Hypercoagulable Havoc
and prevention
and prevention
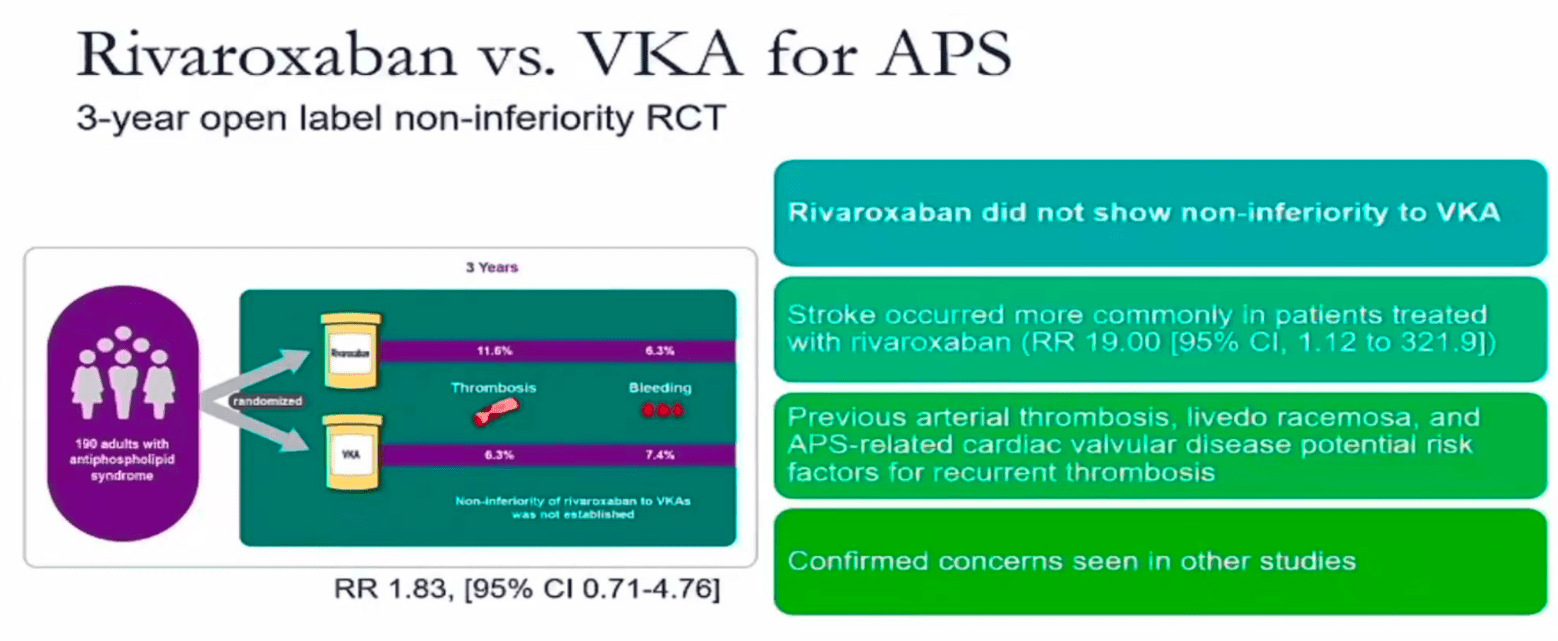
Should DOACs be used for APS?
no, some hematologist do but no - they did not show non inferiority
in some patients with only a venous thrombosis and low risk profile it might be okay - but at this point no evidence to support it. so still no.
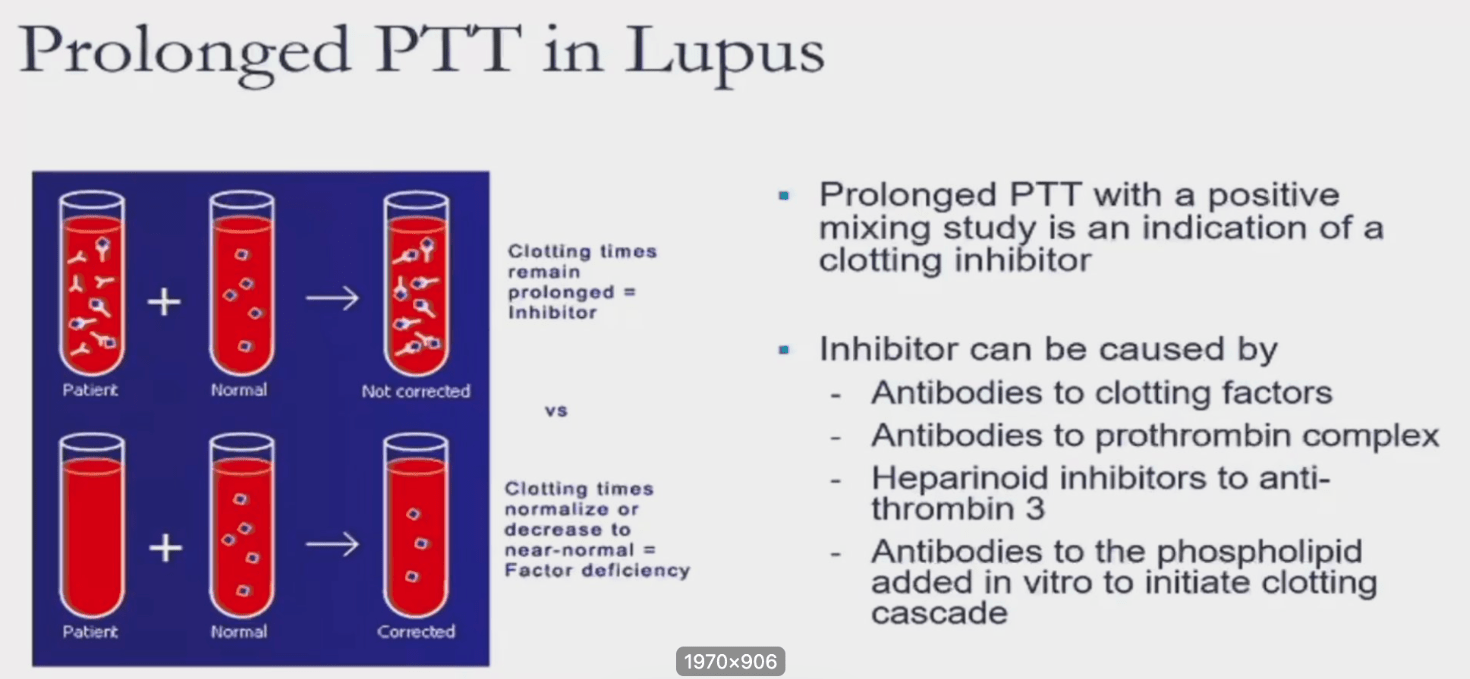
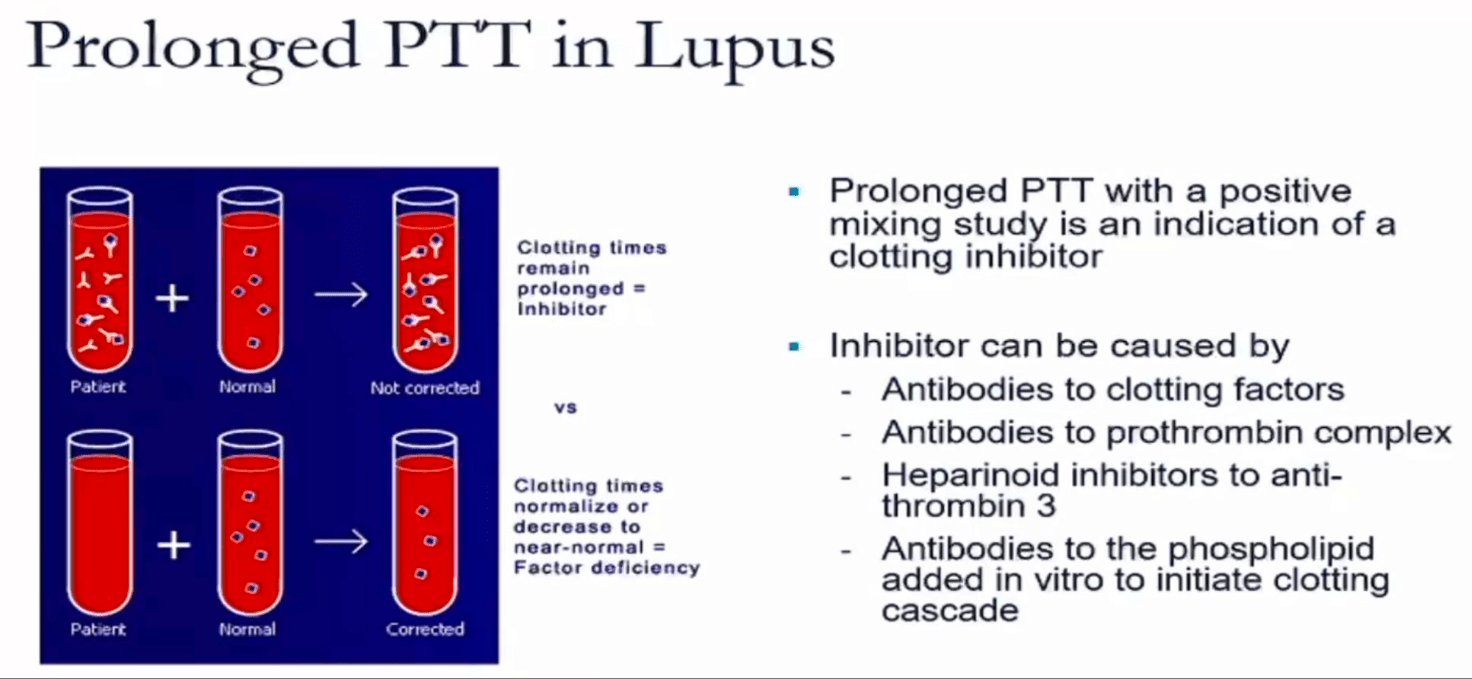
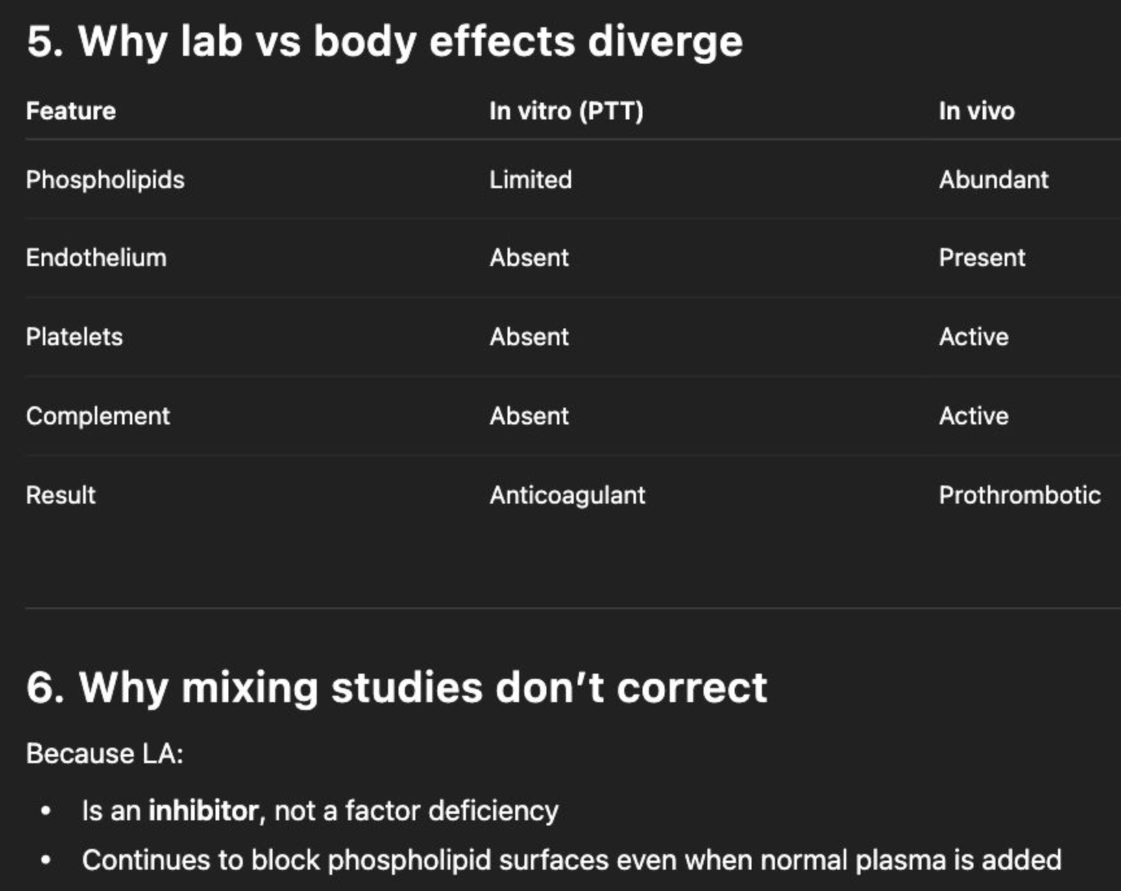
what is a positive mixing study?
