Elevated and Complicated
Catch Your Breath
Marrow Matters
Stomach on Strike
Brain Rot
100
A 55-year-old woman is evaluated for a 5-month history of fatigue and constipation. More recently, she has experienced polydipsia and polyuria. She has no other medical problems.
Physical examination findings, including vital signs, are normal. Serum albumin level is 4.5 g/dL (45 g/L), calcium level is 11.4 mg/dL (2.9 mmol/L), and phosphorus level is 2.2 mg/dL (0.71 mmol/L). Complete blood count, anion gap, and kidney function are normal.
Which of the following should be measured next?
A. Calcitonin
B. 25-Hydroxyvitamin D and 1,25-dihydroxyvitamin D
C. Ionized calcium
D. Parathyroid hormone level
The first step in diagnosing hypercalcemia is to determine the parathyroid hormone (PTH) level with an assay for intact PTH (Option D).
If the PTH level is high or “inappropriately” normal, primary hyperparathyroidism is the diagnosis. If the PTH level is suppressed, a search for other entities that cause hypercalcemia must be conducted. Primary hyperparathyroidism is typically caused by a solitary parathyroid adenoma. Because PTH enhances kidney phosphate excretion, low or low-normal serum phosphorus concentrations support the diagnosis.
Calcitonin (Option A) is secreted by thyroid parafollicular C cells. This serum level is elevated in patients with medullary thyroid cancer or C-cell hyperplasia. Calcitonin tends to lower the calcium level, but the effect is weak and relevant only in pharmacologic amounts. Measurement of serum calcitonin is not indicated in a patient with hypercalcemia.
One of the ways in which PTH increases the serum calcium level is by upregulation of the 1α-hydroxylase enzyme, which stimulates conversion of vitamin D to its most active form, 1,25-dihydroxyvitamin D. This form of vitamin D increases the percentage of dietary calcium absorbed by the intestine. Body stores of vitamin D are assessed by measuring 25-hydroxyvitamin D, which has a long half-life. Measurement of this patient's 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels (Option B) may be appropriate after measuring serum PTH, particularly if the PTH level is suppressed; however, this should not precede measurement of serum PTH.
Ionized calcium measurement (Option C) is not necessary if the serum albumin or corrected total calcium levels are normal, there are no acute acid-base disorders, or there is no evidence of paraproteinemia, such as multiple myeloma (anemia, kidney injury, low anion gap). In most clinical situations, measured calcium levels depend on the amount bound to albumin, which may be affected by nutrition and acid-base status. When albumin concentration is low, ionized calcium measurement or corrected total calcium calculation is required to accurately assess calcium levels. This patient's albumin level is normal, and she has symptoms of hypercalcemia; ionized calcium does not need to be measured.
100
A 44-year-old man is evaluated for shortness of breath. Point-of-care ultrasonography of the lungs is performed. An ultrasound video with the probe placed at the left fifth intercostal space in the posterior axillary line is shown.
Which of the following is the most likely cause of this patient's symptoms?
A. Pleural effusion
B. Pneumonia
C. Pneumothorax
D. Pulmonary fibrosis
This ultrasound finding is most consistent with a pleural effusion (A).
The right of the screen shows the diaphragm (white) moving with respiration. The lung is visible moving in a large collection of fluid, which appears black. The vertebral bodies at the bottom of the screen, usually hidden by aerated lung, can be seen through the collection of fluid cephalad to the diaphragm.
100
A 59-year-old man is evaluated for anemia, acute kidney injury, and lytic bone lesions.
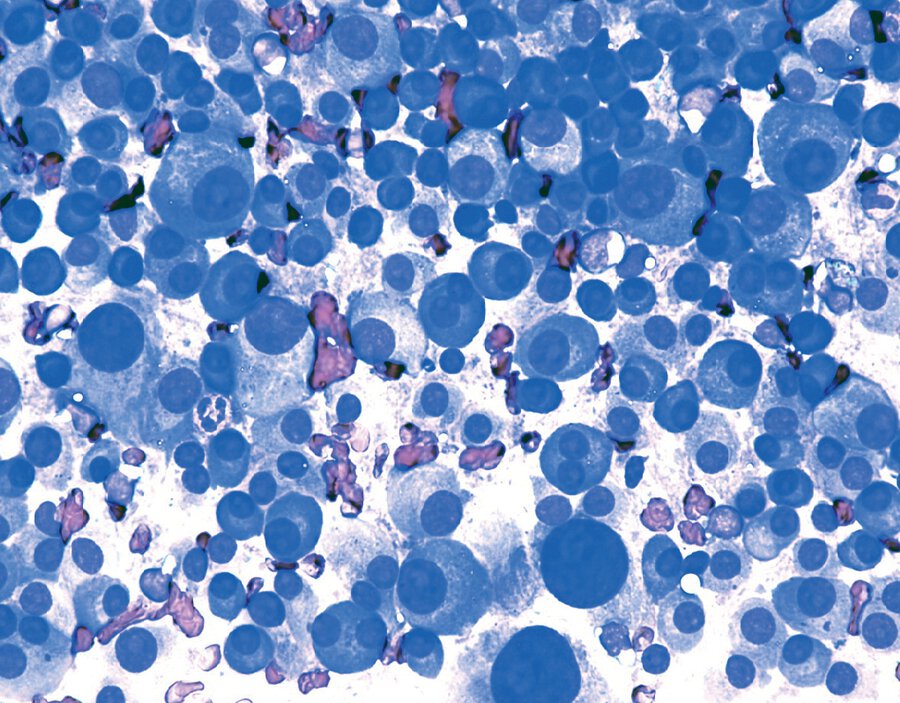
A bone marrow biopsy is shown.
Which of the following is the most likely diagnosis?
A. Metastatic adenocarcinoma
B. Multiple myeloma
C. Myelodysplastic syndrome
D. Polycythemia vera
The most likely diagnosis is multiple myeloma (option B).
This patient's bone marrow is packed with plasma cells that have findings typical for mature plasma cells. The cells are oval and nearly filled with basophilic cytoplasm. The nucleus is round and eccentric, and an area of cytoplasmic clearing (“perinuclear hof”) is seen near the nucleus (arrow).
100
A 40-year-old woman is evaluated for a 3-month history of epigastric pain, bloating, abdominal fullness, nausea, and diarrhea 30 to 60 minutes after meals that is worse with larger meals. She sometimes experiences headaches and feels sweaty after larger meals. Symptoms usually improve gradually 30 minutes to 2 hours after eating. She has obesity, type 2 diabetes mellitus, and hypertension. She underwent sleeve gastrectomy 4 months ago. Current medications are omeprazole, promethazine, metformin, and lisinopril. Vital signs and other physical examination findings are unremarkable. BMI is 35.
