Rob Summer's Fav Organ (Cards)
Butts and Guts (GI)
Only Chao Knows (ID)
Make My PD Proud (Rheum)
Hormone Havoc (Endo)
100
Ms Beam presents to the ER with crushing sub-sternal chest pain. Her ECG is shown below. What class of medications is contraindicated which would normally be used for post-ACS care?
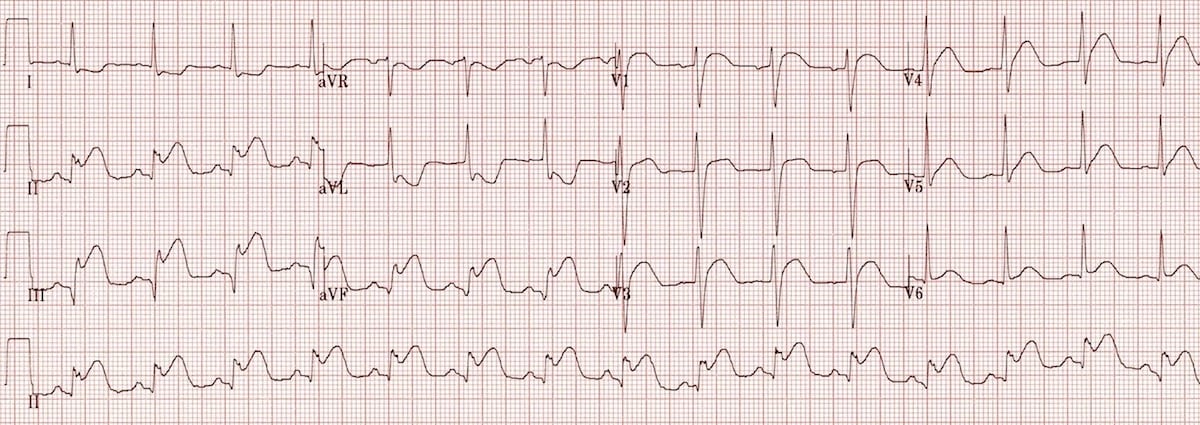
Nitrates
Decreased preload -> collapse of the RV
100
In a patient with mild acute gallstone pancreatitis who has clinically improved and has no evidence of cholangitis or ongoing biliary obstruction, guidelines recommend performing this definitive intervention during the index hospitalization to reduce recurrence.
What is cholecystectomy prior to discharge?
100
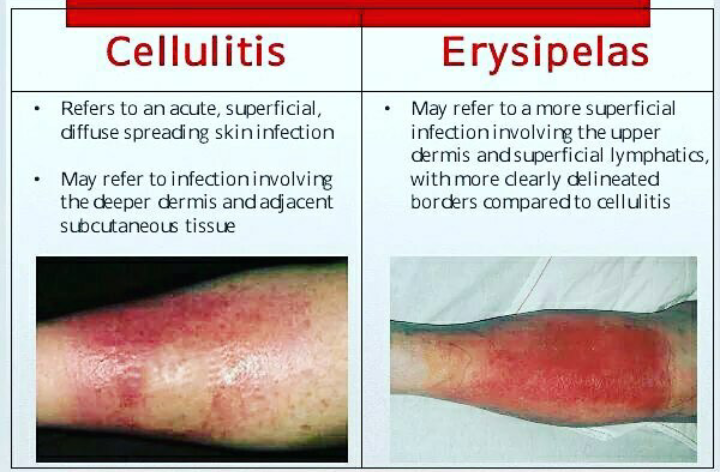
Ms. Smith walks into your office with a well-demarcated, tender, brightly erythematous rash with associated fevers for the past 5 days. What is her diagnosis?

What is erysipelas?
More superficial infection of the dermis than cellulitis
100
What antibody is most commonly associated with Limited Cutaneous Systemic Sclerosis?
Anti-centromere