means it is positive for an inhibitor. It does not normalize after mixing with normal plasma because there is an inhibitor (not a factor deficiency)
what skin finding gives points for APS classification criteria
- Livedo racemosa
- Livedoid vasculopathy lesion
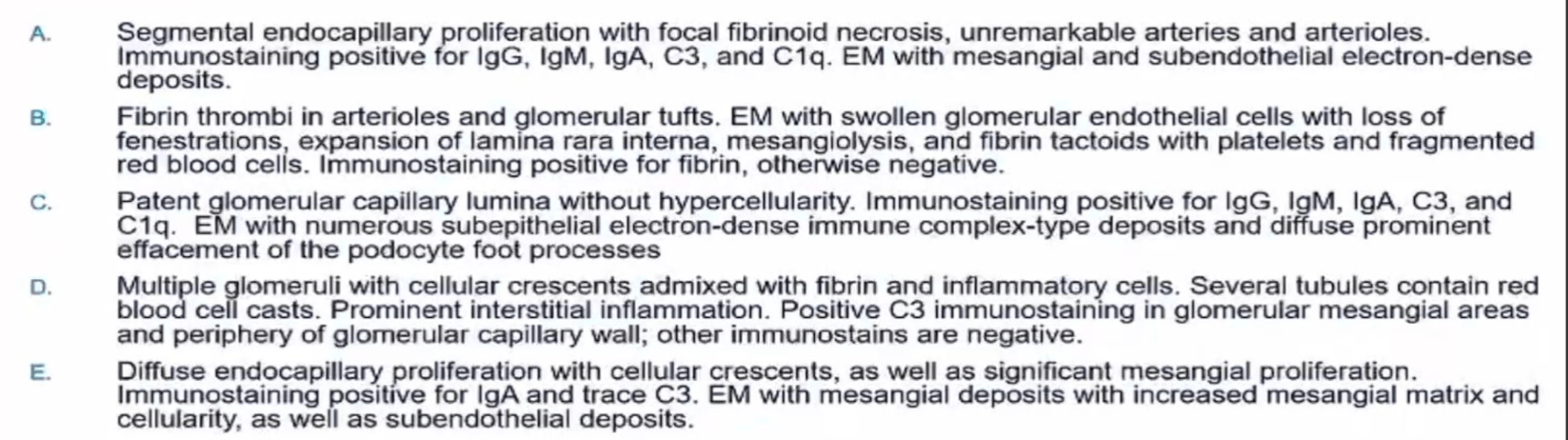
Patient with CAPS with aki and renal biopsy, what will biopsy show?

what is a negative mixing study?
means it is negative for an inhibitor. It does normalized after mixing with normal plasma because there is a factor deficiency (not an inhibitor)
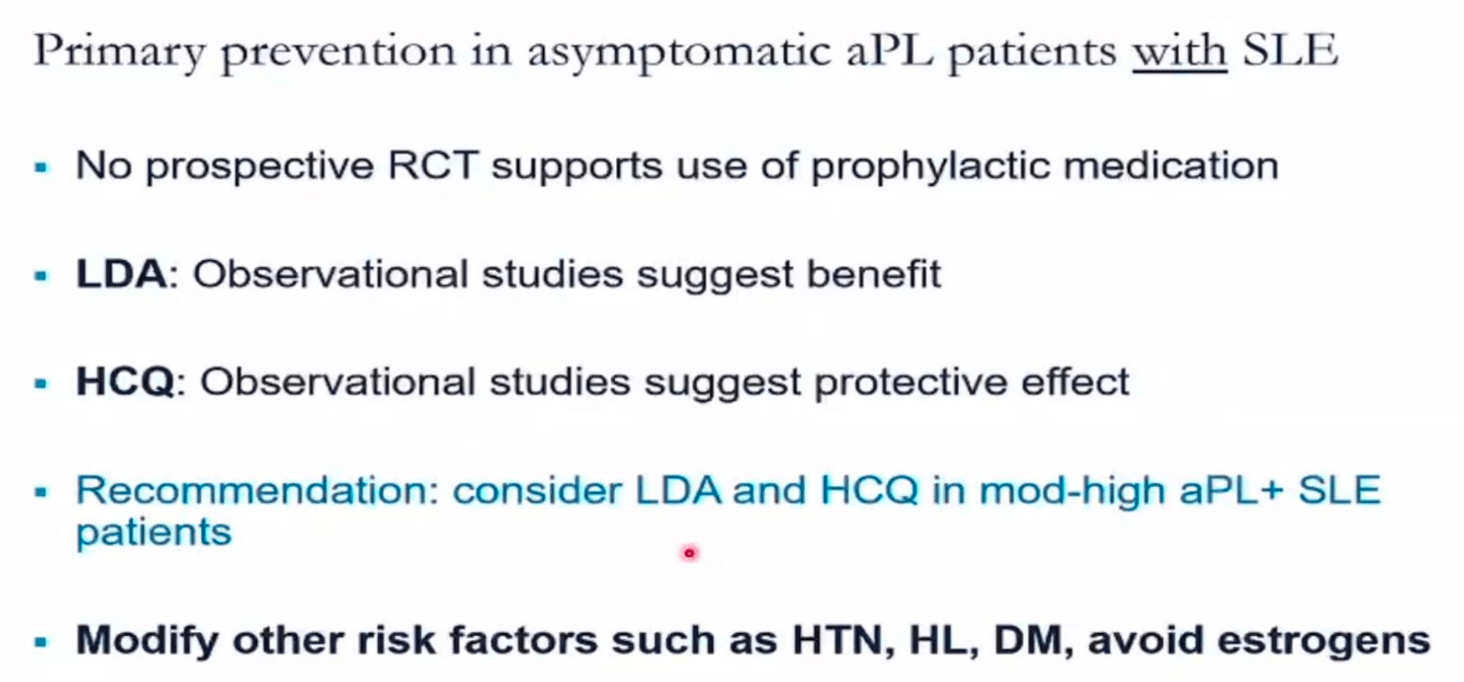
Should you prophylax asymptomatic aPL patients who have SLE?
obviously HCQ as they have SLE and may benefit APS. LDA too if moderate risk serology.
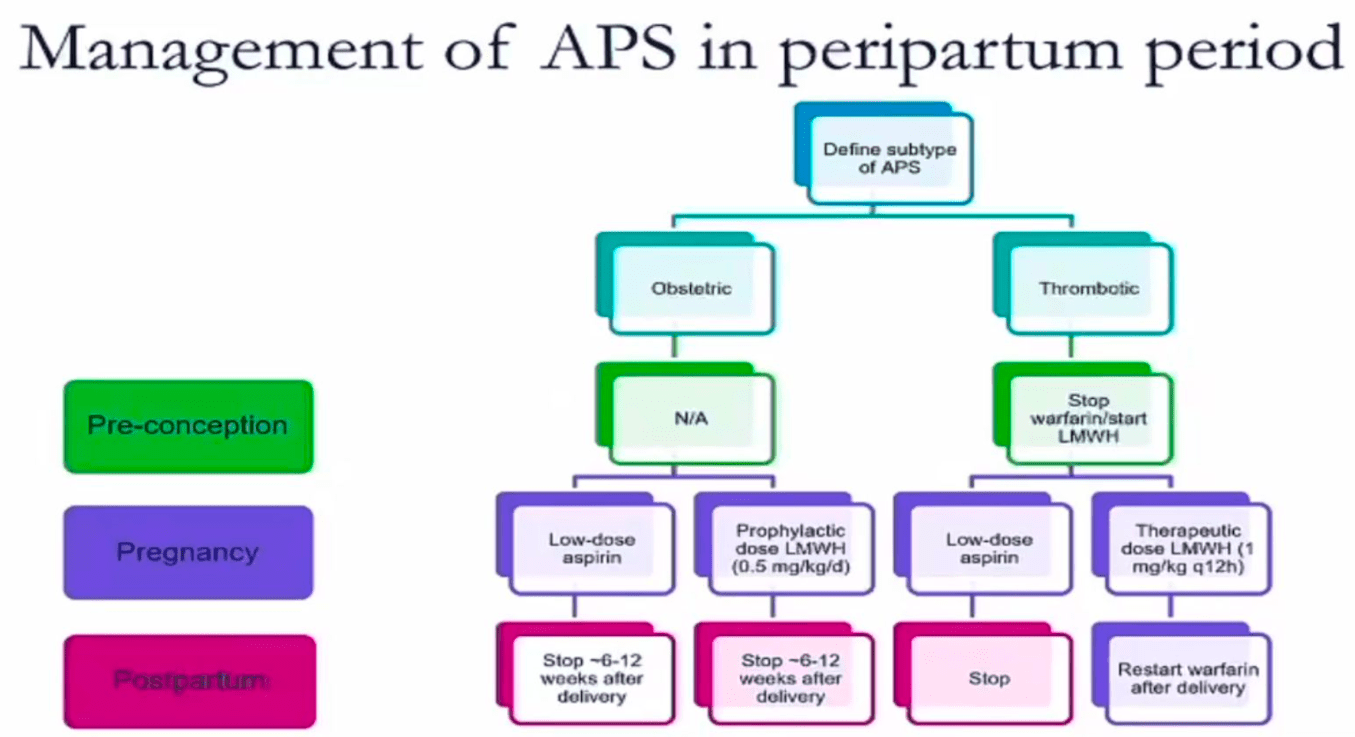
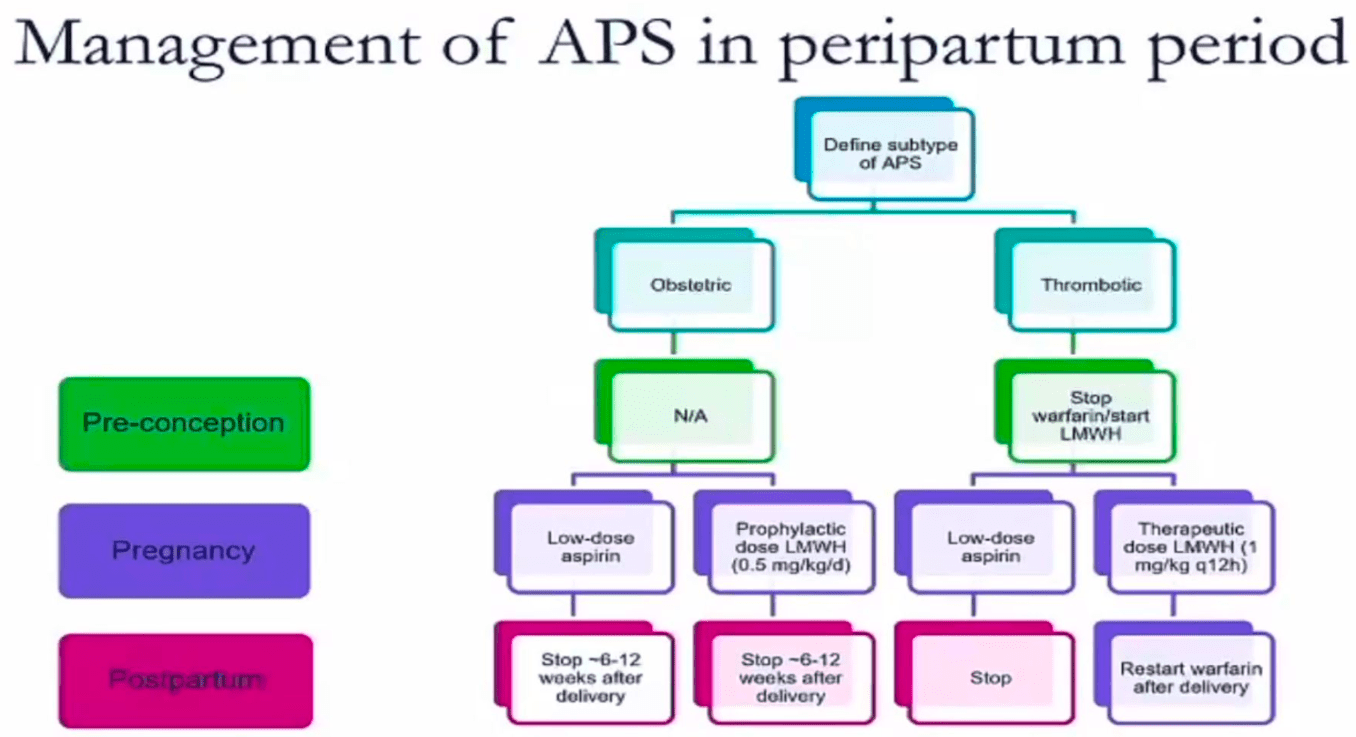
when should you stop treatment for obstetric APS?
