No Germs Aloud!
Urine the Right Track
Protecting the Barrier
Under Pressure
What Wound Michelle Do!
100
Sterile gloves become contaminated when they touch this.
What is a non-sterile surface?
100
What term describes excessive urine output?
Polyuria
100
This is the skin’s primary function in maintaining health.
What is protection?
100
This is the most common site for pressure injuries in patients who are supine.
What is the sacrum?
100
This term describes a break in the skin or mucous membrane.
What is a wound?
200
This part of a sterile gown is considered sterile.
What is the front of the gown from chest to waist?
200
What is the normal adult urine output per hour?
30 mL/hr or greater
200
Potter & Perry identify this as a key factor that delays wound healing.
What is poor nutrition?
200
A Stage 1 pressure injury is characterized by this key finding.
What is nonblanchable erythema?
200
This phase of wound healing involves clot formation and vasoconstriction.
What is the hemostasis phase?
300
This area of a sterile field is considered contaminated.
What is anything below waist level?
300
The functional unit of the kidney is called the _____.
Nephron
300
Potter & Perry recommend repositioning immobile patients at least every this many hours.
What is two hours?
300
This stage of pressure injury involves partial-thickness skin loss with exposed dermis.
What is Stage 2?
300
This phase is marked by redness, warmth, swelling, and pain. Diabetic pts often stay in this stage.
What is the inflammatory phase?
400
Reaching across a sterile field without proper technique causes this.
What is contamination?
400
This type of urinary diversion is shown by the presence of a stoma with continuous urine drainage into an external pouch, commonly created after bladder removal.
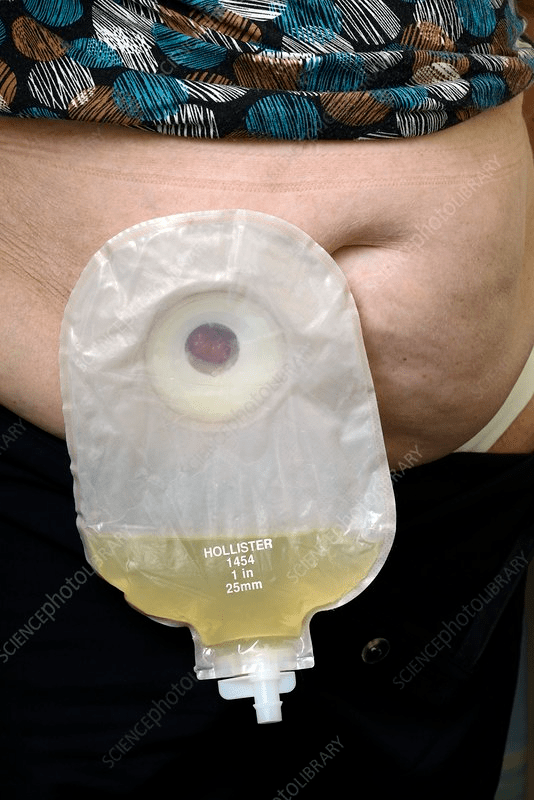
What is a urostomy (ileal conduit)?
400
Sliding down in bed with the head of bed elevated primarily increases this risk factor.
What is shearing force?
400
This stage includes full-thickness skin and tissue loss with visible bone, tendon, or muscle.
What is Stage 4?
400
3 factors contribute to pressure injury development:
What is
•Pressure intensity
•Pressure duration
•Tissue tolerance
500
These must be checked before use to ensure sterility.
What is the integrity of packaging and expiration dates?
500
A patient voids small amounts frequently and feels bladder fullness. This condition is known as what?
What is Urinary retention?
500
Older adults are at increased risk for skin breakdown due to decreased this.
What is skin elasticity or turgor?
500
This commonly used tool assesses a patient’s risk for pressure injury development.
What is the Braden Scale?
500
Name 3 of the 6 subscales on a Braden scale to assess level of risk
What is
Sensory perception
Moisture
Activity
Mobility
Nutrition
Friction
600
Sterile solutions are poured this way to avoid contamination.
What is away from the label and without splashing?
600
What condition occurs when urine leaks unexpectedly due to increased intra-abdominal pressure (coughing, sneezing)?
What is Stress incontinence?
600
This nursing intervention reduces shear and friction.
What is using a slider sheet?
Also acceptable: Lifter or bed pad
600
Adequate intake of this nutrient is especially important for skin repair and wound healing.
What is protein?
600
Name 3 acceptable terms used to describe the amount of exudate on wound dressing and include the % of the dressing that is required to saturated.... hint Scant = wound tissue moist, no drainage in dressing
Small:
•Wound tissues wet, moisture evenly distributed in wound, drainage involves 25% of dressing.
Moderate:
•Wound tissues saturated, drainage may or may not be evenly distributed in wound, drainage involves 25%-75% of dressing.
