EKG
Cardiac Disorders
ACLS
Pharmacology
Complications
100

Patient presents to ER complaining of leg pain x4 days, patient states that he fell while playing basketball and his knee and leg have not stopped hurting since. Upon assessment, you note that patient has edema and ecchymosis to ankle up to mid calf. Knee is tender and swollen. Patient able to move knee and distal pulses are +3. As the triage nurse, how would you proceed with this patient?
ESI 4, patient able to wait in lobby, continue to monitor. Stable to wait
100
56 year old male presents to ER complaining of SOB, chest pain and nausea/vomiting, upon assessment you notate that patient is tripoding and hear crackles upon auscultation to lungs. What cardiac episode could the patient be experiencing?
Left sided heart failure
100
What are your shockable rhythms (defibrillation)?
Ventricular fibrilation
Pulseless Ventricular Tachycardia
MUST SAY PULSELESS VTACH
100
What is the treatment for MI?
MONA = Morphine, Oxygen, Nitro, ASA
100
Untreated strep throat can lead to what kind of heart disease?
Rheumatic heart disease = Endocarditis
200
Patient is BIBA presents to ER found down, unknown last well known time, patient is unresponsive, high quality CPR has been initiated, what is the next step?
Epinephrine administration
200
68 year old male presents to ER complaining of substernal CP x2 days, worsening upon exertion. Pain radiates to jaw, +SOB +nausea -vomiting +dizziness, Upon Assessment, EKG is ordered, Troponin level is elevated. What is happening with this patient? 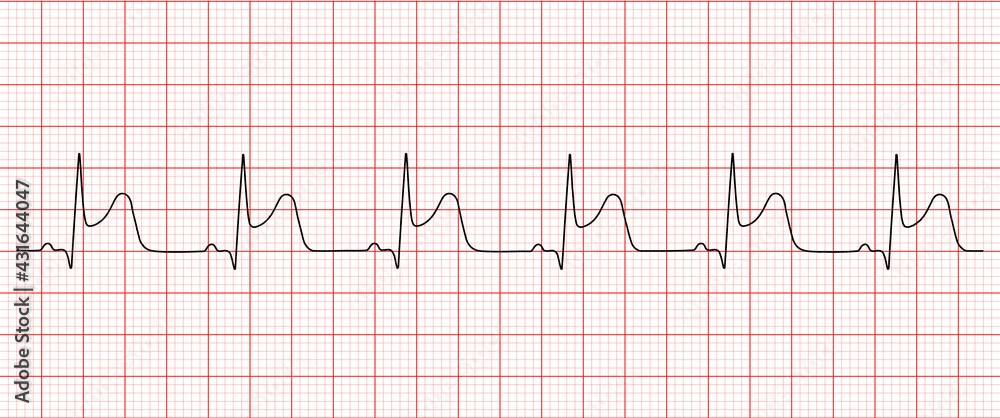
STEMI
200
What type of shock is done for the following rhythms:
Bradycardia
SVT/afib/Vtach with Pulse
Pulseless Vtach/ Vfib
Asystole/PEA
Pacing
Cardioversion
Defibrillation
NONE
200
What are special nursing considerations for Lovastatin?
Hepatotoxic, DO NOT DRINK WITH GRAPEFRUIT JUICE
200
What are the ABC's of heart surgery
Angioplasty - baloon/stent placement
Bypass - CABG
Cutting out fatty block - endodarectomy
300
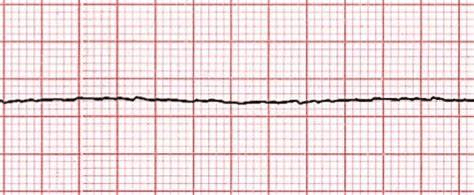
What would be the ACLS algorithm for this rhythm? 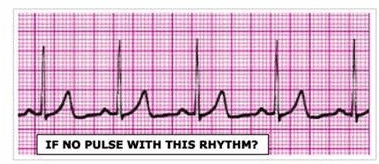
CPR , EPI
NOT SHOCKABLE RHYTHM
300
What position relieves pain for venous stasis ulcers?
300
36 year old male presents to ER pulseless and unresponsive BIBF, unknown medical history, patient was found down, upon assessment patient with GCS 3, pin point pupils, apneic. High quality CPR is initiated. What would be the ACLS algorithm line of treatment?
High quality CPR is initiated. What would be the ACLS algorithm line of treatment?
Narcan
CPR
Epi
Defibrillate
300
What is the action of beta blockers?
lowers heart rate and blood pressure
300
What are the signs/symptoms of lack of oxygenation to limb?
Pain - unrelieved at rest
Paresthesia
Pulses absent
Pallor
Polar
Paralysis
400
What drug/ treatment is used to treat this rhythm? 
Diltiazem - Cardizem
Synchronized Cardioversion
400
What is the difference between stable vs unstable angina?