Upper endoscopy findings are notable only for gastric sleeve anatomy. Gastric biopsy specimens are negative for Helicobacter pylori. Duodenal biopsy specimens (for celiac disease) are normal. Result of a gastric emptying study is normal.
Which of the following is the most appropriate treatment?
A. Acarbose
B. Metoclopramide
C. Rifaximin
D. Smaller, more frequent meals
The most appropriate treatment is smaller, more frequent meals (Option D).
This patient most likely has dumping syndrome as a consequence of her sleeve gastrectomy. Dumping syndrome can follow a variety of surgical procedures, including vagotomy, pyloroplasty, Roux-en-Y bypass, sleeve gastrectomy, and esophagectomy. Early dumping syndrome, as in this patient, results from the rapid transition of food into the small intestine, causing a fluid shift and potential release of gastrointestinal hormones with vasoactive properties. Classic gastrointestinal symptoms can include abdominal pain, epigastric fullness, diarrhea, nausea, vomiting, borborygmi, and bloating. Classic vasomotor symptoms can include palpitations and tachycardia, faintness or syncope, diaphoresis, and flushing and pallor. Symptoms typically occur within 1 hour of eating. Treatment should be tiered, beginning with dietary modifications and patient education by a trained dietitian. Dietary interventions can include the pursuit of smaller and more frequent meals (at least six per day); delayed intake of fluids by at least 30 minutes after intake of solids; avoidance of rapidly absorbable carbohydrates and alcohol; increased intake of high-fiber, high-protein foods; and lying down after a meal for 30 minutes. The use of dietary supplements, such as guar gum or pectin, to increase food viscosity can also be helpful.
Pharmacologic interventions can be considered when the previously mentioned measures fail, although no pharmacologic treatment has been approved for dumping syndrome. The currently available options include acarbose (Option A) and, in severe cases, somatostatin analogues. Acarbose, an α-glycosidase hydrolase inhibitor that interferes with digestion of polysaccharides to monosaccharides, can be used for late symptoms of dumping syndrome if dietary intervention is only partially successful.
Metoclopramide (Option B) is a prokinetic approved for the treatment of gastroparesis. However, this patient does not have gastroparesis, as documented by the normal results of a gastric emptying study.
Rifaximin (Option C) is indicated for irritable bowel syndrome with diarrhea, which this patient does not have.
100
This artist led the 2026 iHeartRadio Music Awards with 9 nominations.
Taylor Swift
200
A 33-year-old woman is evaluated for persistent mild hypercalcemia that was incidentally discovered several years ago. Her father also has persistent, asymptomatic hypercalcemia. The patient has no medical concerns and takes no medications. She takes vitamin D, 5000 IU, daily. Physical examination is normal.
Laboratory studies:
Calcium: 10.7 mg/dL (2.7 mmol/L)
24-Hour urine calcium: 40 mg/24 h
Creatinine: 1.0 mg/dL (88.4 μmol/L)
Calcium-creatinine clearance ratio: 0.008
Parathyroid hormone: 40pg/mL (40 ng/L)
Which of the following is the most likely diagnosis?
A. Ectopic parathyroid hormone–secreting tumor
B. Familial hypocalciuric hypercalcemia
C. Multiple endocrine neoplasia type 1
D. Vitamin D toxicity
The most likely diagnosis is familial hypocalciuric hypercalcemia (FHH) (Option B).
The parathyroid glands and kidney detect serum calcium concentrations through the calcium-sensing receptor (CaSR). In FHH, inactivating mutation of the CaSR gene causes the parathyroid gland to perceive serum calcium levels as low, resulting in increased parathyroid hormone (PTH) secretion and a higher serum calcium level. Simultaneously, the mutated CaSR in the kidney increases kidney reabsorption of calcium, leading to paradoxical hypocalciuria in the setting of hypercalcemia. Although these patients appear to have primary hyperparathyroidism, FHH is a benign condition that will not resolve with parathyroidectomy. Patients do not have sequelae of hypercalcemia, such as stones or osteoporosis. Signs suggestive of FHH include mild hypercalcemia since childhood; low 24-hour urine calcium excretion, especially if the calcium-creatinine clearance ratio is less than 0.01; and/or family history of parathyroidectomy without resolution of hypercalcemia. Although testing for mutations in the CaSR gene is a more direct approach, not all affected families have mutations in this gene, yet all will have a low calcium-creatinine clearance ratio. PTH values in FHH may be slightly above or within the reference range and, as such, do not help distinguish primary hyperparathyroidism from FHH.
An ectopic PTH-secreting tumor (Option A) is a relatively rare cause of hypercalcemia and is described in a limited number of case reports. Although ectopic PTH secretion can cause elevated PTH and calcium levels, it is not associated with hypocalciuria.
Primary hyperparathyroidism in adolescents and young adults may be the first sign of multiple endocrine neoplasia (MEN) syndrome (Option C). Primary hyperparathyroidism is associated with MEN1 and MEN2A syndromes. In contrast to sporadic primary hyperparathyroidism, patients with MEN syndromes have hyperplasia of multiple parathyroid glands. However, patients with MEN-associated hypercalcemia have elevated urine calcium, often occurring before hypercalcemia occurs. This patient's urine calcium excretion is low.
Although this patient is taking a high dose of vitamin D, in the absence of other causes of hypercalcemia and/or without concomitant generous calcium intake, a supplement of 5000 IU/d of vitamin D will not cause toxicity (Option D) or hypercalcemia. If excess vitamin D action were responsible for this patient's hypercalcemia, PTH would be suppressed and urine calcium excretion increased. This patient has elevated PTH in relation to the serum calcium and low urine calcium excretion; neither is compatible with the diagnosis of vitamin D toxicity.
200
A 59-year-old man is hospitalized with acute hypoxemic respiratory failure requiring intubation.
