Kodas
Meds
All about psoriasis
Path Party
Random Rumba
100
Name this condition:

Pityriasis rosea: onset ~10-35 yo; typically lasts 6-8 wks but can be >5 mo.
Herald patch ~2-4 cm but ranges 1-10 cm that may occur as first sign or simultaneously with widespread eruption on the trunk > neck or extremities. Lesions oriented w/ long axis along Langer cleavage lines on posterior trunk and proximal extremities (Christmas tree pattern).
+/- mild prodrome w/ HA, fever, arthralgias, general malaise. Prototypic paraviral exanthem; HHV-6/7; HHV8, H1N1 influenza, covid. May have modest seasonal variation (peak spring and fall; or rainy season).
100
Which biologics are known to paradoxically induce psoriasis?
TNF inhibitors, most commonly adalimumab and infliximab, may cause plaque psoriasis and/or palmoplantar pustulosis
100
Name this variant:
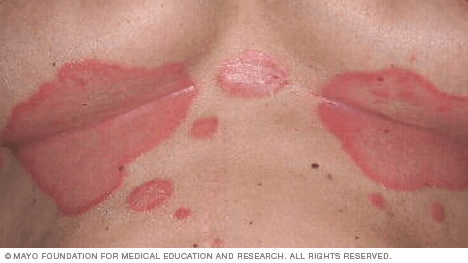
Inverse psoriasis
100
Describe the Auspitz sign
Pinpoint bleeding after removal of white/micaceous scale due to dilated capillaries and suprapapillary plate thinning

100
Strongest HLA association in psoriasis?
HLA-Cw6
---------------------------------------------------------
Presence of HLA-Cw6 confers a RR of 13 for developing psoriasis in the Caucasian population and 25 in the Japanese
Strongly linked to the age of onset of psoriasis: more strongly associated with psoriasis type I (early onset, positive FH) vs. Type II psoriasis (late onset, no family history).
In one case series, expressed in 90% of early-onset psoriasis, in 50% of of late-onset psoriasis; only in 7% of a control population.
200
Name this condition:

Small plaque parapsoriasis: digitate dermatosis
Middle aged and elderly patients. Peaks in fifth decade. 3:1 M:F predominance.
Elongated finger-like pink-brown to yellow-brown patches symmetrically distributed on the flanks. +/- yellow hue (“xanthoerythrodermia perstans”)
SPP: <5cm lesions; LPP: >5cm lesions
Predominantly CD4 T cell infiltrates. Unclear if they are true entities, versus a condition on the spectrum of clonal dermatitis. Generally believed to be benign condition that carries no malignant potential, but there are few case reports of progression (LPP > SPP) into MF.
200
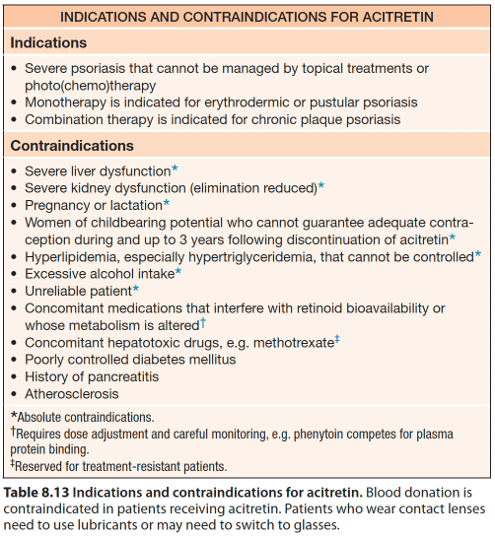
Monotherapy of which systemic agent is effective in treatment of erythrodermic and pustular psoriasis?
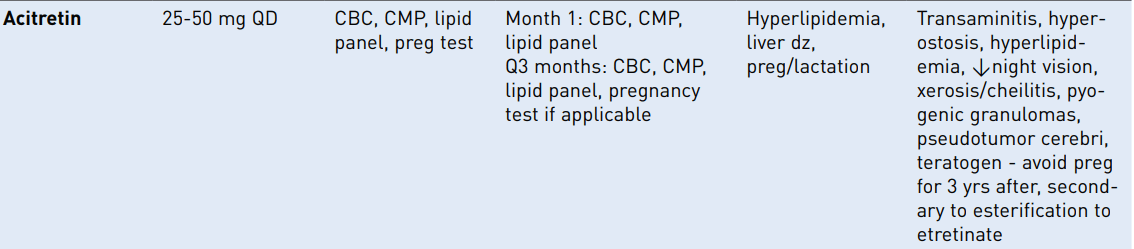
Acitretin (soriatane): 2nd gen retinoid; free metabolite of etretinate. Typically see improvement at 4-6 weeks and maximum benefit may take 3-4 months.
SE: Can cause pseudotumor cerebri if used in conjunction with tetracyclines, pancreatitis from hypertriglyceridemia; hyperostosis (diffuse idiopathic skeletal hyperostosis, a systemic bone-forming condition characterized by the presence of at least three bony bridges at the anterolateral spine)
Do not use if:
PREGNANT
Severely impaired liver or kidney function
Chronically elevated blood lipids
In combo with tetracyclines or MTX
200
Which cytokine has reduced levels of expression in psoriasis?
IL-10
Increase in Th1 (IFNg, IL-2), Th17 (IL-17 A and F) and Th22 (IL-22) cytokines
Reduction in anti-inflammatory IL-10
200
Differential diagnosis for neutrophils in the stratum corneum (name 4 of 6)

