GI
Heme
Oncology
Miscellaneous
100
True or false
Hpylori testing is indicated in patients with typical GERD symptoms
False
100
What is the plasmic score used for ?
estimate the probability of severe ADAMTS13 deficiency (<10%) in a patient with suspected TTP, and to decide whether to start urgent plasma exchange before ADAMTS13 results return.
100
When is a mastectomy indicated in Ductal carcinoma in Situ ?
If BRCA mutation is positive
100
standardized diagnostic criteria used to diagnose functional gastrointestinal (GI) disorders
Rome Criteria
Fun fact most GI criteria are named after cities:
Milan for Liver cancer, Glasgow for pancreatitis, Chicago for Achalasia.
200
35 year old male with 2 years on intermittent chest pain
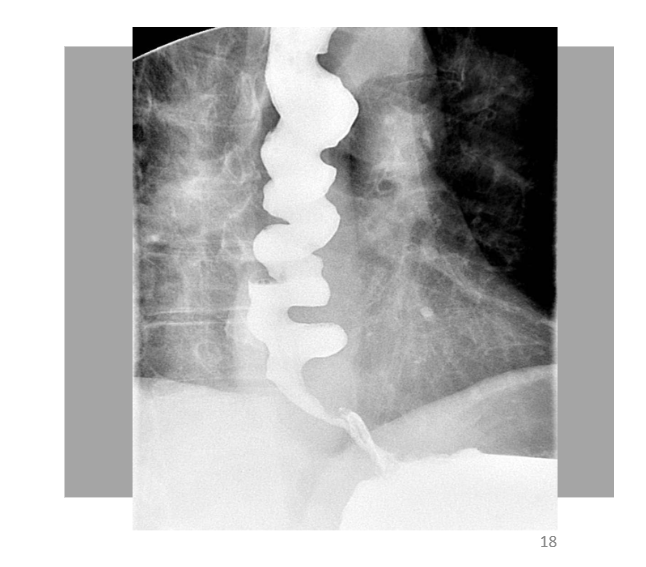
Diffuse esophageal spasm
200
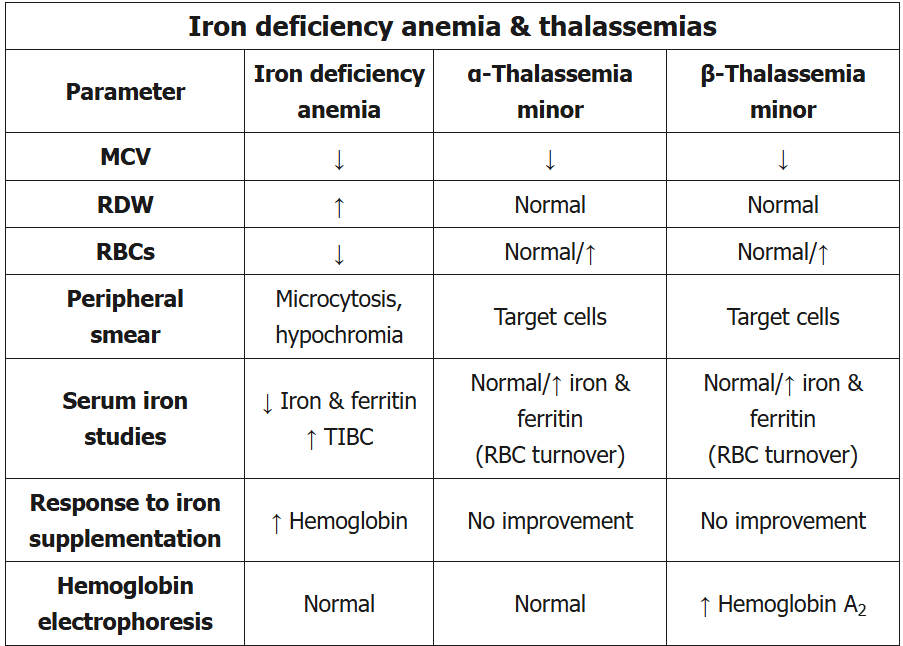
50 year old man comes for a physical, he is asymptomatic. Physical examination is normal
CBC: RBC: 5.2 m. Hgb: 12. RDW normal. TIBC is normal. MCV: 64, WBC and platelets are normal. Hemoglobin electrophoresis is normal.
What's your Dx?