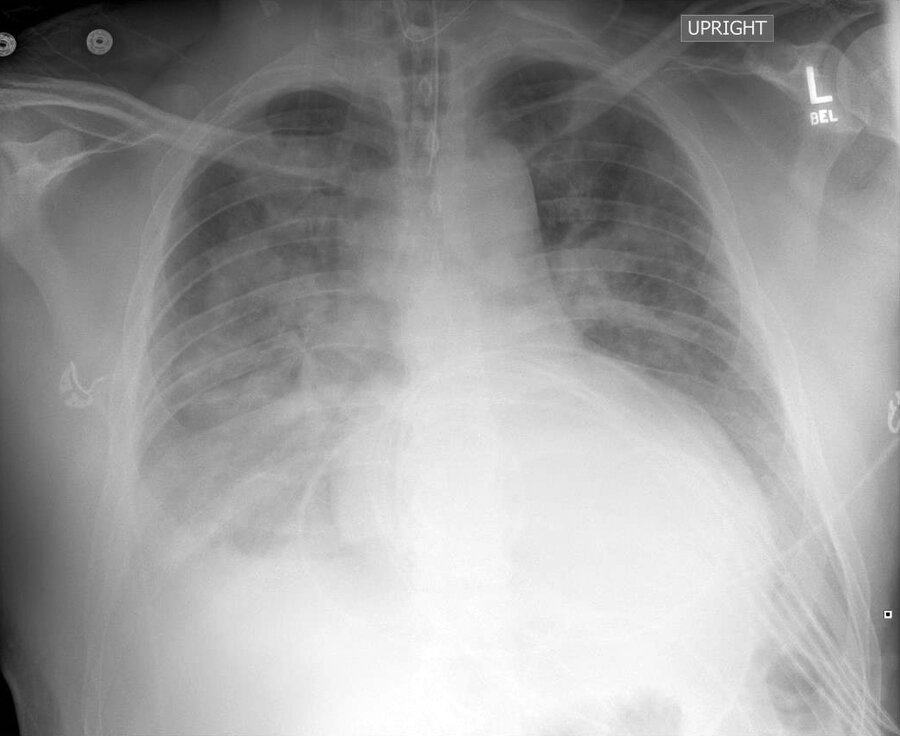
A frontal chest radiograph is shown.
Which of the following is the most likely diagnosis?
A. Atelectasis
B. Mucous impactions
C. Multilobar pneumonia
D. Pulmonary emboli
This frontal chest radiograph reveals bilateral alveolar opacifications with air bronchograms, consistent with multilobar pneumonia (option C).
The right and left hemidiaphragms are each partially obscured, with placement of infiltrates in the right and left lower lobes, respectively. The right heart border is partially obscured, and an infiltrate within the right middle lobe is also possible.
200
A 55-year-old woman is evaluated before starting chemotherapy for multiple myeloma. Anticipated therapy will include bortezomib, lenalidomide, dexamethasone, and daily low-dose aspirin. She has otherwise been well, has no symptoms, and has no previous history of venous thromboembolism (VTE) or risk factors for VTE. She takes no medications. Today, her hemoglobin level is 9 g/dL (90 g/L).
Inactivated influenza and 20-valent pneumococcal conjugate vaccines will be administered today. The patient received the herpes zoster virus recombinant vaccine at age 50 years.
Which of the following is the most appropriate additional treatment during chemotherapy?
A. EPO
B. Fluconazole
C. Metronidazole
D. Valacyclovir
In addition to chemotherapy, this patient should receive prophylactic therapy with valacyclovir to prevent herpes zoster virus reactivation (Option D).
She is immunocompromised because of her plasma cell dyscrasia. Treatment guidelines for patients with multiple myeloma (MM) recommend that those treated with proteasome inhibitors (e.g., bortezomib) should receive antiviral prophylaxis (acyclovir, valacyclovir) to avoid herpes zoster virus reactivation. Prophylaxis should be administered regardless of previous immunization against herpes zoster virus.
This patient should not receive epoetin, an erythropoietin-stimulating agent (ESA) (Option A). The American Society of Clinical Oncology and the American Society of Hematology recommend restricting ESA use to patients with chemotherapy-associated symptomatic anemia when cancer treatment is not curative in intent to reduce the need for erythrocyte transfusions. ESAs are not recommended for patients whose cancer treatment is curative in intent, given the risk of ESA-related cancer progression. Although this recommendation is viewed by some as controversial, this patient's anemia is asymptomatic and does not require treatment with either an ESA or erythrocyte transfusion.
Antibiotic prophylaxis with trimethoprim-sulfamethoxazole or levofloxacin is often administered during induction chemotherapy because of the high rate of infection with gram-negative and encapsulated bacteria during the first 3 months of therapy. Trimethoprim-sulfamethoxazole has been shown to decrease the number of bacterial infections and serious infections, and levofloxacin prophylaxis has been associated with significantly fewer deaths and febrile episodes during this time period. The planned myeloma treatment is not associated with increased risk of fungal infection; therefore, prophylaxis with fluconazole is not indicated in this patient (Option B). Additionally, metronidazole has no activity against encapsulated bacteria, a common source of infection in patients with MM, and is not indicated (Option C).
200
A 68-year-old woman is evaluated for a 5-month history of postprandial fullness. She has hypothyroidism treated with levothyroxine and a remote history of adequately treated Helicobacter pylori infection.
Abdominal examination is normal. Vitiligo and absent vibratory sensation in the lower extremities are noted. Hemoglobin level is 10 g/dL (100 g/L) with a mean corpuscular volume of 114 fL. Result of stool antigen test for H. pylori is negative.
Which of the following is the most likely diagnosis?
A. Chronic autoimmune atrophic gastritis
B. Erosive gastropathy
C. Gastroparesis
D. H. pylori infection
This patient has a medical history, clinical manifestations, and physical findings that support the diagnosis of chronic autoimmune atrophic gastritis (CAAG) (Option A).
CAAG is an autoimmune disorder that leads to replacement of the normal gastric mucosa by intestinal metaplastic cells. The disease is more common in women older than 60 years and presents with nonspecific symptoms that affect the gastrointestinal tract and nervous system. Abnormal vibratory sensation and proprioception may develop due to degeneration of the posterior and lateral columns of the spinal cord. Patients typically have low vitamin B12 levels and macrocytic anemia (pernicious anemia), but younger persons with earlier disease may present with iron deficiency. CAAG is commonly associated with chronic thyroiditis and autoimmune conditions, such as type 1 diabetes mellitus, Addison disease, and vitiligo. Diagnosis may require a combination of clinical, serologic, and histologic information. Parietal cell antibodies are sensitive but also may be found in other autoimmune conditions; conversely, intrinsic factor antibodies are highly specific but not sensitive. Upper endoscopy reveals atrophic and polypoid changes, although abnormalities may not be present in the early stages. CAAG is a precancerous condition that increases the risk for gastric adenocarcinoma and neuroendocrine tumors. Goals of therapy for autoimmune atrophic gastritis include prevention of pernicious anemia and iron deficiency with vitamin B12 supplementation and iron replacement, along with surveillance for gastric neoplasm. Screening upper endoscopy with gastric biopsy is recommended in the setting of pernicious anemia. Otherwise, there are no universally accepted surveillance protocols for gastric neoplasm in chronic atrophic gastritis, and endoscopic surveillance should be considered on an individual basis.
200
This highly successful movie from 2025 recently won 4 Oscars after a record-breaking 16 nominations.
Sinners
300
A 66-year-old man is evaluated for increased confusion and lethargy over the past 2 days, as well as nausea and vomiting. He has also had diffuse bone pain that began 6 weeks ago and has worsened over the past month. His medical history is otherwise unremarkable, and he takes no medications.