200
Name this condition:

Pityriasis rotunda (tinea/pityriasis circinata)
- Third decade of life, children. Slight F>M.
- Patient population: east asian (Japan, China), mediterranean (Morocco, Italy, Israel), african ancestry
No clear unifying cause; absent profilaggrin N terminal domain ~ decreased expression of FLG-2 in some patients.
Most patients are healthy; potential exacerbating factors include malnutrition, mycobacterial dz (TB, leprosy), malignancies (HCC, gastric carcinoma, multiple myeloma), hepatic cirrhosis
Favors trunk/extremities, with large circular and polycyclic lesions, often 10 cm (up to 30 cm) in dm w/ associated fine scale and moderately hyperpigmention w/ a sharp margin. Asymptomatic typically. +/- hypopigmented halo or entirety of lesions hypopigmented
Type I = black or asian patients w/ hyperpigmented lesions associated with malnutrition or internal malignancy, no family history
Type II = younger white patients w/ >30 lesions, sometimes family history, no association with other diseases
300
Name this condition:
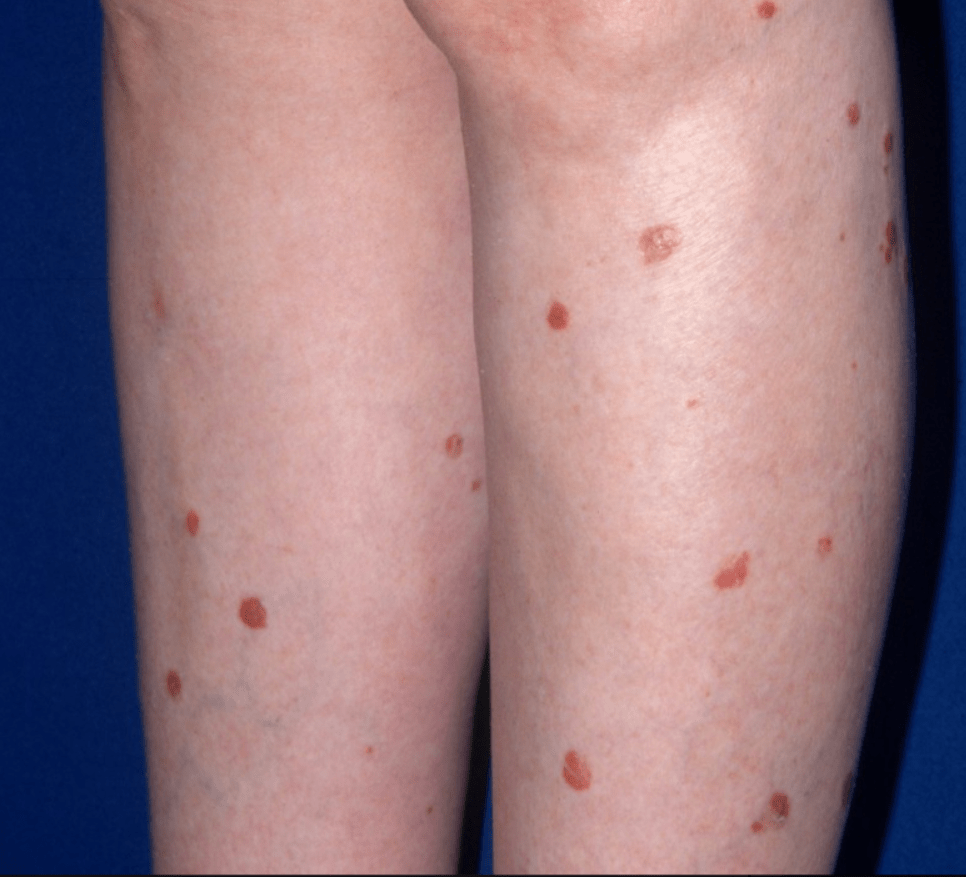
PLC - pityriasis lichenoides chronica
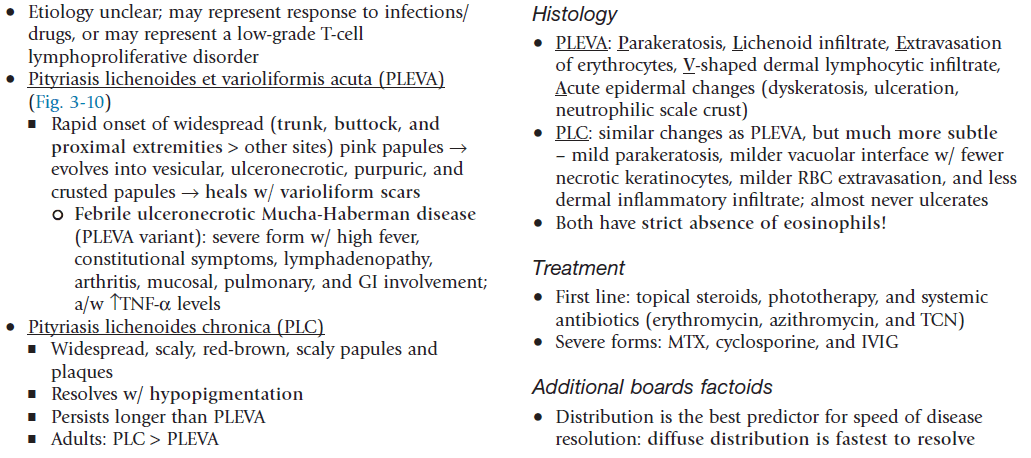
PLEVA (acute) and PLC (chronic) represent two ends of a disease spectrum; both are characterized by recurrent crops of self-resolving lesions
Widespread, scaly, red-brown scaly papules and plaques. Resolves with hypopigmentation
- Lasts longer than PLEVA
- More common in adults > children.
- Distribution is important: diffuse distribution = shorter avg duration (11 mo); peripheral distribution = longest avg duration (33 mo); central distribution = intermediate duration.
300
What is the mechanism of action of tapinarof?
Tapinarof: aryl hydrocarbon receptor modulating agent which decreases Th17/22, promotes epidermal barrier restoration by filaggrin, and upregulates antioxidant activity.
Tapinarof is a topical aryl hydrocarbon receptor (AhR) agonist approved for plaque psoriasis. It exerts its effects by suppressing pro-inflammatory cytokines, including IL-17, IL-22, and TNF-α, normalizing keratinocyte proliferation and differentiation, and upregulating epidermal barrier proteins including filaggrin to promote barrier restoration. It has also been shown to upregulate antioxidant pathways.
300
Name the laser wavelength that can best treat small areas of psoriasis.
Excimer laser: monochromatic 308 nm light from an excimer laser or equivalent source can be used to target individual/smaller psoriatic plaques.