6-12 weeks post partum stop the low dose aspiran and prophylactic dose LMWH (0.5mg/kg/d)
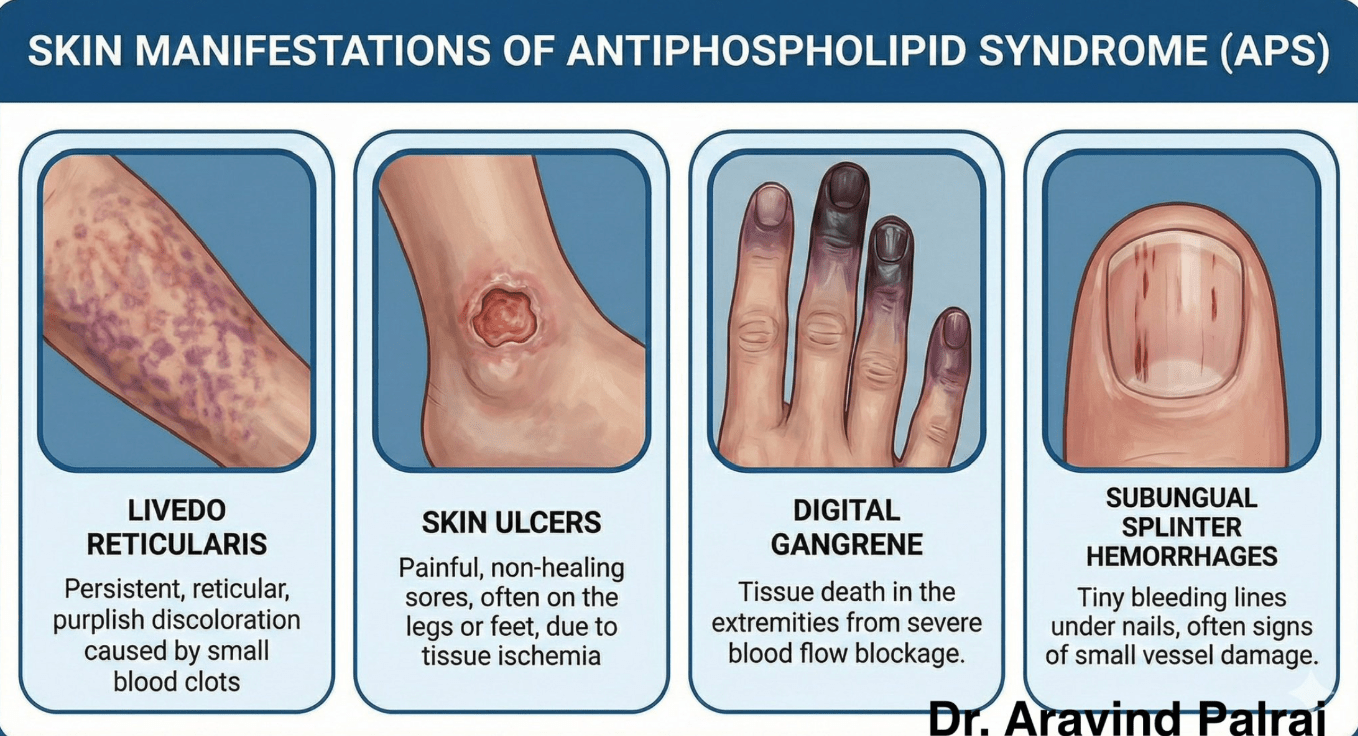
name 4 skin manifestations of APS
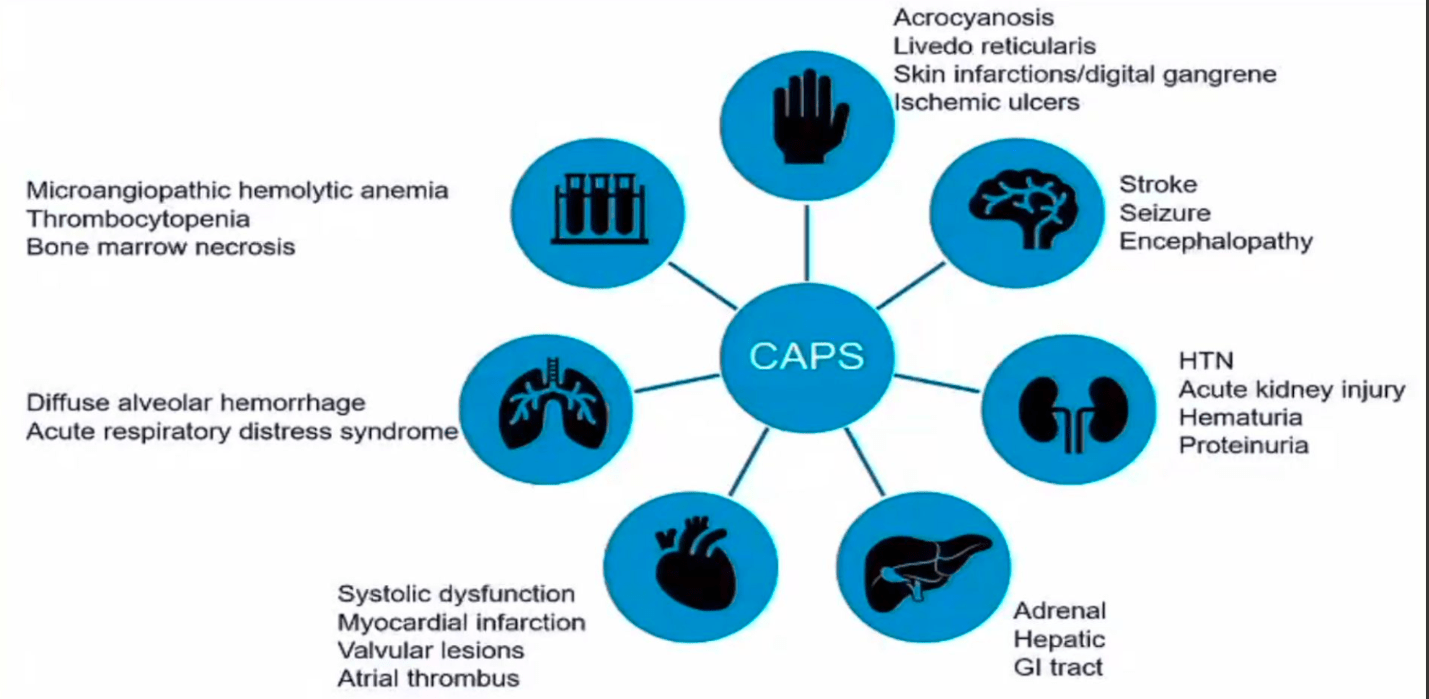
Acrocyanosis is a harmless condition causing a bluish tint to the hands, feet, or face due to narrowed small blood vessels restricting blood flow

Acrocyanosis is a harmless condition causing a bluish tint to the hands, feet, or face due to narrowed small blood vessels restricting blood flow