On physical examination, temperature is 36.4 °C (97.6 °F), blood pressure is 110/60 mm Hg, pulse rate is 110/min, and respiration rate is 16/min. He is somnolent but can be aroused. Mucous membranes are dry, and he has decreased skin turgor. Cardiopulmonary examination is normal.
Results of laboratory studies show an albumin level of 3.8 g/dL (38 g/L), calcium level of 14.8 mg/dL (3.7 mmol/L), and creatinine level of 2.5 mg/dL (221 µmol/L).
Which of the following is the most appropriate initial management?
A. Denosumab
B. Intravenous isotonic saline and calcitonin
C. Intravenous isotonic saline and furosemide
D. Zoledronic acid
This patient has hypercalcemia, likely due to malignancy, and should be treated urgently with intravenous isotonic saline and calcitonin (Option B).
Hypercalcemia of malignancy occurs in 20% to 30% of patients with advanced cancer. It is most frequent in patients with myeloma and cancer of the lung, breast, kidney, head, and neck. Patients with severe or symptomatic hypercalcemia should receive isotonic saline volume expansion, which will increase renal perfusion and urine calcium excretion. The administration of isotonic saline at an initial rate of 200 to 300 mL/hour that is then adjusted to maintain the urine output at 100 to 150 mL/hour is a reasonable goal. Calcitonin increases kidney excretion of calcium and decreases bone resorption; it can decrease calcium within several hours in responsive patients. Tachyphylaxis to calcitonin may appear after 24 to 48 hours, so therapy is usually discontinued after this time period. This patient has an elevated serum creatinine level, which is a common complication of hypercalcemia, and intravenous isotonic saline may improve renal function as well.
Denosumab (Option A), a receptor activator of nuclear factor κB ligand inhibitor, is very effective in reducing serum calcium levels, but its effect is slower than isotonic saline and calcitonin, and it would not be the first treatment used in this situation. It has typically been reserved for patients who do not respond to bisphosphonate therapy, although some expert guidelines now recommend it over bisphosphonates. Denosumab can be used when bisphosphonate therapy is contraindicated, such as in patients with kidney failure. Patients receiving denosumab should be monitored for the subsequent development of hypocalcemia.
Furosemide (Option C), a loop diuretic, is not recommended unless kidney failure or heart failure is present, in which case volume expansion should precede the administration of furosemide to avoid hypotension and further kidney injury.
Bisphosphonates (Option D) are effective medications for correcting hypercalcemia of malignancy and are frequently used as a key part of management. However, their maximum effect occurs in 2 to 4 days, so they are usually given in conjunction with intravenous isotonic saline. Bisphosphonates are contraindicated in the setting of kidney failure.
300
A 65-year-old man is admitted to the hospital with a COPD exacerbation characterized by increased cough and sputum production. He is emergently evaluated 24 hours after admission for acute on chronic respiratory failure.
Chest radiograph is shown.

Which of the following is the most likely diagnosis?
A. Left tension pneumothorax
B. Right consolidated pneumonia
C. Right mainstem bronchus mucous plug
D. Right pleural effusion
The most likely diagnosis is right mainstem bronchus mucous plug (option C).
This chest radiograph shows opacification of the right hemithorax, caused by right lung atelectasis. Atelectasis is the loss of gas within the lung, which reduces volume. In this case, atelectasis of the right lung has caused a rightward shift of the mediastinum, indicated by the rightward displacement of the trachea from the midline (arrow) and the left mainstem bronchus away from its normal position within the left hemithorax (arrowhead). Right lung atelectasis may be caused by an obstruction within the right mainstem bronchus, such as an endobronchial tumor or large mucous plug, as in this patient.
A massive pleural effusion could similarly cause complete opacification of the right hemithorax but would not result in a rightward deviation of mediastinal structures; if large enough, a right-sided effusion could cause leftward displacement of mediastinal structures. Similarly, pneumonia would be unlikely to cause mediastinal shift.
300
A 70-year-old man is evaluated in the emergency department for a 2-day history of worsening confusion as well as polyuria and polydipsia. Medical history is notable only for hypertension. His only medication is lisinopril. On physical examination, he is disoriented. Temperature is 37.0 °C (98.6 °F), blood pressure is 105/60 mm Hg, and pulse rate is 115/min. The mouth and axillae are dry, and skin tenting is observed.
Laboratory studies:
Hemoglobin: 9 g/dL (90 g/L)
Calcium: 13.4 mg/dL (3.4 mmol/L)
Creatinine: 7.1 mg/dL (628 µmol/L)
Protein , total: 9 g/dL (90 g/L)
Chest radiograph shows no infiltrate, but lytic lesions are seen on multiple ribs.
Which of the following is the most likely diagnosis?
A. Lymphoplasmacytic lymphoma
B. Monoclonal gammopathy of renal significance
C. Multiple myeloma
D. Smoldering multiple myeloma
The most likely diagnosis is multiple myeloma (MM) (Option C).
The diagnosis of MM requires biopsy evidence of a bony or extramedullary plasmacytoma or greater than 10% bone marrow clonal plasma cells or lymphoid cells; and any disease-specific symptoms and signs. The CRAB mnemonic is often used to identify myeloma-related symptoms and signs: hyperCalcemia, Renal failure, Anemia, and Bone disease.
Myeloma-defining biomarkers include a clonal bone marrow plasma cell percentage of 60% or greater, involved:uninvolved serum free light chain ratio of 100 or greater, and one or more focal lesions on MRI studies. Based on this patient's elevated total serum protein level, hypercalcemia, kidney injury, anemia, and bone lesions, he most likely has MM. He will require further evaluation, including identification of the M protein and bone marrow aspirate and biopsy.
Lymphoplasmacytic lymphoma varies in presentation, ranging from no symptoms to bulky lymphadenopathy, hepatosplenomegaly, cytopenias, and hyperviscosity syndrome (Option A). Patients present with weakness and fatigue, often secondary to anemia; fever, night sweats, and weight loss are the presenting symptoms in about one third of patients. This patient's clinical syndrome is not compatible with lymphoplasmacytic lymphoma.
Monoclonal gammopathy of renal significance (MGRS) is present when the criteria for monoclonal gammopathy of undetermined significance are met and are accompanied by kidney injury attributable to the underlying monoclonal protein (Option B). Findings suggestive of MM, such as hypercalcemia, bone disease, and anemia, are not present. Kidney biopsy is usually necessary to make the diagnosis of MGRS. This patient has evidence of bone disease and hypercalcemia, making MM the most likely diagnosis.
Patients with smoldering MM have an M spike on serum protein electrophoresis and 10% to 59% clonal plasma cells on bone marrow biopsy but lack CRAB symptoms and signs (Option D). This patient has MM-specific symptoms and signs, excluding smoldering MM.