300
Name the differential for this finding (name 4 of 7):

300
What disease is associated with the following skin findings along with fever and arthralgias?

Febrile ulceronecrotic Mucha-Habermann disease (FUMHD):
- Marked by larger, more ulcerative, and necrotic lesions along with fever and arthralgia.
- There may be gastrointestinal, pulmonary, and central nervous system (CNS) involvement.
- No consensus about first-line therapy, but wide variety of treatment modalities have been suggested to be effective, including systemic steroids, MTX, cyclosporine, dapsone, and IVIG.
400
What is this disorder?

Sneddon-Wilkinson / Subcorneal pustular dermatosis
Characterized by annular or polycyclic lesions typically in the flexures, with very superficial (subcorneal) sterile pustules/vesicles with an erythematous base as the hallmark of disease. May be gravity-induced demarcation in some vesiculopustules, with clear fluid superiorly and pus inferiorly.
Cyclic course: as pustules resolve they are replaced by superficial scaling, then new pustules form again.
Biopsy: subcorneal pustule with neutrophils. Normal surrounding epidermis
*Great response to dapsone: resolution usually within 4 weeks, then taper.
Subcorneal pustules in the absence of spongiform pustules and its response to dapsone supports it being a distinct disease entity from pustular psoriasis.
400
What is the mechanism of action of spesolimab-sbzo, and what condition is it approved to treat?
Monoclonbal IL-36R antibody; generalized pustular psoriasis
Spesolimab-sbzo (Spevigo) is a humanized IgG1 monoclonal antibody that blocks IL-36R, inhibiting downtream inflammatory signaling.
FDA approved in 2022 for treatment of GPP in adults. Additionally approved for pediatric patients ≥12 years of age and weighing at least 40 kg.
Administered as a single 900 mg intravenous infusion over 90 minutes. A second 900 mg IV dose may be administered one week later if flare symptoms persist. More recently, a subcutaneous formulation has been approved for maintenance therapy in eligible patients, allowing ongoing control between flares.
Most common adverse reactions reported in ≥5% of patients treated with SPEVIGO in the clinical trial leading to FDA approval were asthenia and fatigue, nausea and vomiting, headache, pruritus and prurigo, infusion site hematoma and bruising, and urinary tract infection (UTI).
Specific adverse reactions include increased infections (UTI, HSV, cellulitis), DRESS, Guillan-Barre syndrome
400
What is name of this variant?
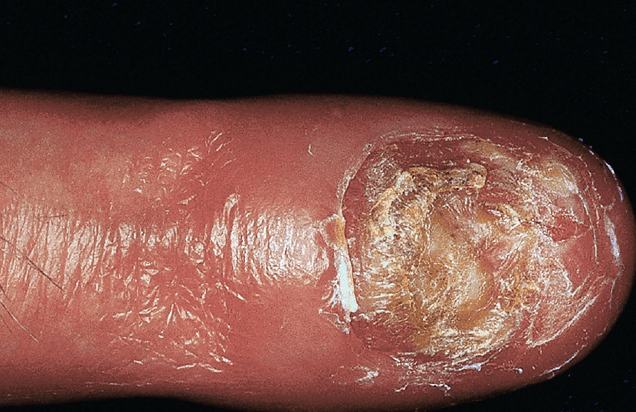

