TAKE MY BREATH AWAY
LOOK AT THIS RADIOGRAPH
DEM BONES DEM BONES DEM DRY BONES
DONT GO BREAKIN MY HEART
MISCELLANOUS
100
3 CXR findings you may see with a tracheobronchial injury
1. Pneumomediastinum
2. Subcutaneous / mediastinal emphysema
3. Rib fractures
4. Pneumothorax
100
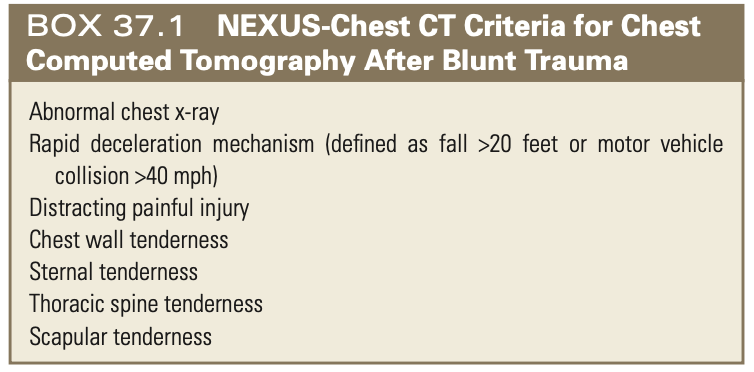
List 3 indications for CT chest after blunt trauma
100
Define flail chest
Results when three or more adjacent ribs are fractures at two points, allowing a free segment of the chest wall to move in paradoxical motion
100
What might you concerned for in this case:
Myocardial concussion
- acute form of blunt cardiac trauma that is usually produced by a sharp, direct blow to the midanterior chest that stuns the myocardium and results in brief dysrhythmia, hypotension, and loss of consciousness. It is a rare event and primarily occurs in adolescents, especially those playing sports involving hard spherical objects (e.g., baseballs, hockey pucks).
100
What further workup may be indicated for pts with 1st rib and/or sternal fractures?
Troponin, CK, ECG, consider CTA chest
200
3 types of pneumothorax
1. Simple
2. Communicating
3. Tension
200
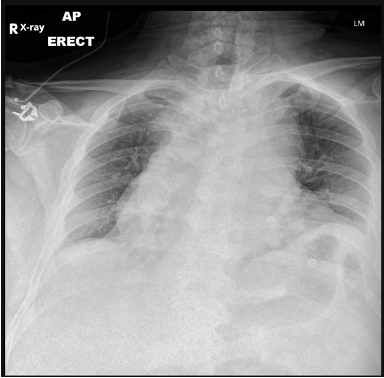
Interpret this CXR

Alveolar infiltrates suggesting pulmonary contusion. Also pneumopericardium, pneumomediastinum.
200
This is the major cause of respiratory insufficiency in patients with flail chest?
Underlying pulmonary contusion
200
This is the most common ventricle to be affected in ventricular rupture and why?
Right ventricle
200
Finding air in these two anatomic spaces on XR may suggest esophageal perforation.
1. Retropharyngeal space - cervical esophageal perf
2. Mediastinal space - thoracic esophageal perf
300
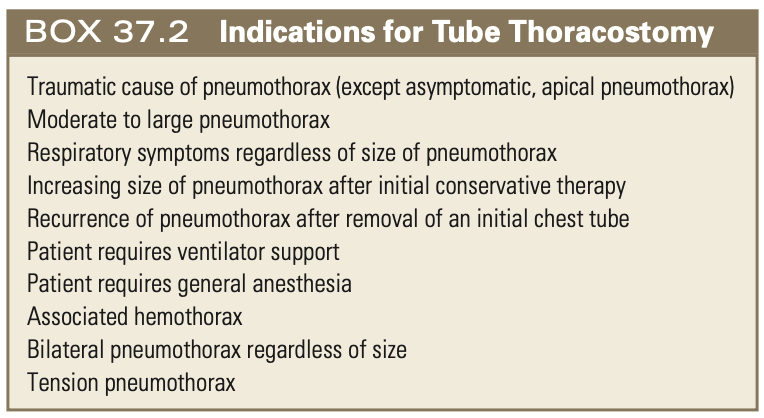
5 indications for tube thoracostomy
300
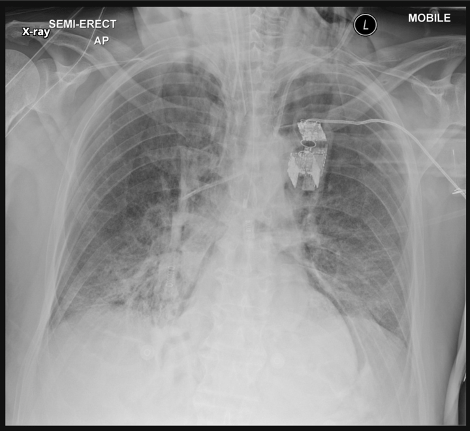
This CXR is concerning for what?