300
A 52-year-old man is evaluated for daily nausea, bloating, and early satiety, along with occasional vomiting. His symptoms began shortly after he experienced a respiratory illness 6 weeks ago. He is otherwise healthy. He has not had fever, weight loss, abnormal bowel movements, or hematemesis. On physical examination, vital signs are normal. Epigastric distention is noted.
Laboratory studies:
Complete blood count: Normal
Comprehensive metabolic panel: Normal
Hemoglobin A1c: Normal
Thyroid-stimulating hormone: Normal
Antinuclear antibody titer: Normal
Upper endoscopy reveals retained food in the stomach but no other abnormalities. Four-hour gastric scintigraphy confirms delayed emptying.
Despite initiation of small, frequent meals, symptoms have persisted and interfere with quality of life.
Which of the following is the most appropriate treatment?
A. Domperidone
B. Erythromycin
C. Metoclopramide
D. Nortriptyline
E. No additional treatment
The correct answer is metoclopramide (Option C).
This patient has gastroparesis, most likely postviral. Gastroparesis is characterized by delayed gastric emptying in the absence of mechanical obstruction. It is commonly caused by diabetes mellitus but may also be caused by other conditions, such as a viral infection. This patient's symptoms have not responded to dietary management, and pharmacologic therapy is therefore indicated to improve gastric emptying and alleviate symptoms. Metoclopramide is the only prokinetic agent approved by the FDA for the treatment of gastroparesis and is considered first-line pharmacologic therapy. Although rare, neurologic adverse effects, such as tardive dyskinesia, can occur with metoclopramide therapy; therefore, the lowest effective dosage should be given. Therapy must be stopped immediately if neurologic adverse effects develop.
Domperidone (Option A) is as effective as metoclopramide in reducing symptoms of gastroparesis. It can be prescribed only through an FDA investigational new drug application, and access is relatively limited. It may be an option for patients who have not responded to metoclopramide, but it is not yet appropriate for this patient. In contrast to metoclopramide, domperidone does not cause neurologic adverse effects. However, it may prolong the QTc interval; baseline ECG and subsequent electrocardiography are thus advised.
Erythromycin (Option B) is considered second-line treatment of gastroparesis. It can improve symptoms and gastric emptying, but long-term oral therapy is limited by tachyphylaxis. Intravenous erythromycin is effective in the treatment of hospitalized patients with gastroparesis who require parenteral treatment. Because this patient has not yet received metoclopramide and is not hospitalized or in need of intravenous medication, erythromycin therapy is not indicated.
Nortriptyline (Option D) and other tricyclic antidepressants may help to alleviate gastroparesis symptoms but will not improve gastric emptying; in fact, these drugs may worsen gastric emptying. Tricyclic medications should be considered only in cases of refractory nausea and vomiting.
Although most postviral cases of gastroparesis typically resolve within 1 year, no additional treatment (Option E) would be inappropriate in this case. This patient has daily symptoms that have not responded to lifestyle changes and are affecting his quality of life. Prokinetic therapy is indicated.
300
This Puerto Rican rapper recently collaborated with GAP leading to a viral commercial featuring their hit song "Wassup".
Young Miko
400
A 52-year-old woman is evaluated for hypercalcemia that was incidentally discovered during a recent office visit. Serum calcium level was 10.7 mg/dL (2.7 mmol/L) three weeks ago. She is asymptomatic, has no other medical conditions, and takes no medications. On physical examination, vital signs are normal; the examination is unremarkable.
Laboratory studies:
Calcium: 10.9 mg/dL (2.7 mmol/L)
Creatinine: 0.9 mg/dL (79.6 μmol/L)
Parathyroid hormone: 58 pg/mL (58 ng/L)
24-Hour urine calcium: 290 mg/24 h
Which of the following is the most likely diagnosis?
A. Familial hypocalciuric hypercalcemia
B. Milk-alkali syndrome
C. Primary hyperparathyroidism
D. Surreptitious thiazide diuretic use
E. Vitamin D toxicity
The most likely diagnosis is primary hyperparathyroidism (Option C).
This patient has a mildly elevated serum calcium level associated with an inappropriately normal parathyroid hormone (PTH) level. Primary hyperparathyroidism is usually caused by a parathyroid adenoma, and calcium levels are often only mildly elevated. PTH levels may be frankly elevated or inappropriately normal (typically the upper half of the reference range), as seen in this patient. Hypercalciuria may be present in up to 30% of patients. Overt hypercalciuria or high-normal levels of urine calcium, as seen in this patient, can help distinguish primary hyperparathyroidism from familial hypocalciuric hypercalcemia, which typically presents with low urinary calcium excretion.
Although familial hypocalciuric hypercalcemia (FHH) may also present with mild hypercalcemia and elevated or inappropriately normal PTH levels, an elevated or high-normal urinary calcium level (>200 mg/24 h), as seen in this patient, excludes the diagnosis of FHH (Option A). In FHH, a mutation of the CaSR gene causes the parathyroid glands to perceive serum calcium concentrations as low, resulting in elevated PTH and calcium levels. The CaSR gene also causes kidney resorption of calcium, leading to paradoxical hypocalciuria, usually less than 100 mg/24 h. This patient does not have hypocalciuria, which makes the diagnosis of primary hyperparathyroidism more likely.
Milk-alkali syndrome is caused by ingesting large amounts of calcium, such as with excessive antacid use, and results in kidney impairment and metabolic alkalosis (Option B). PTH levels are usually suppressed. This patient has an inappropriately normal PTH level and is unlikely to have milk-alkali syndrome.
Surreptitious thiazide diuretic use may cause mild hypercalcemia through reduction of urinary calcium excretion (Option D). This effect is more likely in the setting of previously unrecognized disease, and thiazide diuretics may “unmask” primary hyperparathyroidism. When thiazide diuretics are thought to be the cause of hypercalcemia, the medication should be stopped and calcium and PTH levels should be rechecked. This patient has a high-normal urinary calcium excretion, so surreptitious thiazide diuretic use is unlikely.
Vitamin D toxicity is unlikely in this patient (Option E). Vitamin D toxicity suppresses PTH and decreases urinary calcium excretion, neither of which is occurring in this patient.
400
A 36-year-old man is evaluated for ventilator-associated pneumonia in the ICU, where he was transferred 3 days ago for respiratory failure owing to Guillain-Barré syndrome. Temperature is 38.6 °C (101.4 °F). Pulmonary examination reveals scattered rhonchi. Flaccid weakness is present in the arms and legs. Bronchoalveolar lavage culture grows methicillin-resistant Staphylococcus aureus. The isolate is susceptible to vancomycin, daptomycin, linezolid, and tigecycline. He is allergic to vancomycin. Chest radiograph shows right middle and lower lobe infiltrates without effusions.
Which of the following is the most appropriate treatment?