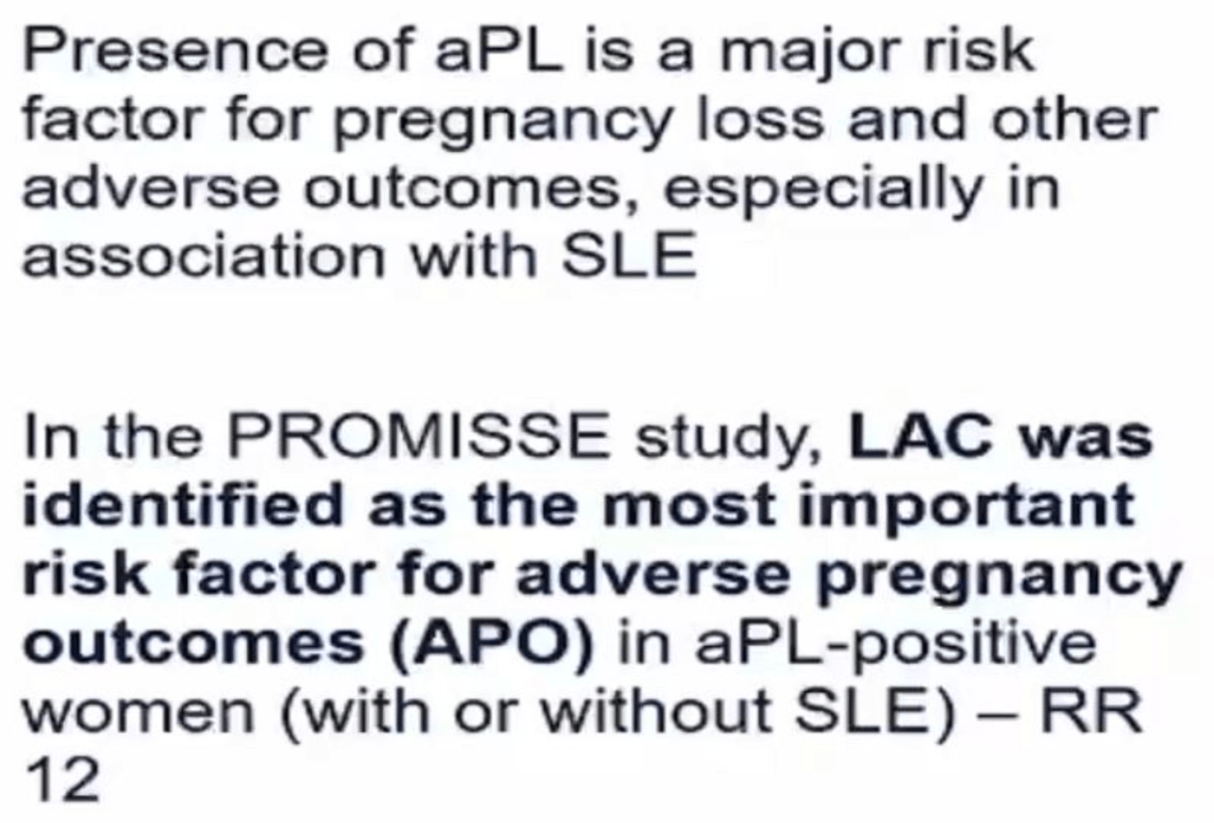
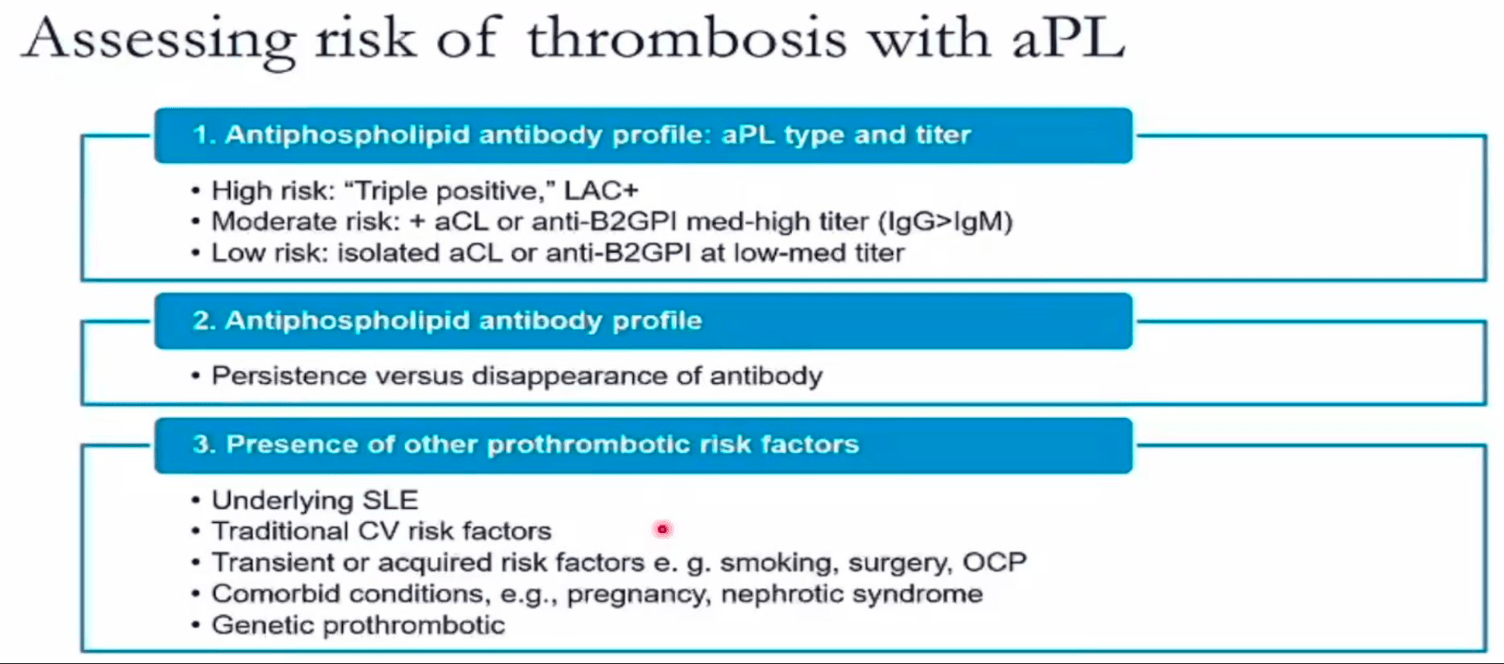
What is the most important risk factor for adverse pregnancy outcomes
LAC, RR 12
What effect does lupus anticoagulant have on PT and PTT
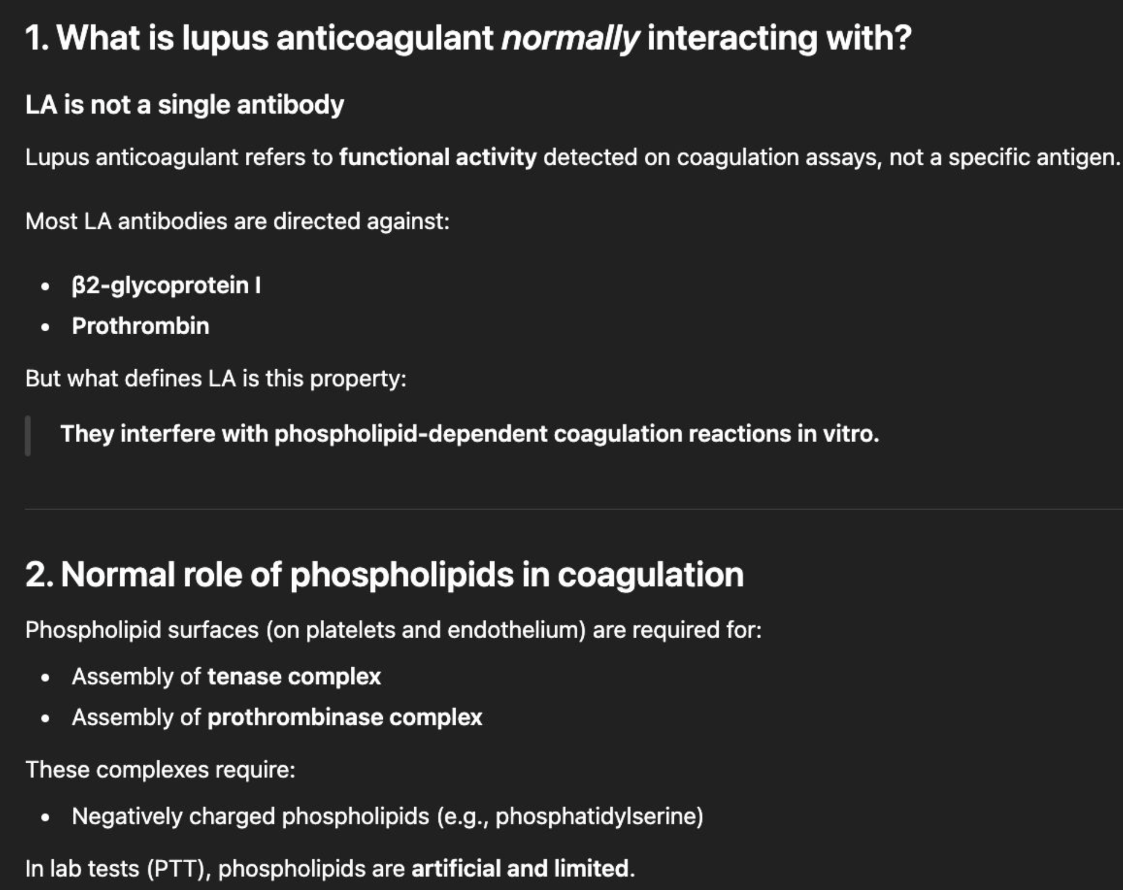
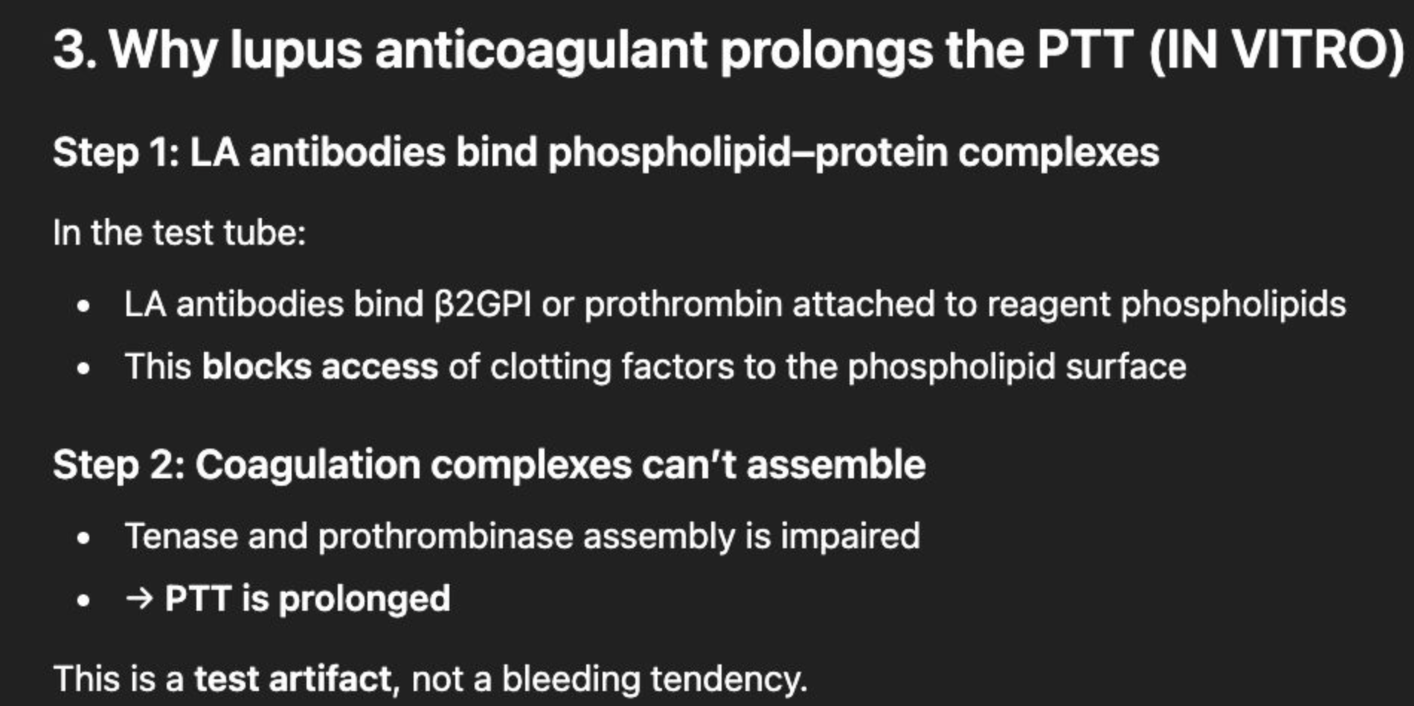
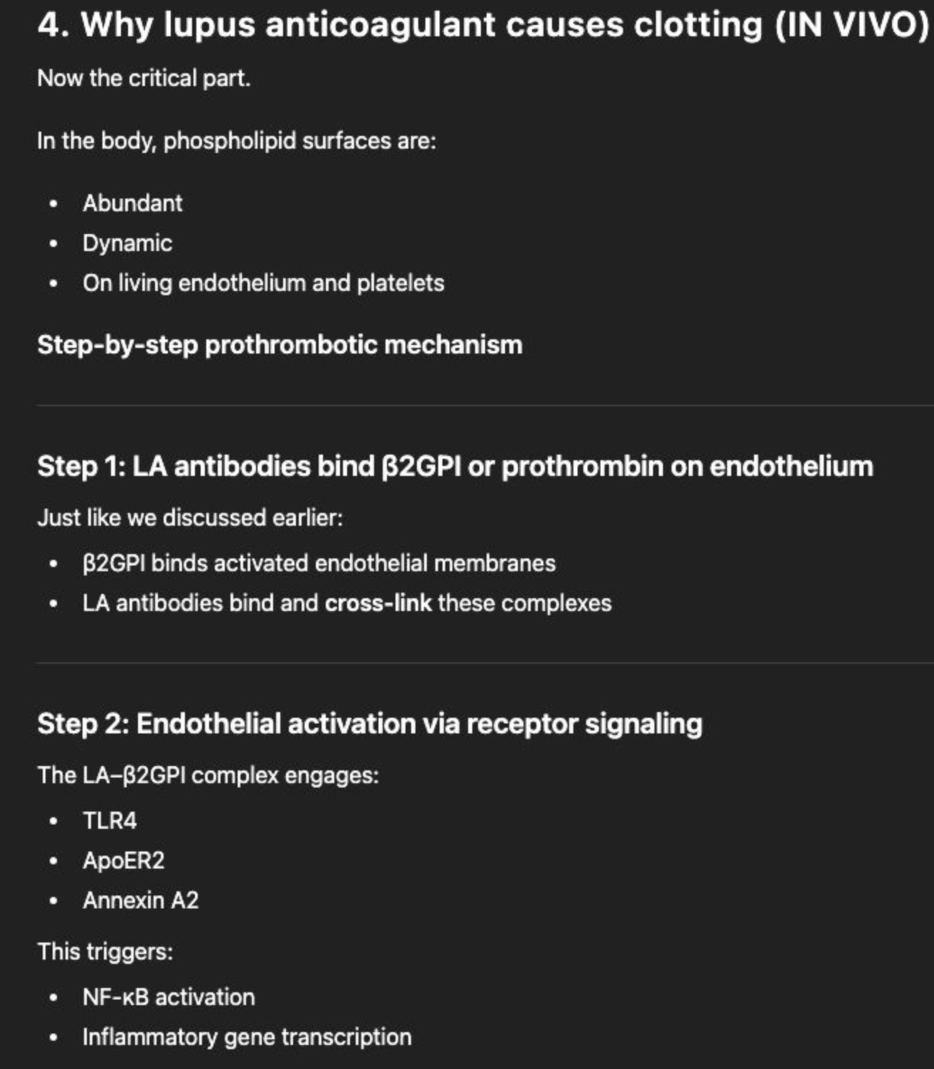
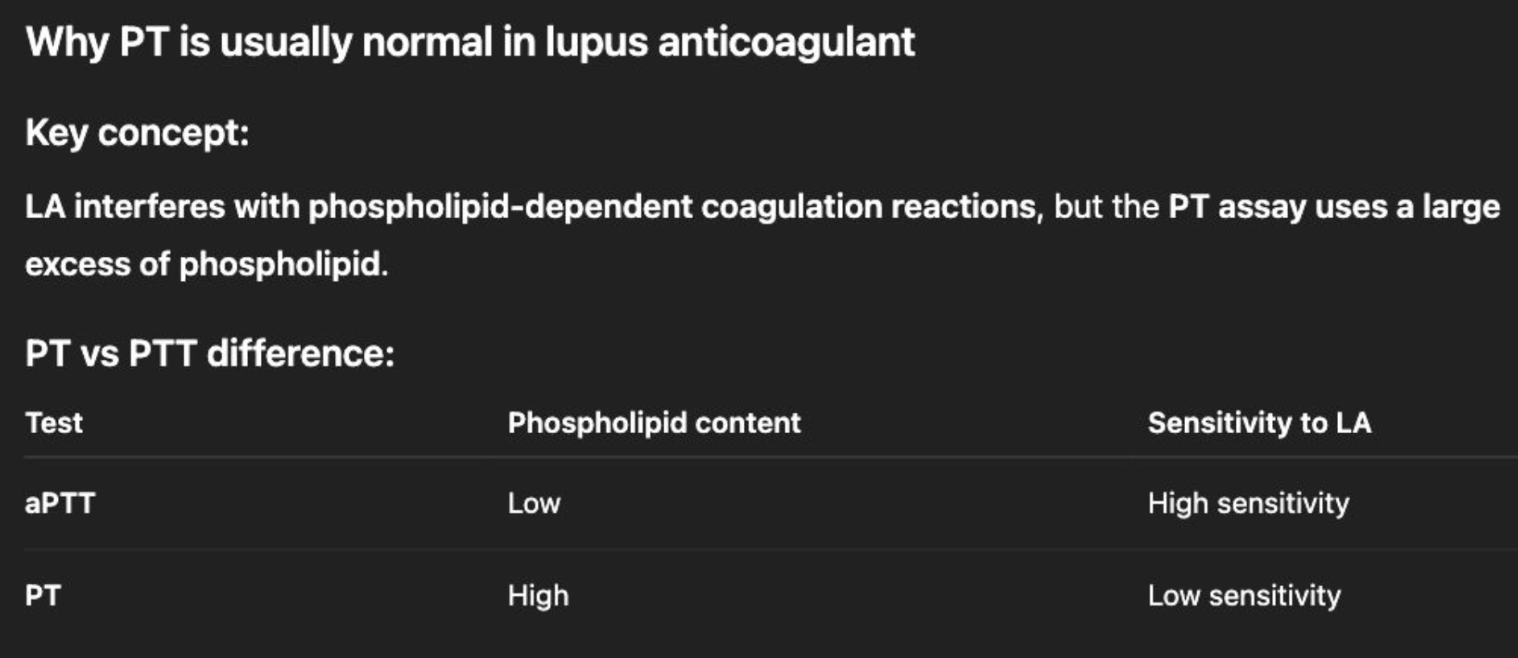
Because PT reagents contain excess phospholipid, they “overcome” the inhibitory effect of LA antibodies.