100
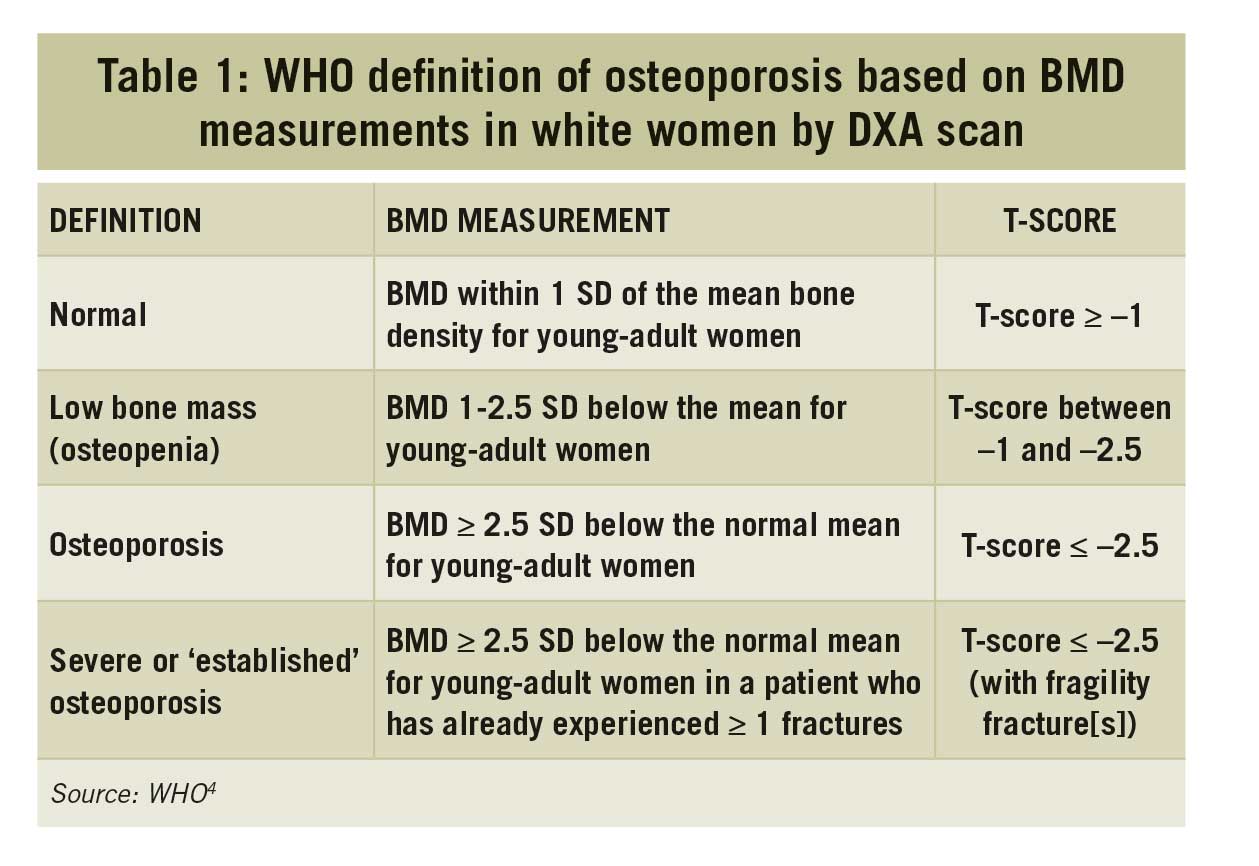
Osteoporosis is diagnosed by either ____ or ____.
What is a DEXA T-score of </= 2.5 or history of fragility fracture (fracture from a fall at standing height or lower, or fracture occurring spontaneously regardless of BMD)?
200
A patient presents to a non-PCI capable hospital with a STEMI. If transfer to another hospital and performance of a PCI is not possible within ____ minutes, a fibrinolytic strategy should be pursued instead.
What is 120 minutes?
Door-to-PCI time goal <90 minutes at PCI capable hospitals, <120 minutes at non-PCI hospitals including transfer time. If they cannot get to a PCI capable hospital in 120 minutes, then fibrinolysis should be performed within 30 minutes.
200
A 30M presents with dysphagia that is refractory to multiple rounds of PPI, H2 blockers, and lifestyle modification. EGD demonstrates longitudinal furrows and luminal narrowing. Esophageal biopsy shows eosinophil counts of 15 or greater in 3 locations. What is the most likely diagnosis?
What is Eosinophilic Esophagitis?

200
This EBV-related lesion is most commonly seen in severely uncontrolled HIV
%2Fcase%2Fdetail_images%2Fc272_detail.jpg&w=1920&q=75)
What is Primary CNS lymphoma?