A. Daptomycin
B. Linezolid
C. Telavancin
D. Tigecycline
The most appropriate treatment is intravenous linezolid (Option B) for ventilator-associated pneumonia (VAP).
VAP notably accounts for approximately 20% of hospital-acquired infections and complicates 10% of ventilation episodes. Empiric VAP regimens include coverage for Staphylococcus aureus or Pseudomonas aeruginosa and other gram-negative bacilli. In this patient with methicillin-resistant S. aureus (MRSA) VAP and an adverse reaction to vancomycin, alternative therapy must be used. Linezolid is an oxazolidinone drug with bacteriostatic activity against gram-positive aerobic bacteria, including MRSA and vancomycin-resistant enterococci, and it has performed well in randomized controlled trials compared with vancomycin for pneumonia. The pharmacokinetics of linezolid in the lung are favorable, and it is an excellent alternative to vancomycin for treating MRSA. An important side effect of linezolid is myelosuppression, notably thrombocytopenia. Weekly complete blood counts should be obtained in patients treated with linezolid.
Daptomycin (Option A) is effective in treating staphylococcal bacteremia and right-sided infective endocarditis, in addition to skin and skin structure infections. It is equally effective for methicillin-sensitive S. aureus (MSSA) and MRSA infections. Although daptomycin is no more effective than β-lactams for treating MSSA infections, it may be a useful alternative to vancomycin for treating MRSA infections in patients with fluctuating kidney function or for isolates with a relatively high (≥2 µg/mL) vancomycin minimum inhibitory concentration. Daptomycin is bound by surfactant, however, and it is not effective in treating pneumonia.
Telavancin (Option C), oritavancin, and dalbavancin are analogues of vancomycin and are used for complicated skin and soft tissue infections. Telavancin is also approved for the treatment of VAP when other alternatives are not available. The incidence of hypersensitivity cross-reactivity with vancomycin is unknown, and alternative antibiotics should be used in the setting of an adverse reaction to vancomycin.
Tigecycline (Option D) is not approved for hospital-acquired (or ventilator-associated) pneumonia. An FDA warning reported increased mortality rates among patients treated with tigecycline in randomized controlled trials of patients with hospital-acquired pneumonia. Consequently, tigecycline should not be used for treating VAP.
400
A 63-year-old woman is evaluated after a recent diagnosis of multiple myeloma. The diagnosis was based on the presence of a large amount of monoclonal protein on serum electrophoresis and more than 10% bone marrow monoclonal plasma cells. She is asymptomatic. She takes no medications. Physical examination findings, including vital signs, are normal. Serum calcium level is 11.2 mg/dL (2.8 mmol/L), and total protein is 9.2 g/dL (92 g/L).
Which of the following should be measured?
A. 24-Hour urine calcium
B. 25-Hydroxyvitamin D
C. Ionized calcium
D. Parathyroid hormone
This patient's ionized calcium level (Option C) should be measured. Her total calcium level is elevated, but she is without symptoms of hypercalcemia.
Approximately 40% to 45% of the calcium in serum is bound to protein, principally albumin, although the physiologically active form of calcium is in an ionized (or free) state. In most patients with relatively normal serum albumin levels, the total calcium usually reflects an accurate ionized calcium fraction. However, in clinical settings in which increased protein binding of calcium may occur, the serum total calcium level may be elevated without a rise in the actual serum ionized calcium concentration. This may occur in patients with hyperalbuminuria (as may occur in those who are severely dehydrated) and in patients with a paraprotein capable of binding calcium (as occasionally occurs in some patients with multiple myeloma). This phenomenon is sometimes termed pseudohypercalcemia (or factitious hypercalcemia). If present, a normal ionized calcium level may indicate that the elevated total calcium level is the result of excessive protein binding and potentially eliminates the need for further evaluation for hypercalcemia. Ionized calcium measurement is indicated in asymptomatic patients with multiple myeloma and elevated total serum calcium.
A 24-hour urine calcium measurement (Option A) is indicated in the diagnosis of familial hypocalciuric hypercalcemia (FHH). FHH is an autosomal dominant condition and the most common type of familial hypercalcemia. In FHH, an inactivating mutation of the CaSR gene causes the parathyroid gland to perceive serum calcium concentrations as low, resulting in increased parathyroid hormone (PTH) secretion and a higher serum calcium level. Simultaneously, the mutated CaSR in the kidney increases kidney resorption of calcium, leading to paradoxical hypocalciuria in the setting of hypercalcemia. This patient with multiple myeloma and a large amount of serum monoclonal protein likely has pseudohypercalcemia, and measurement of the ionized calcium level is the most appropriate diagnostic test.
25-Hydroxyvitamin D (Option B) is the storage form of vitamin D in the body, and its measurement is the most appropriate test for assessing vitamin D stores but will not help evaluate patients with hypercalcemia. Measuring both 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D is useful in further assessing patients with non–PTH-mediated hypercalcemia to assess for excess vitamin D production.
PTH testing (Option D) is indicated in patients with hypercalcemia to differentiate between PTH-mediated and non–PTH-mediated hypercalcemia. Measurement of PTH and 1,25-dihydroxyvitamin D levels may be indicated as part of this patient's evaluation, but only after true hypercalcemia has been established by measuring the ionized calcium. However, the primary cause of hypercalcemia in patients with multiple myeloma is not primary hyperparathyroidism but rather tumor-induced, osteoclast-mediated bone resorption due to cytokines released by myeloma cells.
400
A 60-year-old woman is evaluated at follow-up for daily nausea, bloating and occasional vomiting after large meals, epigastric pain, and fullness. Upper endoscopy last week revealed some retained food in the stomach but no other significant findings, including Helicobacter pylori infection. She has a 10-year history of type 2 diabetes mellitus. Current medications are metformin and canagliflozin. The hemoglobin A1c level is 9%.
Which of the following is the most appropriate next step in management?
A. Initiate erythromycin
B. Initiate metoclopramide
C. Obtain 4-hour gastric scintigraphy
D. Obtain upper gastrointestinal barium series
E. Repeat upper endoscopy once hemoglobin A1c level is less than 7%
The most appropriate next step in management is 4-hour gastric scintigraphy (Option C).