👉 Result: PT is usually normal, while aPTT is prolonged.
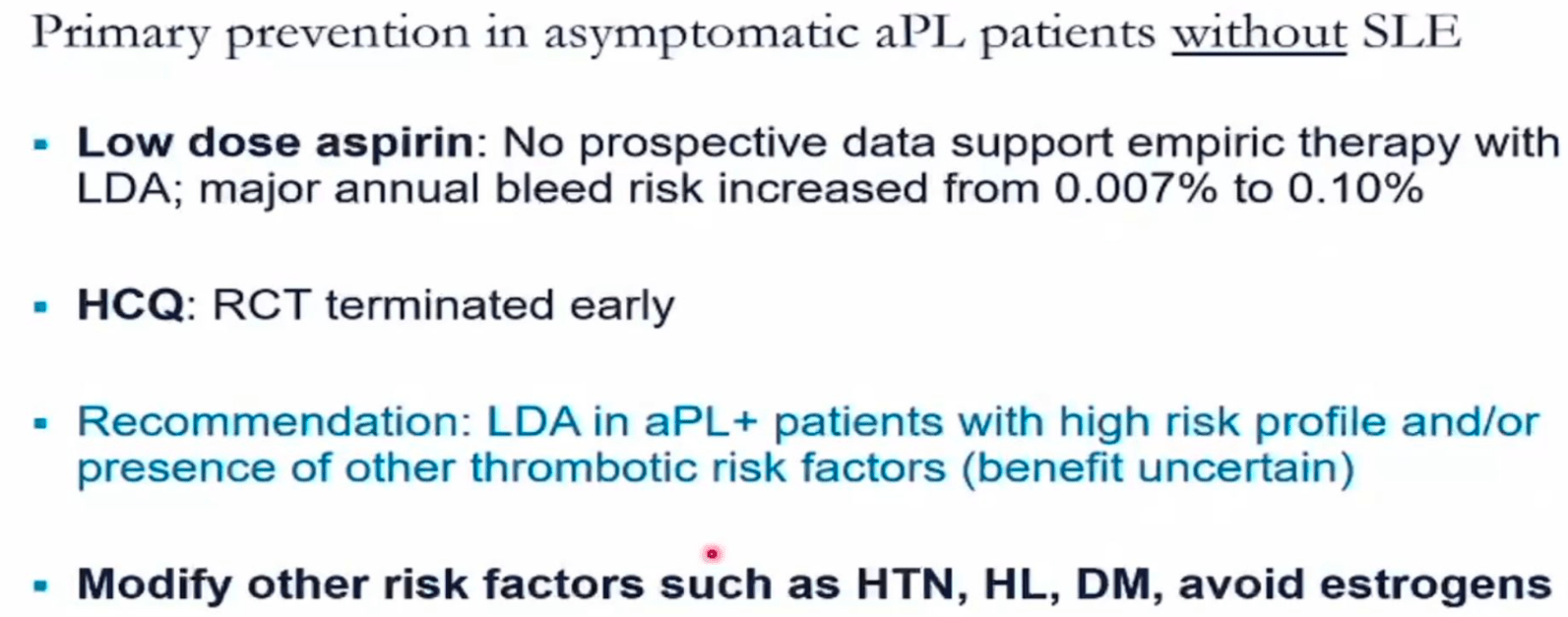
What primary prevention should be used in asymptomatic aPL patients without SLE
Most cases: nothing.
LDA only if high risk (meaning tripple + for persistent LAC+) profile and or presence of other risk factors
Patient with APS (dx by DVT) on warfarin becomes pregnant. How should you treat them pre-conception, during pregancy and during postpartum period?
THERAPEUTIC LMWH (1mg/kg q12hr) pre-conception (stop warfarin), aspirin and THERAPEUTIC LMWH (1mg/kg q12hr) during pregnancy. post partum stop aspirin (no need to continue for 6-12 weeks like you do in obstetric APS) and restart warfarin.
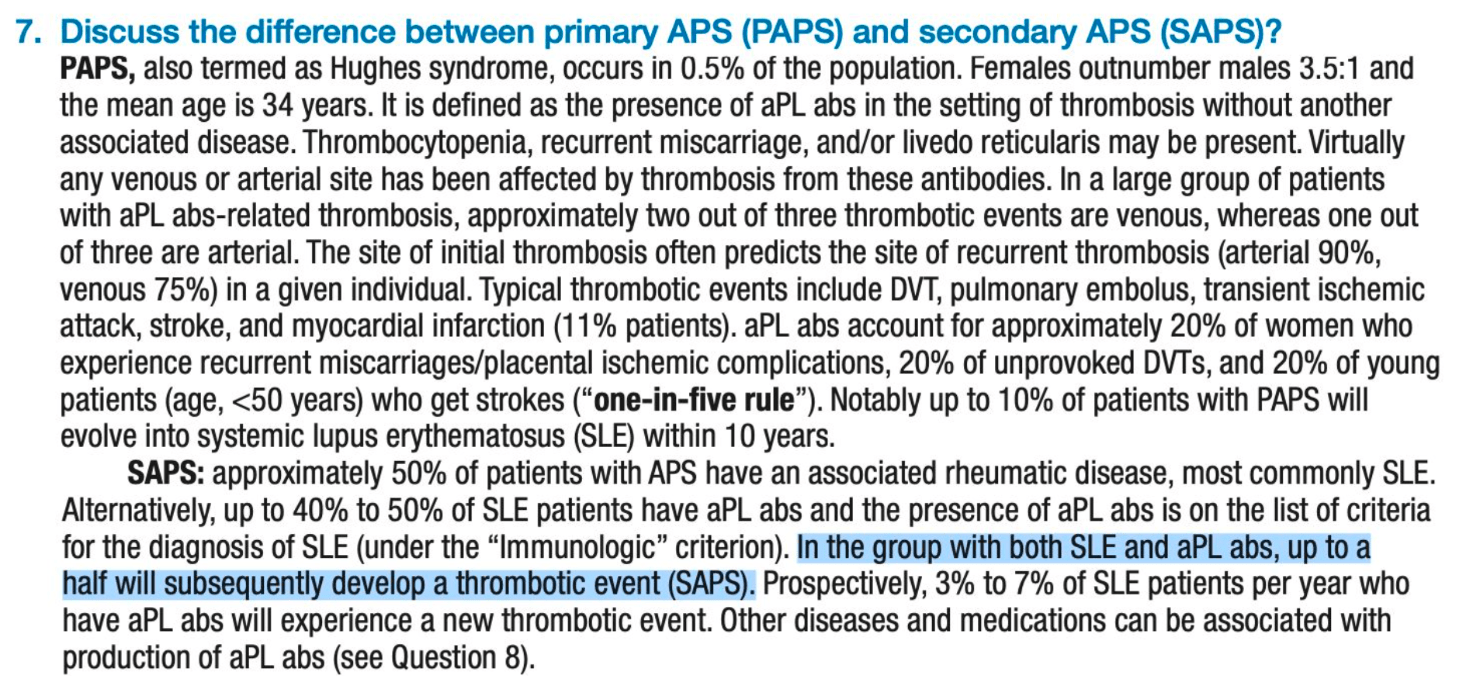
What percentage of patients with SLE and aPL abs will develop Secondary APS?
10%
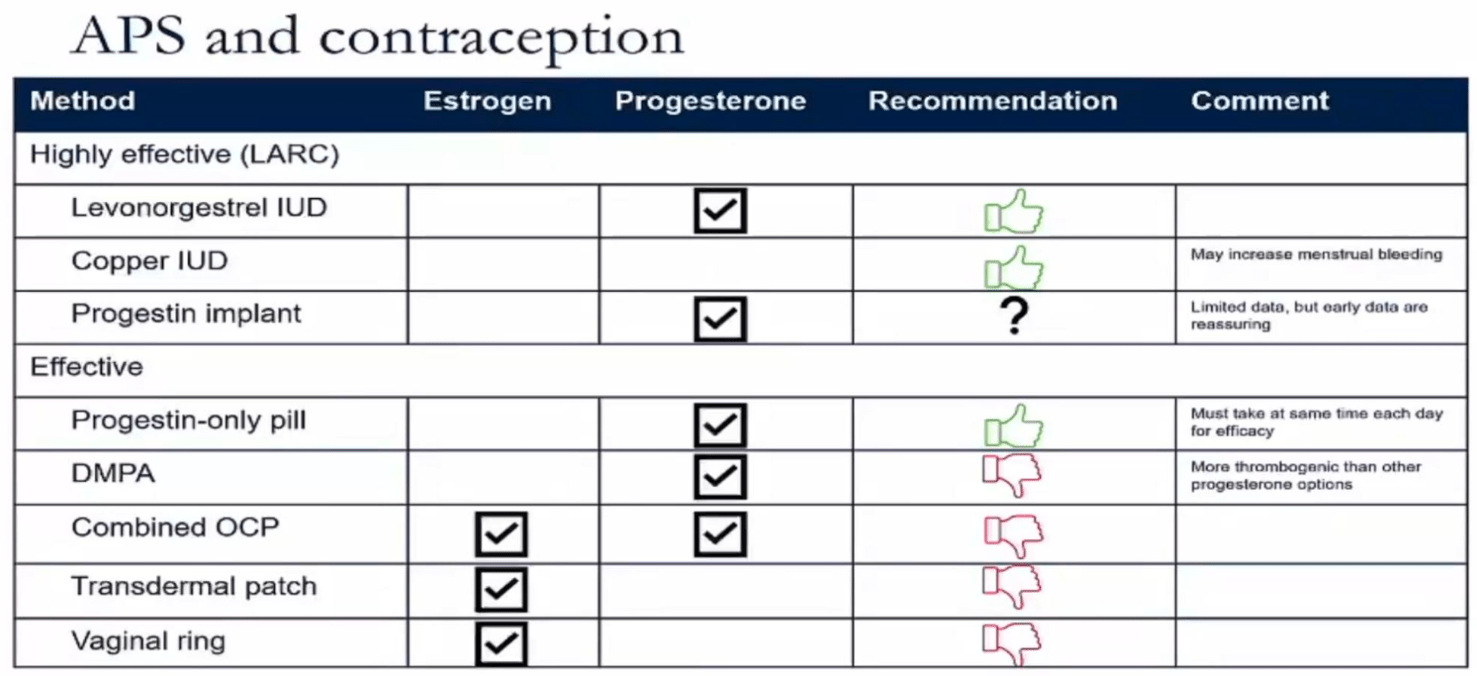
If a patient has an aPL antibody, which form on contraception should they get? What if theres no hx of a clot?