200
This supplement can be considered with methotrexate to reduce the toxicity of the drug.
What is folate supplementation?
200
This is the radiologic cutoff criteria for an adrenal incidentaloma that requires no additional follow-up imaging.
What is a homogeneous mass, density </= 10 HU, any size?

300
Mr. Rodgers presents with increased wall thickness on TTE, a low voltage ECG, bilateral carpal tunnel syndrome and progressive leg swelling. He recently was found to have an elevated M spike on lab work. What underlying process is driving his cardiomyopathy?
What is Amyloidosis? (specifically AL Amyloidosis)
300
A 60F presents with a few months of watery diarrhea. She takes NSAIDs for chronic back pain and fluoxetine for anxiety. Colonoscopy demonstrates a normal mucosa. Colon biopsies demonstrate a subepithelial collagen band and inflammatory infiltration of the lamina propria.
What is the most likely diagnosis?
What is microscopic colitis?
300
A 55 year old patient with a history of liver transplant presents to the hospital with fevers, cough, sinus pressure and malaise for a few days. His CT scan is shown below. Gram stain of blood cultures demonstrated gram negative septating hyphae. What is the most likely microbe?
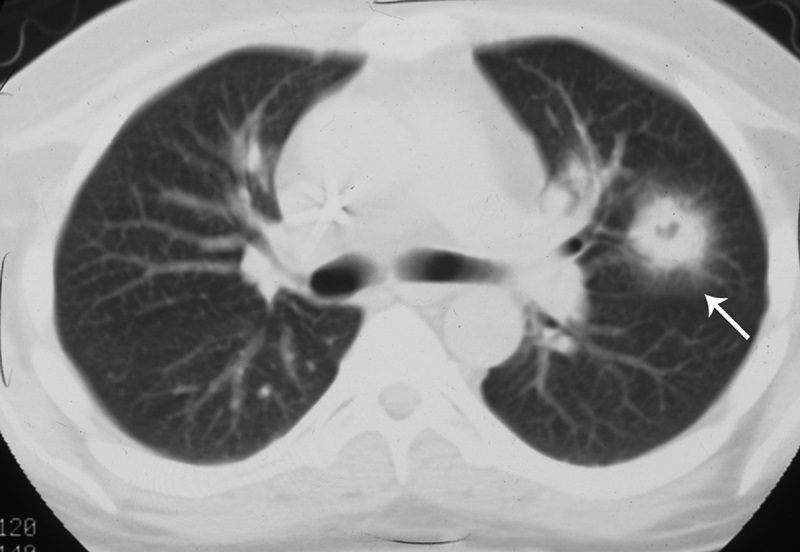
What is Aspergillus?
Halo sign on CT scan indicative of hemorrhage of the adjacent tissues
300
A 70 y/o F with early morning stiffness lasting 90 minutes and joint pain in both hands. Right knee joint pain for the past 2 months. ESR 48. X-ray obtained shown below. Rh factor is negative and anti-citrulline antibodies are negative. Symptoms respond to NSAIDs. What is the diagnosis and what will you do next (treatment to initiate)? 
Diagnosis: RA
Tx: Start Methotrexate
300
This is the preferred medical management for a 26yo F with Graves Disease who is planning to become pregnant. (Give medication preference and timing within pregnancy course)
What is propylthiouracil (PTU) within the first trimester?
Methimazole has been linked to esophageal or choanal atresia and aplasia cutis (a congenital skin defect), with a twofold increased risk of major fetal malformations compared to propylthiouracil exposure in the first trimester.
Some clinicians transition to methimazole after the first trimester because propylthiouracil can cause rare but clinically significant hepatotoxicity.
400
A 29yo F presents with chest pain two weeks after an uncomplicated delivery. She had an uncomplicated pregnancy, had no previous medical history, no cardiac risk factors, and no family history of atherosclerotic disease. Her troponins are elevated and ECG demonstrates ST segment elevation in the inferior leads. What is the most likely diagnosis?
What is spontaneous coronary artery dissection (SCAD)?

400
What is the formula for stool osmotic gap?
290 - 2 (Na + K)
Osmotic gap < 50 indicates secretory diarrhea and gap > 100 indicates osmotic diarrhea

400
What is the mechanism of creatinine elevation after TMP/SMX administration?
Competitive inhibition of creatinine excretion by Trimethoprim

400
A 54F presents to your clinic with facial erythema, rough, cracked, scaly skin along the lateral aspects of the digits and palms and violaceous slightly scaly plaques over the prominences of the hands and calcinosis cutis. Anti- t-RNA synthetase is negative. Characteristic lesions are shown below. What is the most likely diagnosis?