Aortic dissection - >8 cm when supine or >6 cm when upright
300
4 possible complications associated with rib fractures
pneumothorax, hemothorax, pulmonary contusions, post-traumatic pneumonia, costochondral seperation, atelectasis, post-traumatic neuroma, empyema, non-union
300
If someone does not immediately die after myocardial rupture, they are at risk of developing this.
Pericardial tamponade
Two-thirds of patients with cardiac rupture have an intact pericardium and are protected from immediate exsanguination. These patients may survive for a brief period but will then develop significant hemopericardium and pericardial tamponade. One-third of patients with cardiac rupture have associated pericardial tears and succumb promptly to exsanguination.
300
You have inserted a chest tube for a patient with flail chest and pneumothorax, but notice the pleurevac is bubbling continuously indicating a persistent air leak. What else are you worried about?
Tracheobronchial and/or esophageal injury
400
An 84 year old man was cycling and ran into a tree. He has some anterior chest wall pain but no rib fractures, no pneumothorax, is vitally stable and not hypoxic, and appears well apart from some mild increase resp rate and shallow breathing. You worried about this for this patient population in particular?
Pulmonary contusion.
400
What is this finding and what might it suggest?

Air in retropharyngeal space - esophageal rupture
400
3 possible injuries caused by rib fractures
lung laceration, splenic laceration, liver laceration, pleural laceration, diaphragm laceration
400
What guidelines should be used to determine if a patient would be appropriate for an emergent ED thoracotomy in the setting of blunt chest trauma?
East Guidelines

400
What is the most common site of blunt aortic injury and why?
Aortic isthmus, descending aorta just distal to left subclavian artery.
Descending thoracic aorta relatively fixed by tethering of intercostal arteries and ligaments arteriosium, but arch is relatively mobile,
Sudden deceleration- more mobile aortic arch swings forward producing shearing force / whiplash effect at aortic isthmus
Also lateral oblique compression - bending of arch over Left mainstream bronchus and pulmonary artery

500
Describe pathophysiology of diaphragmatic rupture and its complications.
Increased intra-abdominal or intrahtoracic pressure from blunt trauma ruptures diaphragm. Negative intrathoracic pressure with respiration increases risk of herniated abdominal viscera, strangulation, etc.
Due to degree of pressure required, often associated with other intra-abdominal organ injuries.
Diagnosis often delayed due to distracting injuries, progression of injury over time.
500
Interpret this CXR
Pneumomediastinum
500
Interpret this XR
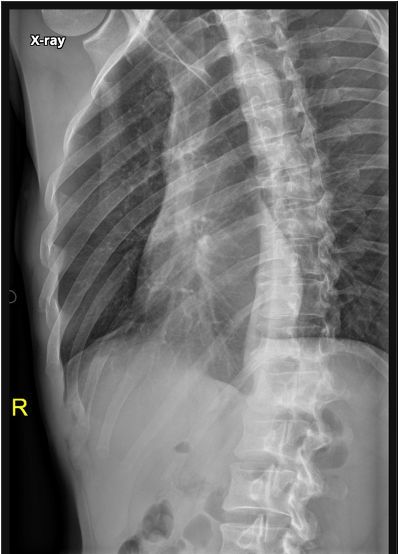
Right 4th-6th rib fractures
500
A patient presents after an MVC with obvious signs of blunt injury to the chest (bruising, flail chest). He arrests with EMS while en route to the hospital. When he arrives to the ED he has no spontaneous ventilation, and no obvious signs of life. The medical student who you are working with suggests that you proceed with ED thoracotomy. What do you do?