This patient's presentation strongly suggests—but is not diagnostic of—diabetic gastroparesis. Her upper gastrointestinal symptoms and the retained food on upper endoscopy indicate delayed gastric emptying. However, definitive diagnosis of gastroparesis requires objectively demonstrating a delay in gastric emptying. American College of Gastroenterology guidelines state that the diagnosis of gastroparesis must be based on the combination of symptoms of gastroparesis, absence of gastric outlet obstruction or ulceration, and a delay in gastric emptying. Objective evidence of delayed gastric emptying is important because other conditions, such as accelerated gastric emptying, functional dyspepsia, Helicobacter pylori infection, and peptic ulcer disease, can present with similar symptoms. This patient reports many gastroparesis symptoms, which can include early satiety, postprandial fullness, nausea, vomiting, bloating, and/or upper abdominal pain. Her upper endoscopy excluded a mechanical obstruction of the stomach and H. pylori gastritis. To document a delay in gastric emptying, further testing must be performed. The three tests used are scintigraphy, wireless motility capsule, and breath testing using 13C-labeled Spirulina platensis. Of these tests, scintigraphy of a solid-phase meal is considered the standard for diagnosis of gastroparesis because it quantifies the emptying of a physiologic caloric meal. The 4-hour solid-emptying study is preferred over shorter solid-emptying studies or sole liquid-emptying studies because those methods are less sensitive. The most reliable parameter to document a delayed gastric emptying is the percentage of retained gastric contents 4 hours after meal consumption.
Medical therapy for gastroparesis—erythromycin (Option A) or metoclopramide (Option B)—should not be initiated until the diagnosis is confirmed.
An upper gastrointestinal barium series (Option D) can exclude mechanical obstruction and other structural abnormalities of the upper gastrointestinal tract, but this confirmation has already been accomplished with upper endoscopy. A barium series cannot objectively assess gastric emptying.
Although poor glycemic control is known to further delay gastric emptying, there is no value in repeating upper endoscopy after better control of this patient's diabetes (Option E) to reassess for retained food.
400
This NBA player recently scored 83 points setting the record as the second-highest-scoring game in NBA history.
Bam Adebayo
500
A 22-year-old woman is evaluated in the office for a 6-month history of intermittent nausea, anorexia, and occasional constipation. She does not smoke cigarettes, drink alcohol, or use recreational drugs. She otherwise feels well and takes no medications. Family history is unremarkable. Vital signs and physical examination are normal. Hypercalcemia was noted on an initial metabolic profile.
Repeat laboratory studies:
Calcium: 11.1 mg/dL (2.8 mmol/L)
Creatinine: 1.0 mg/dL (88.4 μmol/L)
Phosphorus: 4.4 mg/dL (1.4 mmol/L)
Parathyroid hormone: <10 pg/mL (<10 ng/L)
25-Hydroxyvitamin D: 36 ng/mL (89.9 mmol/L)
1,25-Dihydroxyvitamin D: 97 pg/mL (233.0 pmol/L)
24-Hour urine calcium: 450 mg/24 h
Which of the following is the most appropriate additional test?
A. Chest radiography
B. Neck ultrasonography
C. Parathyroid hormone-related protein measurement
D. Urine calcium-creatinine ratio determination
The most appropriate additional test is chest radiography (Option A).
This patient has mildly symptomatic hypercalcemia and a high-normal serum phosphorus level, suppressed parathyroid hormone (PTH), and an elevated 1,25-dihydroxyvitamin D level. Unregulated conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D may occur in granulomatous tissue associated with fungal infection, tuberculosis, sarcoidosis, and lymphoma, leading to increased intestinal absorption of calcium. Vitamin D-dependent hypercalcemia is associated with normal to elevated serum phosphorus levels because vitamin D enhances intestinal absorption of phosphorus, and suppressed PTH secretion reduces kidney phosphorus excretion. In the absence of an established cause of vitamin D-dependent hypercalcemia, such as documented ingestion, a chest radiograph to diagnose sarcoidosis, fungal infection, tuberculosis, or lymphoma is reasonable. In this young otherwise healthy patient, pulmonary sarcoidosis causing vitamin D-dependent hypercalcemia is probable.
Neck ultrasonography (Option B) may be reasonable to consider in a patient with PTH-dependent hypercalcemia to locate an adenoma before surgery. However, this patient's PTH is suppressed, making hyperparathyroidism unlikely.
Tumor-produced PTH-related protein (PTHrP) is the most common cause of hypercalcemia of malignancy. As in this patient, PTH would be suppressed but 1,25-dihydroxyvitamin D would not be elevated and serum phosphorus would be low. Most patients with humoral hypercalcemia of malignancy have advanced cancer associated with severe hypercalcemia; tumor-produced PTHrP is an unlikely mechanism of hypercalcemia in this otherwise well young patient. Therefore, PTHrP measurement is inappropriate for this patient (Option C).
Urine calcium-creatinine ratio determination (Option D) is useful to confirm the diagnosis of familial hypocalciuric hypercalcemia (FHH). Patients with this disorder are asymptomatic, have a history of hypercalcemia since childhood, and a family history of hypercalcemia. In this condition, the PTH level is elevated and the urine calcium excretion is low, resulting in paradoxical hypocalciuria in the setting of hypercalcemia. This patient's clinical and biochemical profiles are inconsistent with FHH, so measurement of the urine calcium-creatinine ratio is unnecessary.
500
A 22-year-old man is hospitalized with a 3-day history of nonproductive cough, fever, and diarrhea. He returned 1 week ago from a tournament in Indiana with his college wrestling team. During this trip, the team used an indoor hot tub. Three other team members have developed a flu-like illness. Medical history is noncontributory, and he takes no medications. On physical examination, temperature is 38.8 °C (101.8 °F), blood pressure is 115/75 mm Hg, pulse rate is 68/min, and respiration rate is 24/min. The examination is unremarkable.
Laboratory studies show a serum sodium level of 128 mEq/L (128 mmol/L).
COVID-19 testing and Legionella urinary antigen are negative.
A chest radiograph is shown.

The patient improves within 48 hours of initiating empiric therapy with ceftriaxone and azithromycin.
Which of the following is the most likely diagnosis?
A. Herpes simplex virus type 1 pneumonia
B. Histoplasma pneumonia
C. Legionella pneumonia
D. Mycobacterium avium complex lung infection
E. Pseudomonas pneumonia
Despite the negative Legionella urine antigen test, the most likely diagnosis in this patient is Legionella pneumonia (Option C).
Legionella causes 2% to 15% of community-acquired pneumonia (CAP) illnesses but is likely under-recognized. Several clinical and epidemiologic clues suggest a Legionella pneumonia diagnosis in this patient. Most important is the clustering of infections among cotravelers exposed to a common water source. Legionella has been associated with inhalation of infectious aerosols from water sources, including air conditioning cooling units, spas, pools, fountains, and showers. Features that are variably present but may suggest Legionella include gastrointestinal symptoms (including diarrhea), altered mentation, pulse-temperature dissociation, increased liver enzymes, and hyponatremia. The 2019 Infectious Diseases Society of America and American Thoracic Society guidelines recommend conditional testing for Legionella urinary antigen when suggestive epidemiologic features are present, such as an outbreak, or in cases of severe pneumonia. This test only detects L. pneumophila serogroup 1, which accounts for between 70% and 90% of laboratory diagnosed CAP in the United States; other species or serogroups would be missed through urinary antigen testing but may be identified by culture of respiratory specimens on selective media.