Alpha thalassemia
The clue is the normal RBC count with severe microcytosisand normal Hemoglobin
200
A 64-year-old postmenopausal female presents with 3cm left breast mass. Needle biopsy confirms invasive ductal carcinoma. Undergoes left lumpectomy and axillary node dissection. Final path confirms 3.5cm ER+/HER2-, with 2 positive nodes. She undergoes adjuvant chemotherapy followed by radiation. She is then placed on adjuvant endocrine therapy with letrozole. Which of the following would represent an appropriate component of surveillance strategy?
- Liver function tests every 6 months x5 years
- CT CAP annually x5 years
- Bone density scan every 2 years
- MRI + mammogram BL annually
- PET annually
Bone density scan every 2 years.
Aromatase inhibitors carry a risk of causing osteoporosis.
200
A 60-year-old woman with no PMH presents with 2 weeks of fatigue and low-grade fever. PE showed scleral icterus, Generalized lymphadenopathy, hepatosplenomegaly.
Labs: Hgb 5, WBC's 70.000, Plt 70, retic count 12, TB 6.3 with direct Bili 1.6. Cog studies were normal
Mention the finding on peripheral blood smear?
Spherocytes
Warm agglutinin autoimmune hemolytic anemia (AIHA) is a common complication of chronic lymphocytic leukemia (CLL) and is characterized by a positive direct antiglobulin (Coombs’) test and spherocytes on peripheral smear.
300
Mention 3 medications that can cause pill induced esophagitis ?
Tetracycline, doxycycline
Iron
Potassium Chloride pill
Oral bisphosphnates
Aspirin, NSAIDS.
300
An 82-year-old man with untreated chronic lymphocytic leukemia (CLL) presents with sudden-onset back pain. Exam reveals lymphadenopathy, splenomegaly, and localized spinal tenderness. Imaging shows an L2 compression fracture.
Penitent labs: K 8.2, Wbc's 180, 000 , Hct 27, Plt 85
What's the next step regarding the hyperkalemia ?
Redraw K from an arterial blood draw.
300
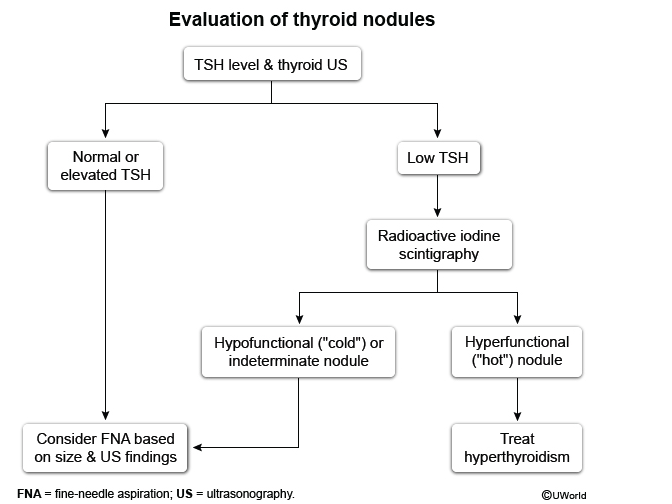
A 30-year-old woman with no thyroid-related symptoms is found to have an incidentally discovered thyroid nodule after a CT scan done for trauma.
Labs: TSH 0.12 (Low), T3 190 (High), T4 1.8 (Normal)
Thyroid US: solid right lobe hyperechoic nodule measuring 2.3×1.6×1.2 cm with no evidence of microcalcification or internal vascularity.
What's the best next step?
Radioactive Iodine Scan
300
A 31-year-old woman with hypothyroidism has persistent symptoms of fatigue, cold intolerance, abdominal bloating, and cognitive fog.
She properly takes her Levothyroxine when checking.
Hgb: 9.4 g/dL
MCV: 66 µm³
AST: 62 U/L
ALT: 74 U/L
TSH: 20 mU/L
Free T4: 0.8 ng/dL
What would you like to order next ?