- pustules that coalesce into "lakes of pus" on the distal fingers, toes, and nail beds. Pustulation results in scaling and crust formation, and shedding of the nail plates.
May be associated with annulas migrans of the tongue (migratory annular erythematous lesions w/ hydrated white scale)

400
Name the disease
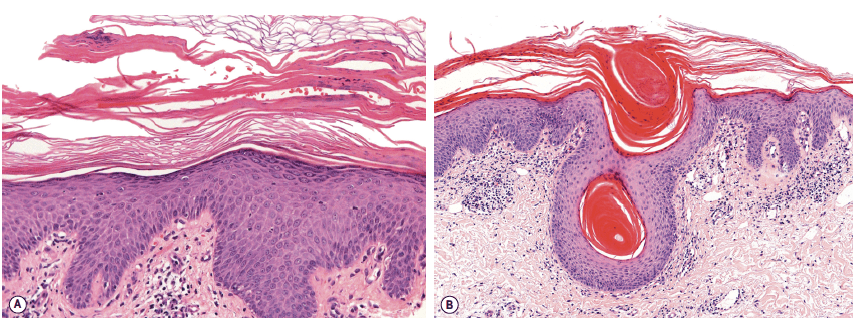
PRP:
Irregular acanthosis resembling psoriasiform dermatitis with irregular hyperkeratosis and alternative vertical and horizontal ortho- and parakeratosis ("checkerboard pattern")
Follicular plugging and shoulder parakeratosis: follicles are dilated and filled with a keratinous plug while the "shoulder" of straum corneum surrounding the follicular opening frequently shows parakeratosis.
Acantholysis and focal acantholytic dyskeratosis in the epidermis. Sparse lymphohistiocytic perivascular infiltrate in the dermis.