if aPL Ab +, they are contraindicated from getting estrogen containing contraceptives
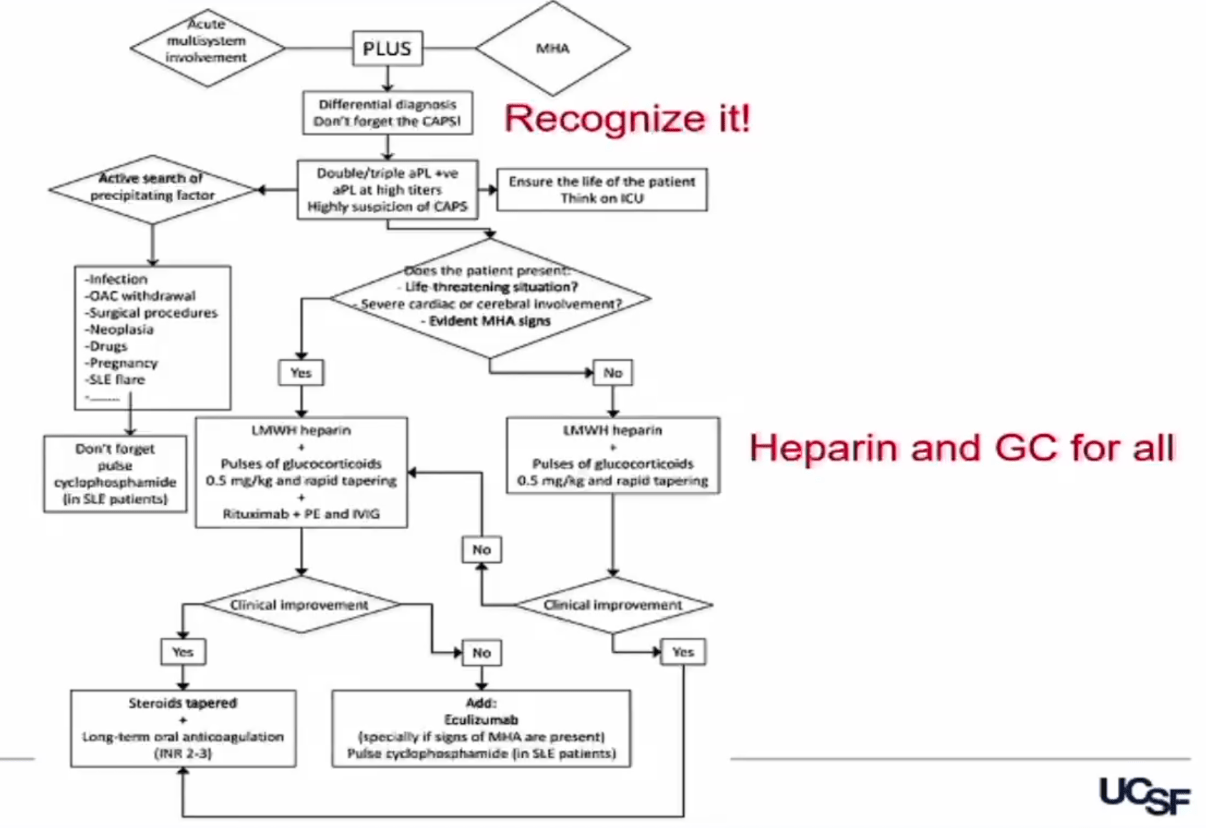
Name two drugs involved in treating all cases of CAPS
Treatment varies a lot. GC and heparin for all.
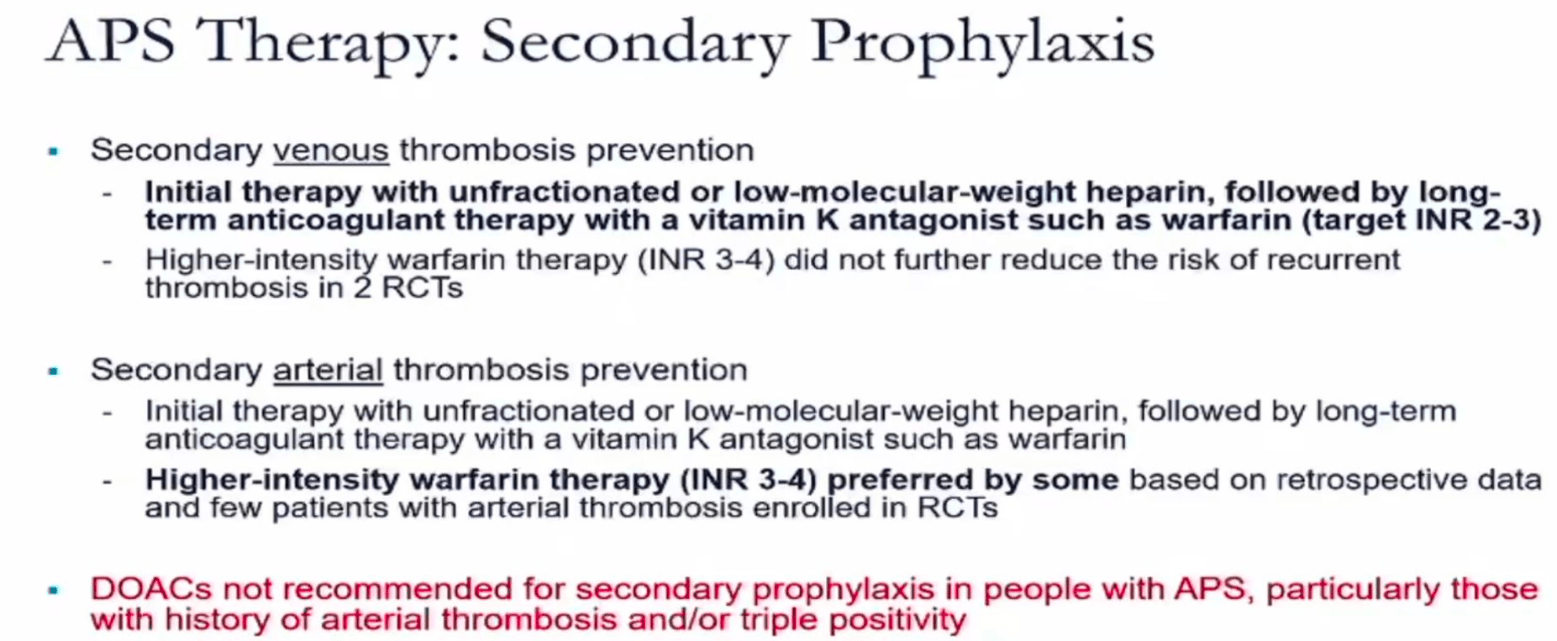
For secondary ppx in APS what med and target should be used
use warfarin,if arterial thrombosis the hematologist may go for INR of 3-4 instead of standard 2-3. but 2-3 is fine for most patients
Patient with obstetric APS is undergoing IVF. What should you treat with while undergoing IVF? (not yet pregnant)
Aspirin is for pre-eclampsia and other pregnancy complications, so not a risk if your not pregnant.
We are worried about risk of thrombosis while undergoing IVF so use prophylactic dose LMWH
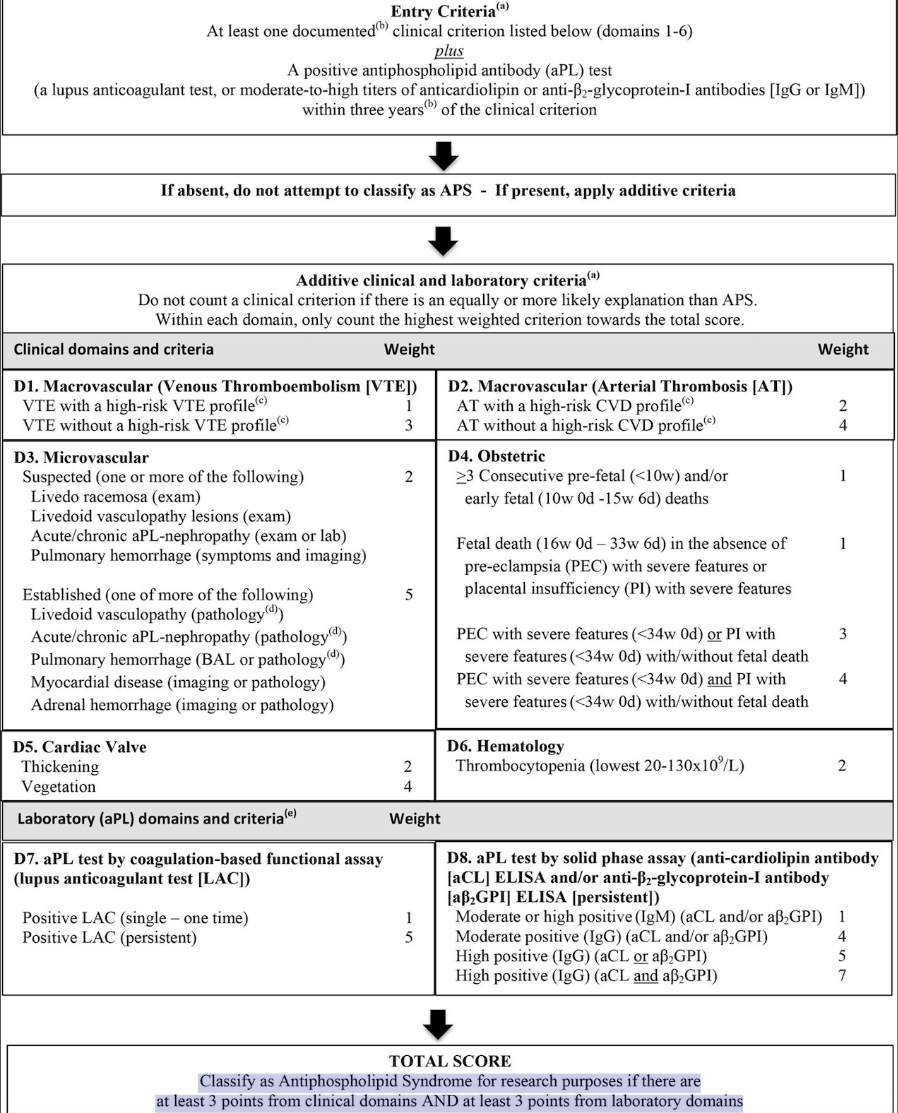
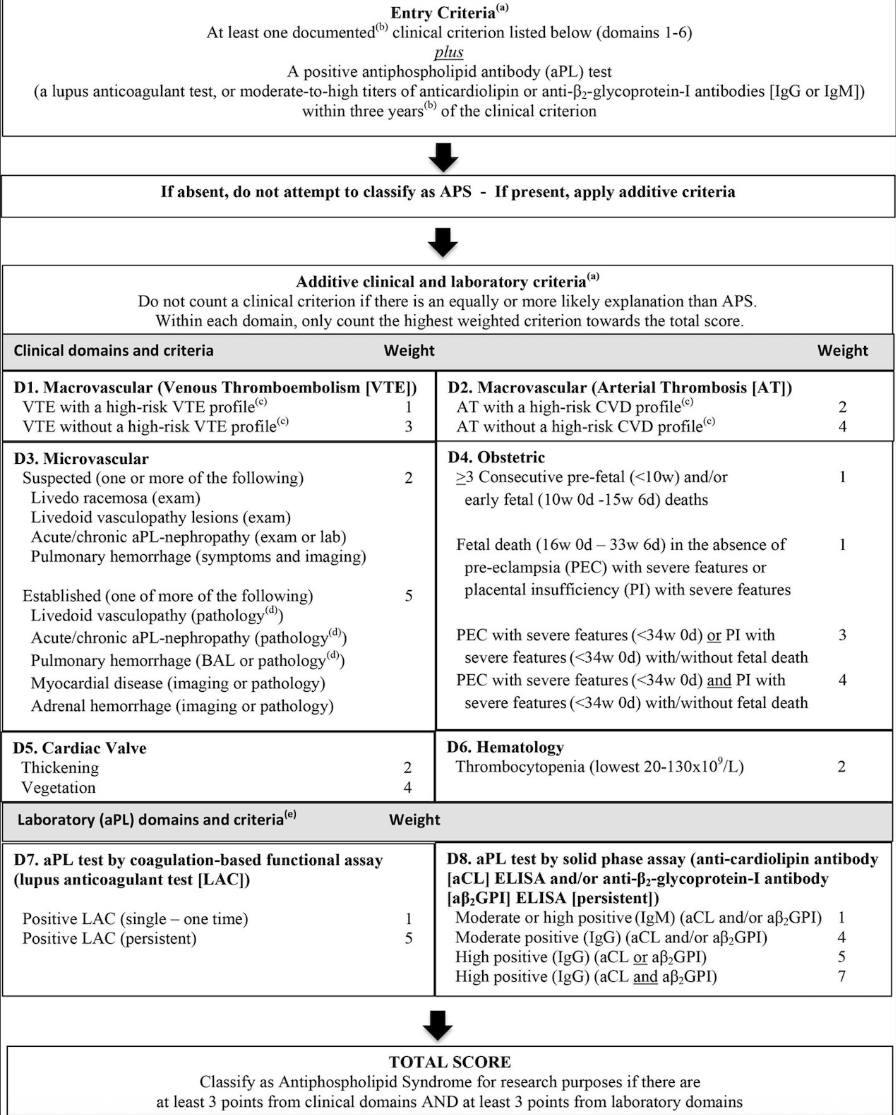
Classification criteria for APS
You classify as Antiphospholipid Syndrome if there are at least _ points from clinical domains AND at least _ points from laboratory domains