What is dermatomyositis?
400
A hospitalized patient develops polyuria of 75 mL/kg/24 hours (normal: <50 mL/kg/24 hours). Labs show:
Serum sodium: 151 mEq/L (normal: 135–145 mEq/L)
Serum osmolality: 308 mOsm/kg (normal: 275–295 mOsm/kg)
Urine osmolality: 90 mOsm/kg (normal: ~300–900 mOsm/kg, depending on hydration status)
After administration of desmopressin, the urine osmolality rises significantly.
This condition best explains the patient’s findings.
What is arginine vasopressin deficiency (central diabetes insipidus)?
500
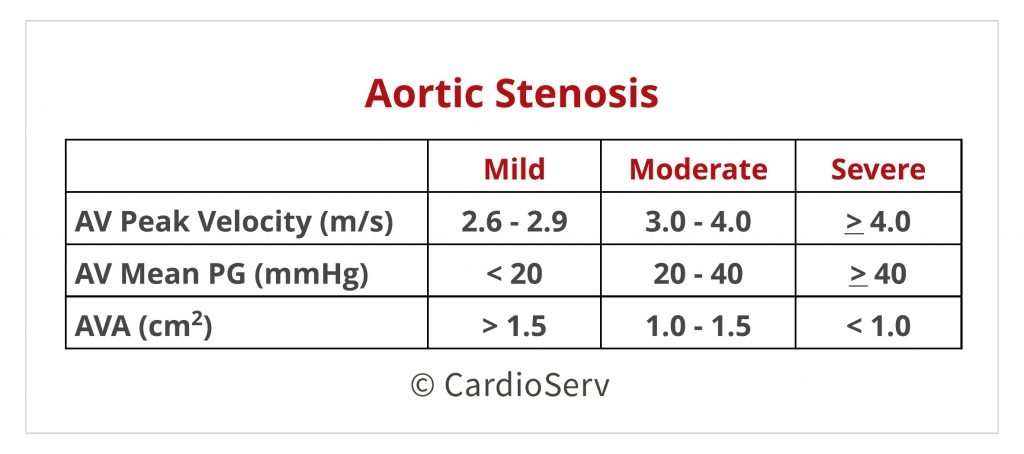
Based on the 2020 AHA/ACC guidelines on aortic stenosis, give two of the three measurements that would qualify a patient's aortic stenosis as severe.
Peak Velocity > 4m/s, AV mean gradient >40mmHg, AV Area <1.0cm2
500
According to the 2016 AASLD Guidelines, give two patient populations that would warrant treatment of their chronic Hepatitis B infections.
(Could be comorbid conditions, phase of infection, etc)
Patients needing treatment for Hep B include those with decompensated cirrhosis, those with immune-active Hep B (elevated ALT, HBeAg +, elevated HBV DNA), reactiveated Hep B (elevated ALT, HBeAB +, elevated HBV DNA), pregnant patients with a HBV DNA level > 200,000, select immunocompromised patients (typically those starting biologics), and those with cirrhosis and low level viremia (DNA level <2000).
500