400
Name this ocular finding and its associated condition:
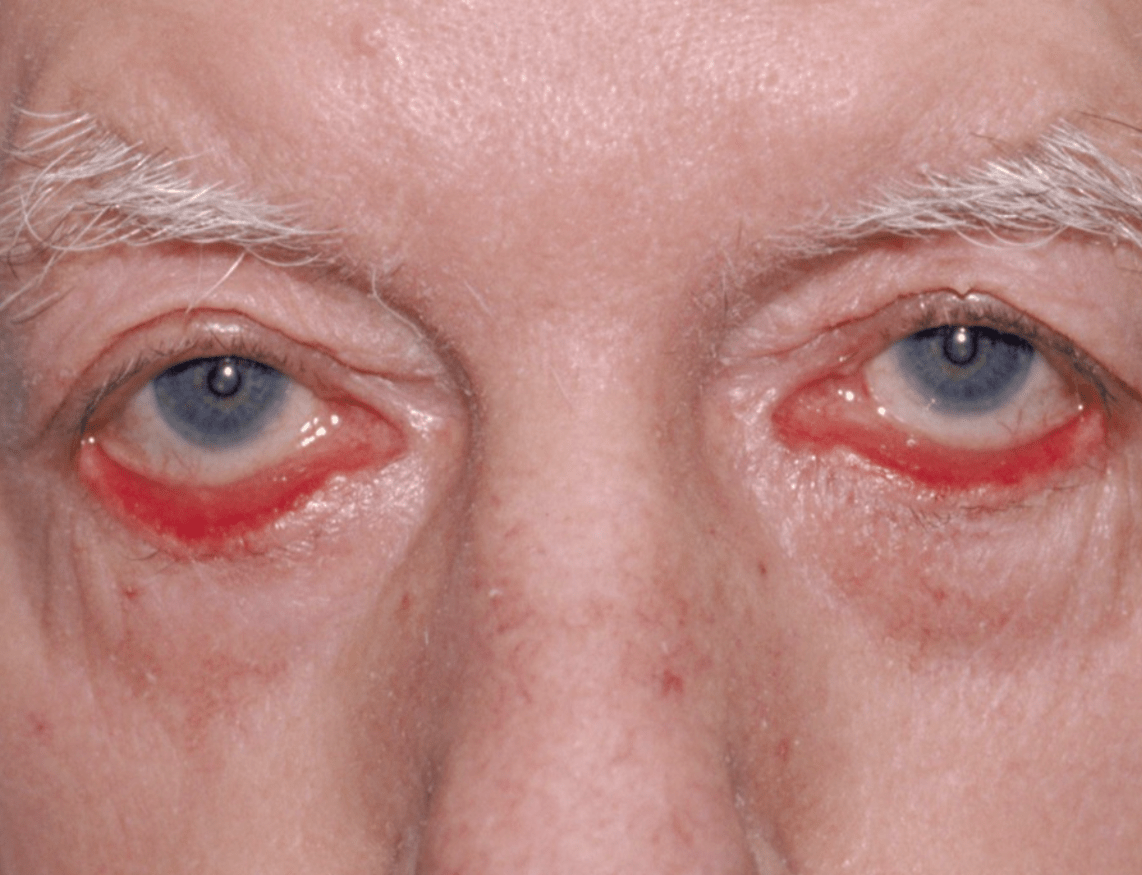
Ectropion - scarring ectropion and ocular dryness are rare ocular findings.
In PRP, ectropion occurs when chronic inflammation and hyperkeratosis around the eyelids lead to scarring and tightening of the skin. This contraction pulls the lower lid outward, and associated ocular dryness can further accentuate the eversion.
500
This patient had erythrodermic psoriasis and then developed this finding. What was the medication?
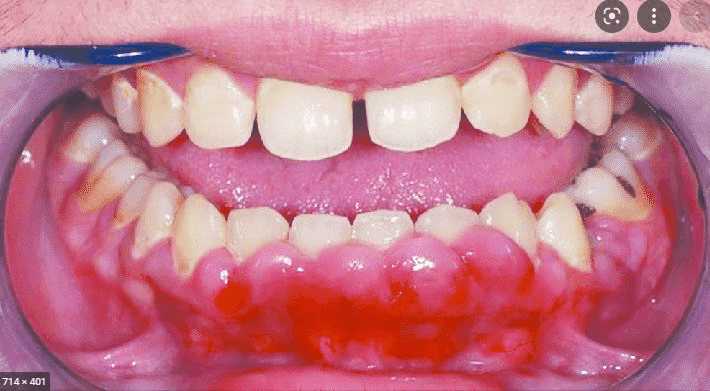
Cyclosporine
-------------------------------------------------
Cyclic undecapeptide isolated from fungus Tolypocladium inflatum
Common SE: nephrotoxicity (reduced GFR, tubular atrophy); risk for renal impairement and HTN increased; increased risk SCCs; GI discomfort, hypertrichosis, paresthesias, gingival hyperplasia, HA, vertigo, muscle cramps, tremor
Metabolic SE: hyperkalemia, hypomagnesemia, hyperuricemia (decr clearance uric acid), hypercholesterolemia and triglyceridemia
500
Name three triggers (i.e. external, infectious, endocrinologic, medication-induced) for psoriasis.
Common triggers:
•Rapid taper of systemic steroids can induce pustular psoriasis & flares of plaque psoriasis
•TNF inhibitors can cause new onset or worsening of psoriasis (including palmoplantar)
•Dupixent for atopic dermatitis may cause psoriasiform lesions (shifting from TH2 --> TH1 response)
500
What is this finding called?