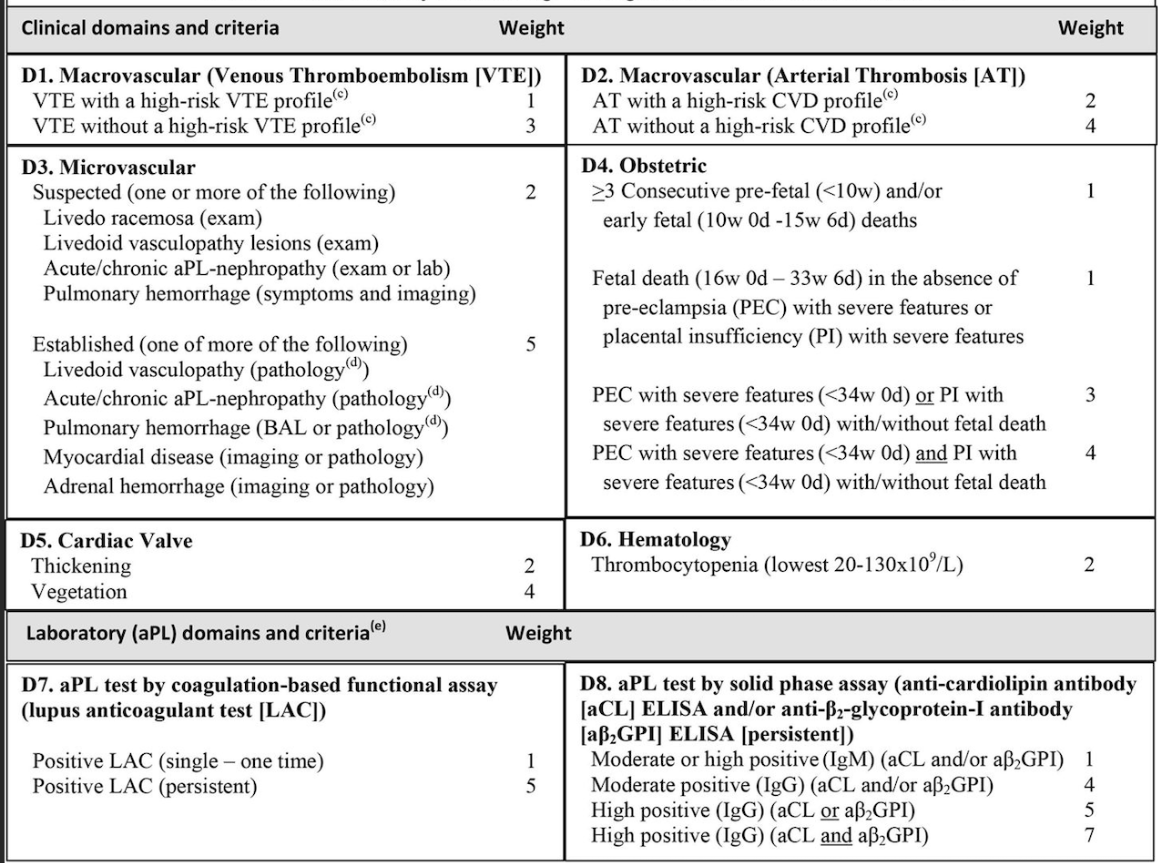
3, 3
What types of thrombosis should lead you to suspect APS
Arterial thrombosis especially before age of 50
Unprovoked DVT (before age of 50)
Recurrent thrombosis
Both arterial and venous thombosis events
Thrombosis at unusual sites
Obstetrical, fetal loss or recurrent miscarriages - source: secrets 2019
- source: secrets 2019
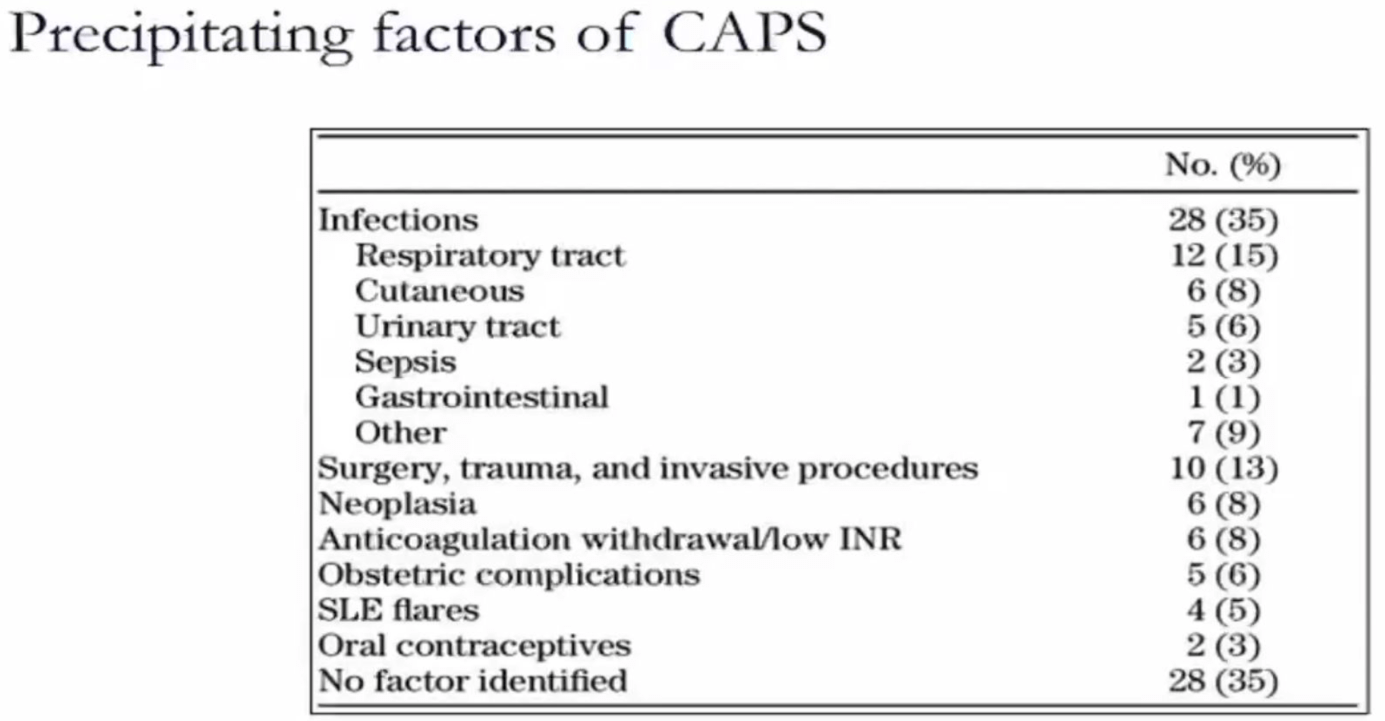
what are the two most common precipitating factors of CAPS/APS
often none
inections and trauma/surgery/procedure
A patient with APS has APL + and hx fetal loss. What tx would you recommend for this patient during pregnancy?
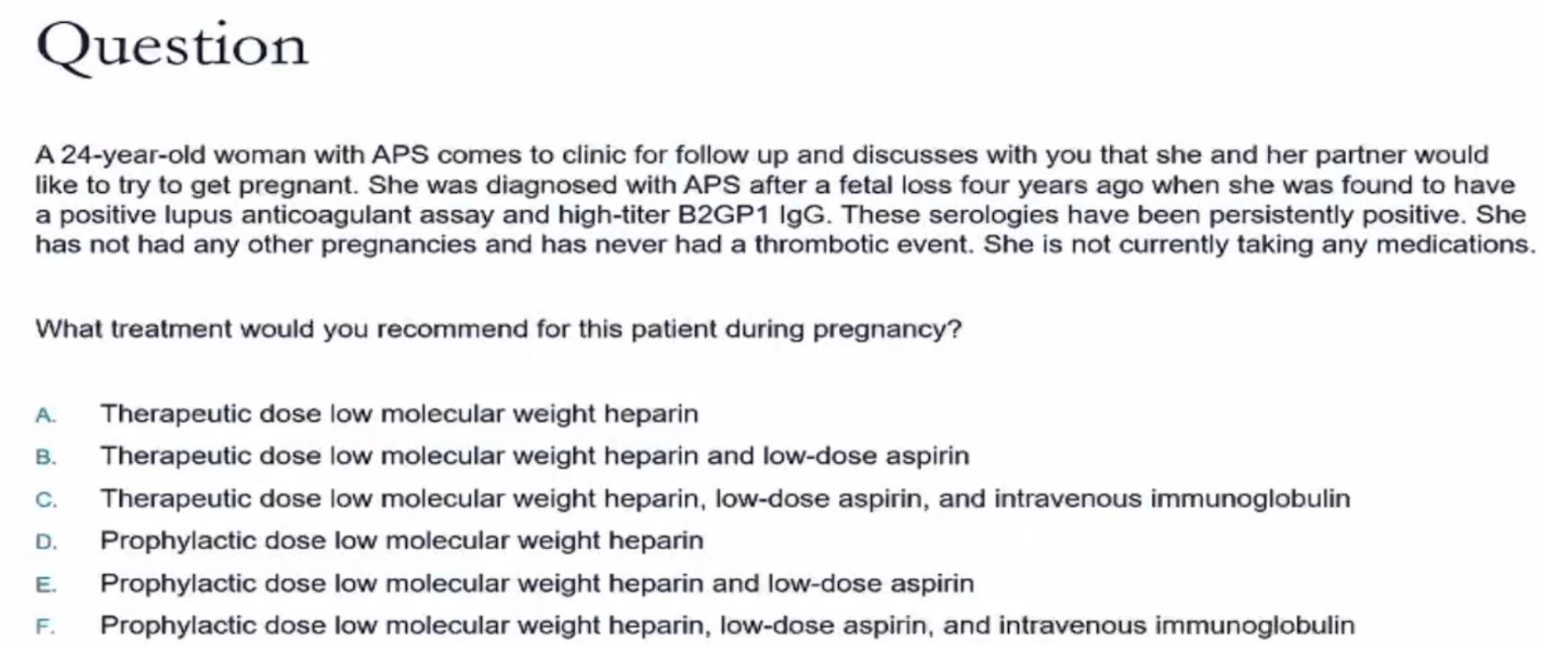
E. Prophylactic dose LMWH and low dose aspirin
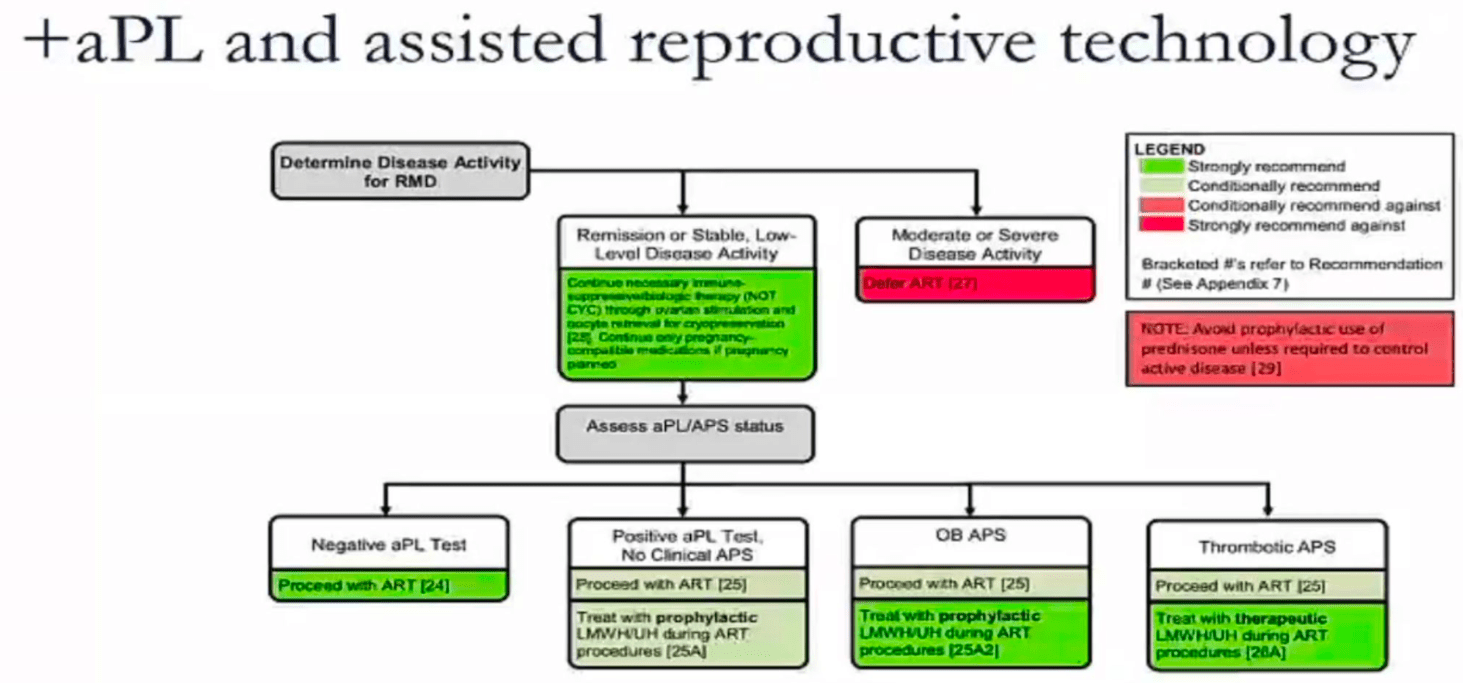
how should you treat patients undergoing assisted reproductive technology like IVF? regarding aPL carriers, OB APS and thrombotic APS
aPL carriers (no APS) still are conditionally recommended to go on prophylactic LMWH during ART - ART (Assisted Reproductive Technology).