Wrestlers are at risk for herpes gladiatorum, a cutaneous infection with herpes simplex virus type 1, but not herpes simplex pneumonia, which typically occurs in severely immunocompromised patients (Option A).
Histoplasmosis is an important endemic mycosis in Indiana and the Ohio and Mississippi River Valleys but causes a more indolent pulmonary infection and would not improve with standard treatment for CAP (Option B).
Pseudomonas and Mycobacterium avium complex (MAC) are associated with respiratory infection and granulomatous lung disease (“hot tub lung”), respectively, following hot tub exposure in an enclosed area (Option D, E). Neither of these pathogens is likely, given the clinical course. Pseudomonas would not improve without effective antibiotic therapy, and hot tub–associated pneumonia is very rare. MAC-related disease, thought to be a hypersensitivity reaction rather than true infection, usually occurs following prolonged hot tub exposure and is more indolent in presentation.
500
A 65-year-old man is evaluated for a 7-week history of increasing fatigue and poor appetite. Medical history is otherwise unremarkable. He takes no medications. Physical examination findings, including vital signs, are normal.
Laboratory studies:
Hematocrit: 28%
Albumin: 3.0 g/dL (30 g/L)
Calcium: 10.4 mg/dL (2.6 mmol/L)
Creatinine: 1.6 mg/dL (141.4 µmol/L)
Sodium: 130 mEq/L (130 mmol/L)
Potassium: 3.6 mEq/L (3.6 mmol/L)
Chloride: 99 mEq/L (99 mmol/L)
Bicarbonate: 23 mEq/L (23 mmol/L)
Osmolality: 290 mOsm/kg H2O
Total protein: 9.8 g/dL (98 g/L)
Urine osmolality: 240 mOsm/kg H2O
Urine sodium: 45 mEq/L (45 mmol/L)
Which of the following is the most likely cause of this patient's hyponatremia?
A. Hypercalcemia
B. Multiple myeloma
C. Poor solute intake
D. Psychogenic polydipsia
E. Syndrome of inappropriate antidiuretic hormone secretion
The most likely cause of this patient's hyponatremia is multiple myeloma (Option B).
Results of this patient's laboratory studies, including elevated serum calcium, anemia, and elevated total protein and low albumin suggesting an increased gamma globulin fraction, support the diagnosis of multiple myeloma. The key finding, however, is that the patient has a normal measured serum osmolality in the context of hyponatremia. When evaluating a patient with hyponatremia, the first step is to measure serum osmolality. In this patient, the serum osmolality is normal, and thus he has isotonic hyponatremia. Isotonic hyponatremia (serum osmolality, 275-295 mOsm/kg H2O) is a laboratory artifact caused by the method by which serum sodium is measured. Plasma is divided into a water phase (93%), in which the sodium is dissolved, and a solid phase (7%), which consists of lipids and proteins. If the solid phase is increased by an increase in proteins, such as those found in multiple myeloma or severe elevations in serum triglycerides, there is a decrease in the water phase (i.e., from 93% to 80%). Most laboratories use a diluting electrode in which there is a tenfold dilution of the specimen when measuring electrolytes. With a decrease in the aqueous phase, the dilution is no longer 1:10, but even greater, resulting in a spurious value for sodium.
Hypercalcemia (Option A) can cause polyuria secondary to arginine vasopressin resistance, which would increase the sodium concentration, not lower it, as seen in this patient.
Because the kidney requires solute to excrete water, a decrease in solute intake (Option C), which occurs in potomania (excessive beer drinking) or in individuals with starvation, the kidney's ability to excrete water is reduced and can result in hyponatremia without excessive water intake. In these cases, urine osmolality would be <100 mOsm/kg H2O.
In psychogenic polydipsia (Option D), excess water intake exceeds the kidney's ability to excrete water through the urine, and urine osmolality would likely be <100 mOsm/kg H2O.
In the syndrome of inappropriate antidiuretic hormone (SIADH) secretion (Option E), the measured serum osmolality is always low, unlike that seen in this patient. Furthermore, patients with SIADH have hypo-osmolar hyponatremia.
500
A 41-year-old man has a 9-month history of nausea, vomiting, early satiety, and postprandial bloating. His only other medical problem is chronic shoulder pain, for which he takes daily ibuprofen.
Vital signs are normal. The abdomen is distended, with epigastric tenderness without guarding or rigidity. A succussion splash is heard.
Which of the following is the most appropriate management?
A. Gastric scintigraphy
B. Lansoprazole
C. Metoclopramide
D. Upper endoscopy
The most appropriate management is to perform upper endoscopy (Option D).
This patient has symptoms suggestive of delayed gastric emptying, which is characterized by nausea, vomiting, early satiety, bloating, postprandial fullness, and abdominal pain. A loud succussion splash is associated with retained air and gastric fluid. It is auscultated with the stethoscope over the upper abdomen when the patient is rocked or the abdomen is palpated. Delayed gastric emptying can be due to either a mechanical gastric outlet obstruction or gastroparesis. Gastroparesis is a neuromuscular disorder of the gastrointestinal tract. It is most commonly idiopathic, but other common causes are diabetes, drugs, and surgery. In this patient, the use of ibuprofen could have caused peptic ulceration with outlet obstruction due to inflammation and/or scarring. In all patients, the initial diagnostic test is upper endoscopy to exclude gastric outlet obstruction. Once a structural cause for symptoms has been excluded, a test to assess gastric emptying (such as gastric scintigraphy, wireless motility capsule, or radiolabeled carbon breath test) is performed. Gastric scintigraphy is used most commonly. Once delayed emptying is confirmed, additional testing may be required to determine the underlying cause of the gastroparesis.
Only after mechanical obstruction is ruled out would gastric scintigraphy (Option A) be a reasonable test to evaluate for gastroparesis. If scintigraphy is pursued, the 4-hour study is preferred over 90- or 120-minute studies due to increased diagnostic accuracy.
A proton pump inhibitor, such as lansoprazole (Option B), might be used in this patient if a pyloric ulcer is diagnosed as the cause of mechanical outlet obstruction, but its use would be premature until a diagnosis is established.
Treatment of gastroparesis focuses on prokinetic drugs, such as metoclopramide (Option C), and avoidance of medications that impair gastric motility, such as opioids and anticholinergics. Pyloric botulinum toxin injections, pyloroplasty, and gastric electrical stimulation have been used as well. Treatment with any of these modalities would be premature until a diagnosis is established.
500
At the start of 2026, the Venezuelan leader Nicolas Maduro was captured overnight in a U.S. military extraction. What was the Venezuelan president wearing (company or line of clothing will be accepted) which led to his photo going viral on social media?
Grey Nike Tech Fleece jacket and sweatpants