Large:
•Wound tissues bathed in fluid, drainage freely expressed, may or may not be evenly distributed in wound, drainage involves 75% of dressing.
700
This part of sterile gloves is considered non-sterile after donning.
What are the cuffs?
700
A patient with spinal cord injury lacks awareness of bladder filling. This is known as what type of bladder dysfunction?
What is Neurogenic bladder?
700
Keeping the skin clean and dry helps prevent this common problem.
What is skin breakdown?
700
Name 5 Risk factors for Pressure Injury Development.
What is
•Impaired sensory perception
•Impaired mobility
•Alteration in level of consciousness
•Shear
•Friction
•Moisture
•Nutrition
•Tissue perfusion
•Infection
•Pain
•Age
•Psychosocial impact of wounds
700
Wounds are measured in what numerical denomination and listed in what order.
What is LxWxD in centimeters?
800
While wearing a sterile gown, the nurse clasps hands below the waist while waiting. This breaks sterility because this area is considered what.
What is non-sterile?
800
A postoperative patient has a bladder scan showing 850 mL but no urge to void. What is the most appropriate nursing action?
What is notify the physical immediately to report findings and get an order to catheterize the patient.
800
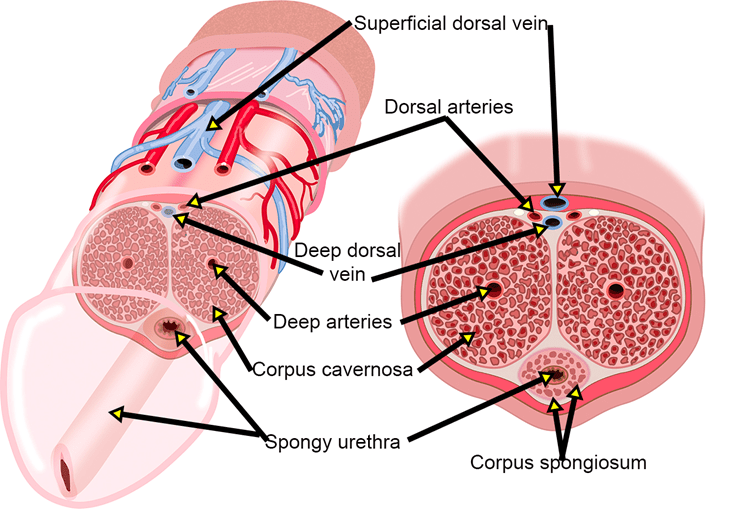
This skin layer contains blood vessels, nerves, sweat glands, and hair follicles.
What is the dermis?
800
This risk factor causes an increase in risk for pressure ulcer development when the HOB is elevated, and the skeleton starts to slide but the skin is fixed because of friction with the bed.
What is shear?
800
Name 5 Classic Signs of Wound Infection
What is
•Pain & Tenderness at the wound site
•Erythema (reddening of the surrounding tissue)
•Edema (swelling), induration (increase firmness of the tissue
•Inflammation of wound edges
•Purulent discharge
•Warmth in surrounding tissue
•Fever, chills
•Foul odor
•Elevated WBC’s
•Delayed healing
900
A sterile drape becomes wet from a prep solution. The top surface appears dry. According to aseptic principles, the drape is considered this because of this phenomenon.
What is airborne contamination d/t strike-through contamination?
900
Name the type and purpose of each of the ports for this catheter:
What is a three-way catheter, drainage, inflation and solution installation port.
900
This layer stores fat, insulates the body, and cushions organs.
What is the subcutaneous layer (hypodermis)?
900
This risk factor prolongs the inflammatory phase, delays collagen synthesis, prevents epithelialization and increases the production of proinflammatory cytokines, which leads to additional tissue destruction.
What is infection?
900
Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure or shear or both.
What is a Deep Tissue Injury?
1000
A nurse opens a sterile kit on a table, reaches across it to grab supplies, then turns to answer a question while keeping the kit in sight. Name TWO breaks in sterile technique.
What are reaching across the sterile field and turning away from the sterile field?
1000
If a male catheter is not properly secure this condition can occur.
What is Urethral erosion?
Also acceptable:
Iatrogenic Hypospadias
Meatal erosion or meatal cleft
Ventral urethral dehiscence
Urethral laceration with glans splitting
1000
Nurses are warned to avoid friction and shear because elderly skin behaves like this when moist.
What is wet tissue paper?
1000
Two considerations are related to duration of pressure:
What is
Low pressure over a prolonged period of time.
High intensity pressure over short period of time
1000
When assessing a wound, this clear watery drainage is normal early in healing, this blood-tinged drainage is commonly seen in surgical wounds, and this thick yellow or green drainage often indicates infection.
What are serous, serosanguineous, and purulent exudates?