IgA ATT ab
Celiac disease is more likely to coincide with other autoimmune diseases, in this case its causing malabsorption of the levothyroxine and persisted symptoms. the clue is Microcytic anemia which caused by iron deficiency
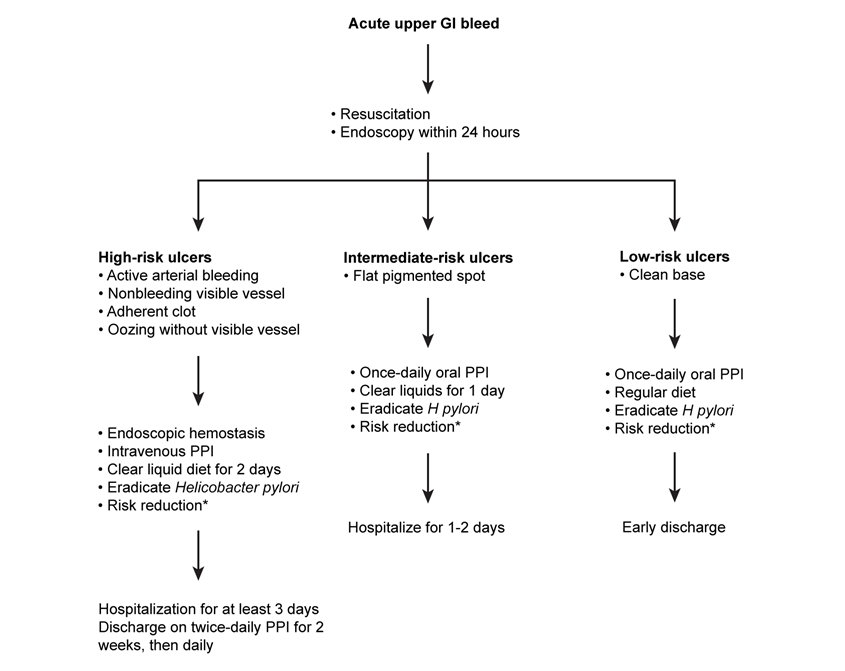
400
A 57-year-old woman presents with acute upper gastrointestinal bleeding, evidenced by melena (black stools) and hematemesis over 24 hours.
Hemodynamically stable after fluids
Hb 9.2 g/dL
1.5-cm gastric antral ulcer, No active bleeding Adherent clot present, Endoscopic hemostatic therapy performed
Admit or Dc and if admit to what floor?
Keep Npo or start a diet and if so what diet ?
Admit to Medsurg with clear liquid diet
400
A 22-year-old African American male is evaluated for gross hematuria. He has had 5 days of grossly bloody urine every time he urinates. He had a similar episode one year ago which lasted 5-10 days and resolved spontaneously. He is muscular with BMI of 25, otherwise exam is unremarkable.
CBC showed HCT 40%, cmp was negative. UA was remarkable for Blood gross, Red blood cells many/hpf, Casts none
Renal US was also negative
What test is most likely to confirm the diagnosis ?
Hgb electrophoresis.
400
53-year-old postmenopausal woman finds breast lump. Ultrasound and mammography confirm a suspicious 3cm mass. A core biopsy is positive for infiltrating ductal carcinoma. A lumpectomy and axillary node dissection are done. The cancer is 3cm with 2 positive axillary nodes. ER/PR negative, HER2 negative.
Which of the following do you recommend?
- Repeat surgery with conversion to mastectomy
- Local radiation with tamoxifen
- Adjuvant chemotherapy followed by radiation
- Close follow up with monthly exam
- Local radiation alone
Adjuvant chemotherapy followed by radiation
TNBC adjuvant therapy is chemotherapy. Given positive nodal disease with lumpectomy radiation is indicated
400
52 year old male who works as auto mechanic presented with a week of pain and discoloration of fingers:
Labs: ANA 1:160, C3 56 (low), C4 5 ( low), RF 560 (high)

What is the Dx???
Type 2 mixed cyroglobenima or Hepatits C infection
- Type II and III cryoglobulinemia (i.e., mixed cryoglobulinemia): 90% of cases
- Viral infection: most common etiology (HCV infection in 70–90% of cases) [4]
- Formation of hepatitis C IgG and IgM rheumatoid factor → immune complex formation with hepatitis C antigen → complement activation and inflammation of blood vessels
- Other
- Autoimmune diseases (e.g., Sjogren syndrome, SLE, rheumatoid arthritis)
- Lymphoproliferative disorders
- Idiopathic (i.e., essential mixed cryoglobulinemia)
- Viral infection: most common etiology (HCV infection in 70–90% of cases) [4]
- Type I cryoglobulinemia: 10% of cases (e.g., in multiple myeloma, CLL)
500
A 51-year-old woman presents with 6 months of chronic diarrhea and bloating, having 4–6 bowel movements daily, including occasional nocturnal stools, and unintentional weight loss (8 lb).