Name either an oral two-drug PrEP (pre-exposure prophylaxis) or an intramuscular one drug regiment for PrEP for HIV prevention.
Tenofovir disoproxil fumarate (TDF) or tenofovir alafenamide (TAF) plus emtricitabine; Cabotegravir
TDF is less preferred with osteoporosis or reduced eGFR 30 to 60%
500
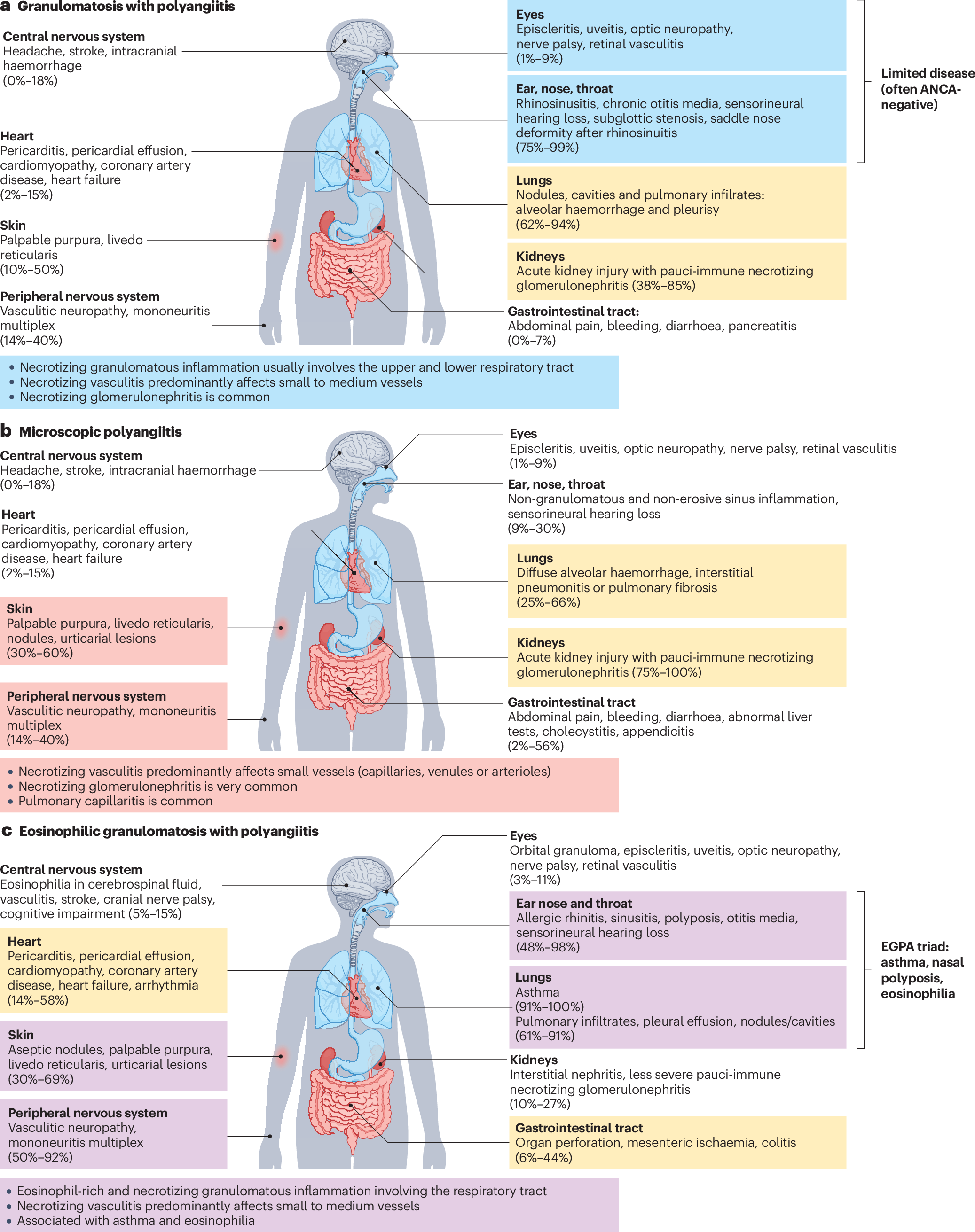
A 64M presents to the hospital with renal failure and hemoptysis. He has bilateral neuropathy. Lab testing demonstrates a positive p-ANCA. CT Chest shows alveolar hemorrhage with pulmonary fibrosis. Biopsy of the muscles demonstrates a pauci-immune nongranulomatous vasculitis without eosinophils. What is the most likely diagnosis?
What is microscopic polyangiitis?
500
A 68yo F is admitted to ICU for urosepsis. PMHx notable for hypothyroidism, but no levothyroxine is present on med rec.
Vitals: T 93.2F, BP 90/40, HR 64, RR 8, and SpO2 90% (RA)
PE: periorbital edema, 3+ pitting edema in BL LE's, absent deep tendon reflexes, lethargic and slow to respond to questions
Labs: Na 130, TSH 29, free T4 0.1, serum cortisol 21
This is the most appropriate medical management (include recommended dosing).
Myxedema coma:
What is IV Levothyroxine? Loading dose of 200-400μg, followed by an oral dose of 1.6 μg/kg/d.
Oral levothyroxine administration is inappropriate because the severe hypothyroidism may cause bowel edema and slowed oral absorption of levothyroxine.
Steroids can be held if random serum cortisol level >18μg.