Do not.
Blunt + no signs life = Do not proceed
Blunt + signs of life = consider
500
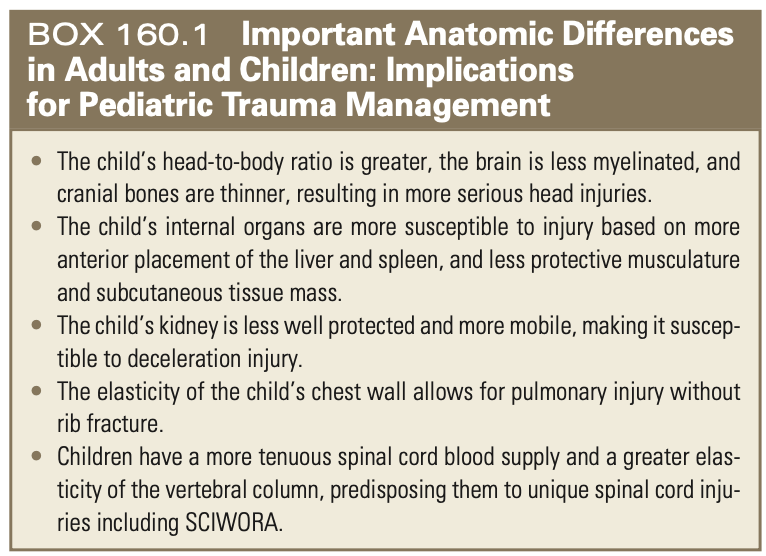
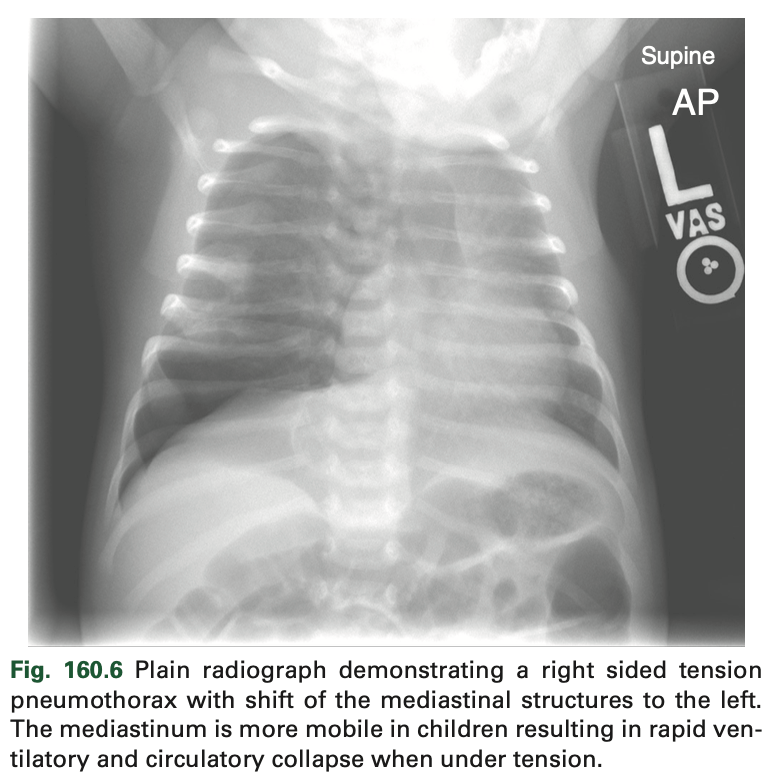
Name two differences in pediatric and adulty thoracic anatomy that may affect blunt thoracic injury.
1. More elastic chest wall lower risk of rib fractures, but pulmonary contusions still common
2. More mobile mediastinal structures while pneumothorax less common, mediastinal shift and tension physiology may be more likely to develop when pneumothorax present.