to aggressively maintain normothermia and avoid temperatures >37.8C (continuous temperatures probes) based on TTM2 trial. No evidence to support TTM benefit over maintain normocardia