PE: Skin thickening & tightening at the finger with face telangiectasia.
(Hb 10.8, MCV 104)
B12 is low
folate is elevated
Negative (tTG)
- Stool studies Negative for ova or parasites
- Colonoscopy a year ago was negative
What your test of choice ?
SIBO, Hydrogen breath test
500
A 62-year-old man comes to the hospital due to 2 days of bilateral lower extremity swelling and throbbing pain. Two weeks ago he was admitted to a different hospital with a non-ST elevation myocardial infarction. he was initially treated with ACS protocol but was found to 3 vessel disease and underwent a CABG.
Labs showed Hgb 11.4, Plt 80, PT 12, PTT 23, INR 0.8
US of lower extremity: extensive bilateral DVT.
What's your treatment of choice?
Direct thrombin inhibitor.
Delayed onset HIT.
Delayed-onset HIT - immune mediated due to high-titer antibodies against heparin-PF4 complexes in the absence of circulating heparin. Cases typically arise 5-19 days after heparin cessation; therefore, most patients present in the outpatient setting. Thrombocytopenia with or without life-threatening arterial or venous thrombosis are the norm.
500
A 58-year-old woman with no significant medical history presents with 5 days of progressive headache and dizziness.Neurologic exam is normal (no focal deficits, no meningeal signs).
Brain imaging shows a single 2 × 3 cm frontal lobe lesion at the gray–white matter junction with vasogenic edema.
CT chest shows spiculated 2.5 cm right upper-lung mass with ipsilateral bronchial lymphadenopathy.
What's the most appropriate next step regarding the brain lesion ?
Brain surgery
This patient likely has primary lung cancer, which may be small cell (SCLC) or non-small cell (NSCLC). Brain metastases from SCLC appear to respond initially to chemotherapy, but studies have shown variable overall response rates without significant survival benefit. Adding whole-brain radiation (WBRT) improves the response rate to chemotherapy but without significant survival benefit. NSCLC is not as chemosensitive as SCLC, and brain metastases respond better to WBRT and/or surgical resection. As a result, surgical resection is usually considered for brain metastases due to SCLC or NSCLC.
500
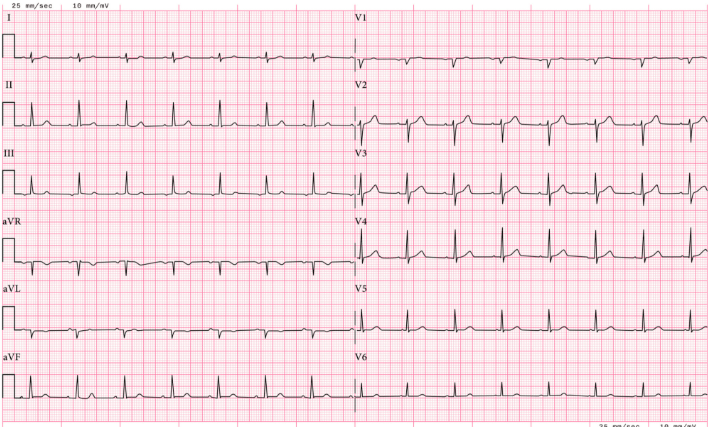
A 76-year-old woman with severe ischemic cardiomyopathy (EF 30%) and chronic atrial fibrillation presents with 2 weeks of fatigue, nausea, abdominal pain, poor appetite, and visual disturbances (black spots).
Labs: K 6.4, Hco3 18, Cr 2.2, Digoxin levels < 1.8 normal is < 2.
In the ED she had multiple runs of V.tach.
EKG: shows a regular narrow-complex rhythm at 48/min, no P waves, and occasional ventricular premature beats
What's the treatment?
Digoxin Fab fragments
Digoxin toxicity does not correlate well with serum digoxin levels (toxicity can occur with normal or subtherapeutic levels); therefore, the diagnosis should be based on clinical presentation and ECG findings. Initial treatment involves intravenous hydration. In addition, digoxin-specific antibody (Fab) fragments should be given in patients with any of the following:
- Life-threatening cardiac arrhythmia (eg, advanced conduction block with junctional rhythm as in this patient)
- End-organ dysfunction due to hypoperfusion
- Hyperkalemia (serum potassium >5.5 mEq/L)