Woronoff's ring:
- Usually sharply demarcated
- Surrounding pale blanching ring around regressing psoriatic lesions.
500
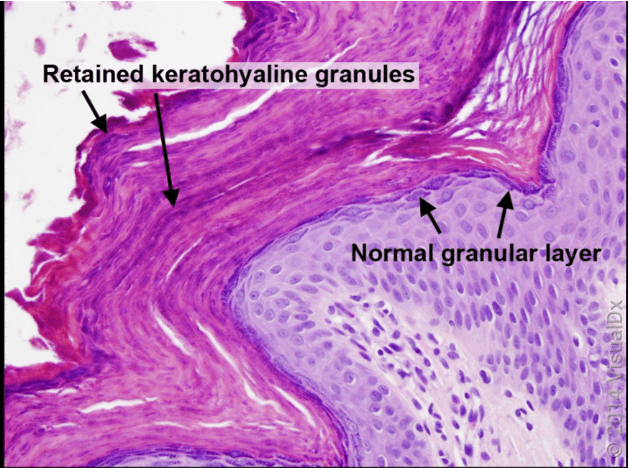
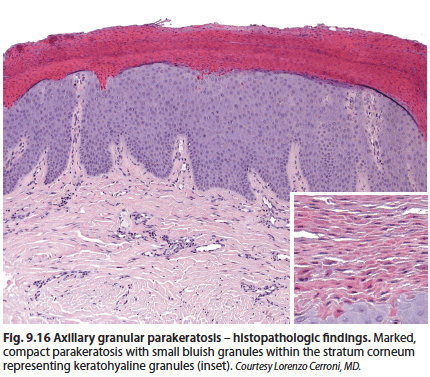
What is this disease?
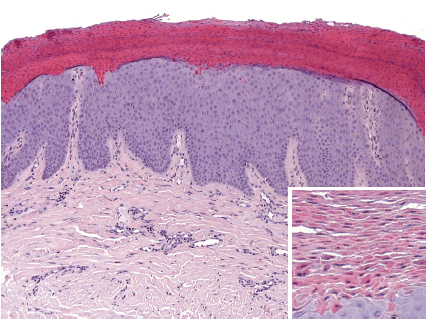
Intertriginous/axillary granular parakeratosis: adult women > infants (diaper area). Characterized by keratotic, brownish red papules, can be conical;, which may coalesce into larger, well demarcated plaques with various degrees of maceration (secondary to local occlusion). Associated with various personal hygiene products (deodorant, antiperspirant), occlusion from diapers (infants), or chemical irritation from benzalkonium chloride (laundry rinse aids).

500
What is this condition? Which subtype specifically?

Type 4 Pityriasis Rubra Pilaris
------------------------------------
"classic" PRP: Follicular hyperkeratosis on an erythematous base resulting in rough papules resulting in "nutmeg grater" appearance on dorsal hands and coalesce to form large salmon-colored to orange-red plaques with "islands" of sparing . Can progress to erythrodermic appearance with varying degrees of exfoliation.
Classification is based on age, duration, and type of cutaneous involvement.
Type I (classic adult): Typically begins on head and neck region that progressively advances caudally. 80% clear within 3 years.
Type II: palmoplantar waxy keratoderma w/ coarse and lamellated scale, more ichthyosiform scaling on lower extremities, occasional alopecia areata; protracted clinical course
III-V: children and adolescents:
Type III: classic juvenile, closely resembles classic adult, clears within 3 years
Type IV (circumscribed juvenile). Most common form in juvenile PRP; only subtype with a focal nature. Circumscribed pink or erythematous follicular papules and scaly plaques on dorsal aspects of the hands, elbows, knees, and Achilles, with palmoplantar keratoderma.
Type V (atypical juvenile): often due to CARD14 gain of function mutations. Similar to type II; palmoplantar keratoderma/sclerodermal-like changes of the hands and feet, and eczematous dermatitis with more ichthyosiform scaly plaques and more chronic course.
CARD-14 associated papulosquamous eruption (CAPE): often have features of both psoriasis and PRP - typically early age of onset and prominent involvement of cheeks, chin, ears, and palms/soles, with chronic course.
Type VI: HIV-associated infection. May respond w/ ART. May resemble PRP type I (coalescing of inflammatory plaques into an erythroderma). May be part of a follicular occlusion tetrad that includes acne conglobata and hidradenitis suppurativa.