OB APS - strong recommendation for prophylactic LMWH
Thrombotic APS - THERAPEUTIC LMWH during ART
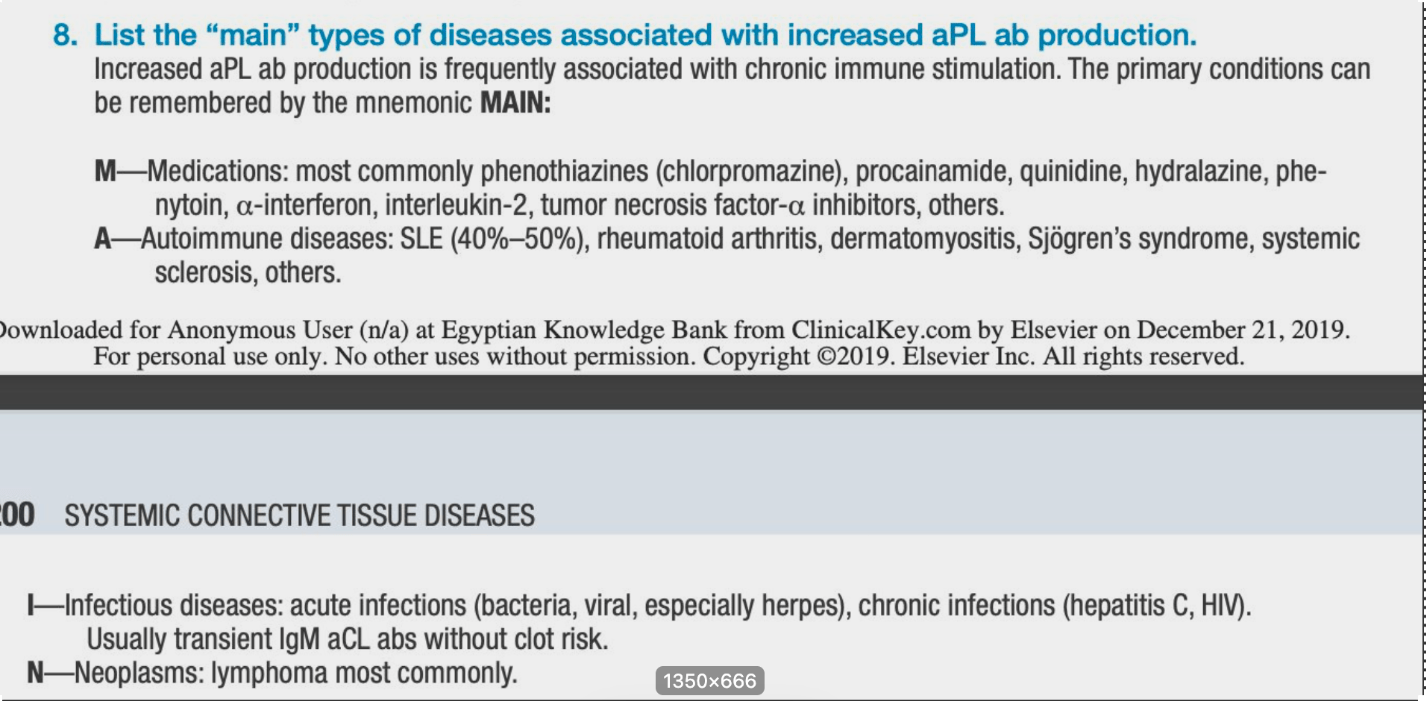
Name the four etiologies associated with increased aPL ab production (hint: MAIN)
Medications, CTDs, infections, neoplasms
should we screen every lupus pt for APS antibodies
Yes, (per UCSF speaker) good to have for pregnancy management decisions. good to have also in setting of thrombotic event rather than searching for them after the event.
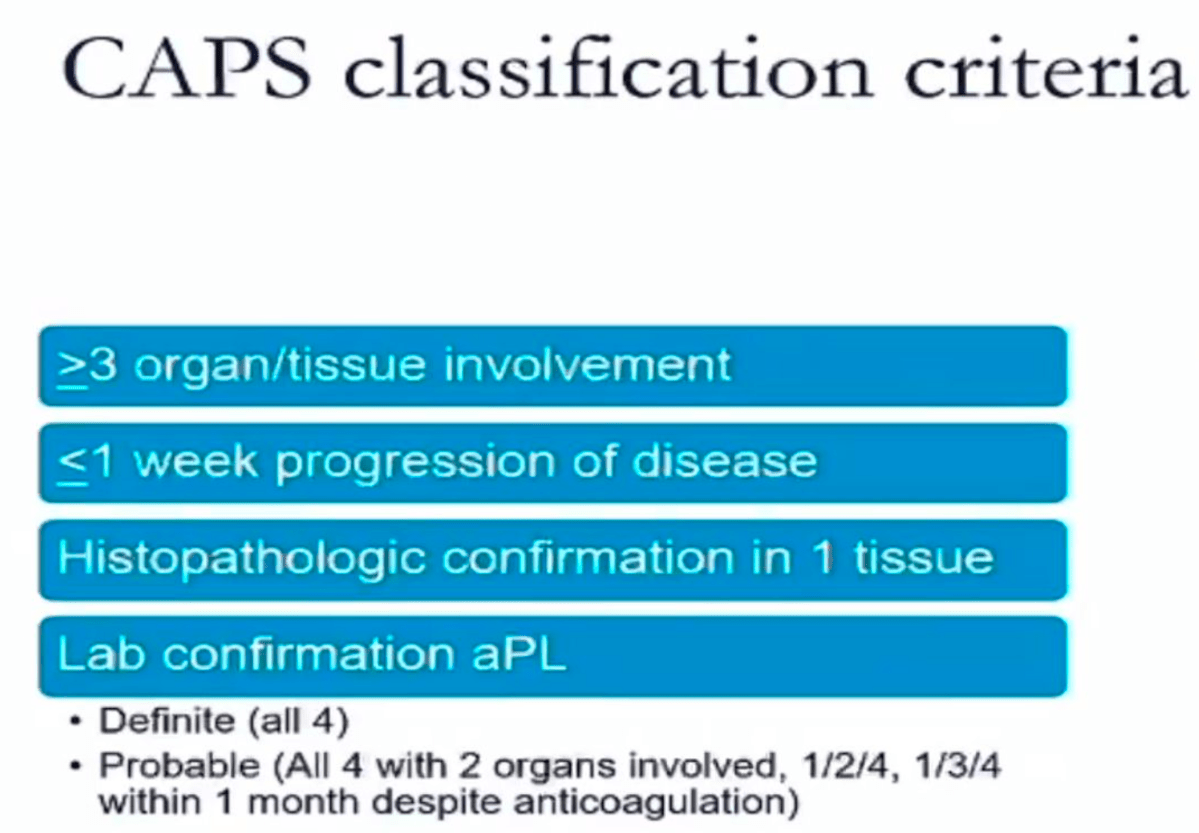
What are the 4 CAPS classificcation criteria
distinction of Libman-Sacks endocarditis from infectious endocarditis seen on ECHO?
APS AFFECTS BOTH SIDES OF THE VALVE
also will note small vegitations.
negative blood cultures.
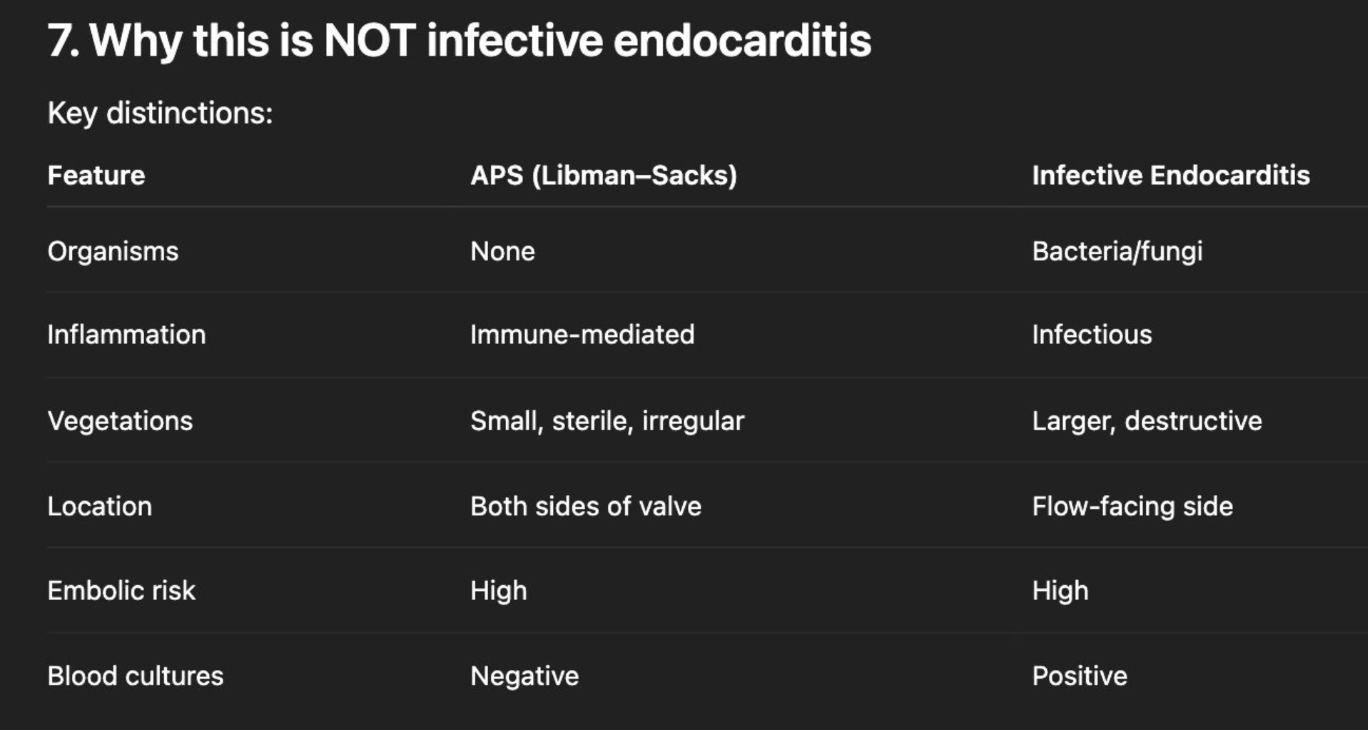
Also will have valve damage from chronic injury from inflammation and fibrosis