Stable = relieved with rest, worsening on exertion
Unstable = all the time, unrelieved with rest
400
15 year old male admitted to ICU, patient being treated for DKA has just finished fluid resuscitation, acid base balance has been restored, patient to be downgraded to telemetry when he suddenly becomes pale, diaphoretic, and restless. Patient then suddenly becomes unresponsive. After checking for a pulse, patient is pulseless, 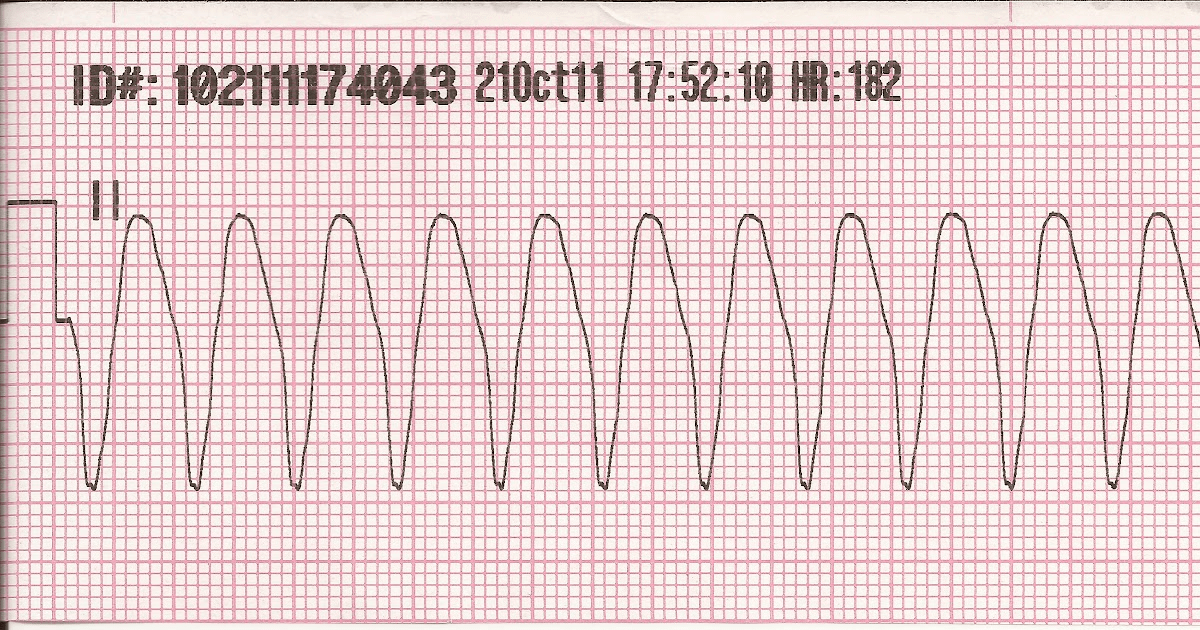 . what is the ACLS algorithm for this patient?
. what is the ACLS algorithm for this patient?
CPR
Check Blood sugar
D50
Epi
Defibrillate - SHOCK
400
What lab values should you monitor when you are warfarin and what is the therapeutic range?
INR 2.5 - 3.5
400
56 year old female presents to ER complaining of chest pain, syncope and difficulty breathing, upon assessment you note muffled heart sounds, hypotension and JVD, Lungs CTAB but showing signs of hypoxia with O2 Saturation at 80%. EKG shows QRS complexes of differing heights. What would be the treatment for this patient?
Pericardiocentesis
Oxygen
500
24 year old male presents to ER s/p methamphetamine abuse, cardiac monitor shows the following rhythm. Patient is alert and oriented, Blood pressure is 110/64. What would be the treatment for this patient? 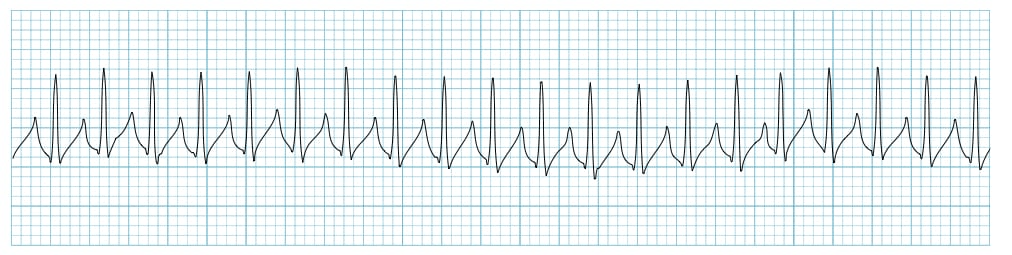
Vagal maneuvers - ice on neck, carotid massage, Valsalva
Adenosine - 6mg - 12mg - 12mg
Synchronized Cardioversion
500
Cold fingers brought on by cold or stress - fingers go from white to blue to red
Raynaud's syndrome
500
patient found down at union station, BIBA after bystanders could not wake him up. The following is on the monitor. Patient has the following vital signs: BP: 0, HR: 0, O2: Unreadable, Temp: 35.2 C, no signs of trauma on patient, what would be the appropriate treatment for this patient? 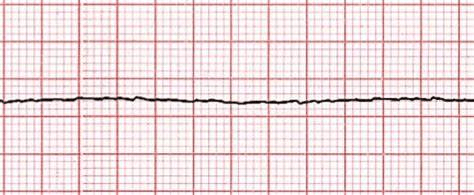
BEHR Hugger
CPR, EPI
Asystole not shockable rhythm
500
What lab values should be monitored when taking heparin or lovenox? and what is the therapeutic range?
PTT: 46-70
500
What safety considerations should be considered for PAD and PVD?
Careful with Hot temperature - impaired sensation
Cautious with foot trauma
AVOID Constriction
No Crossing legs
No constrictive clothing
No cigarettes
No caffeine
No cold temperatures
Shoes well fitted - non sandales
Skin Assessed Daily
Hydration
Toenail trimmed ONLY BY PROVIDER
Limit Standing
600
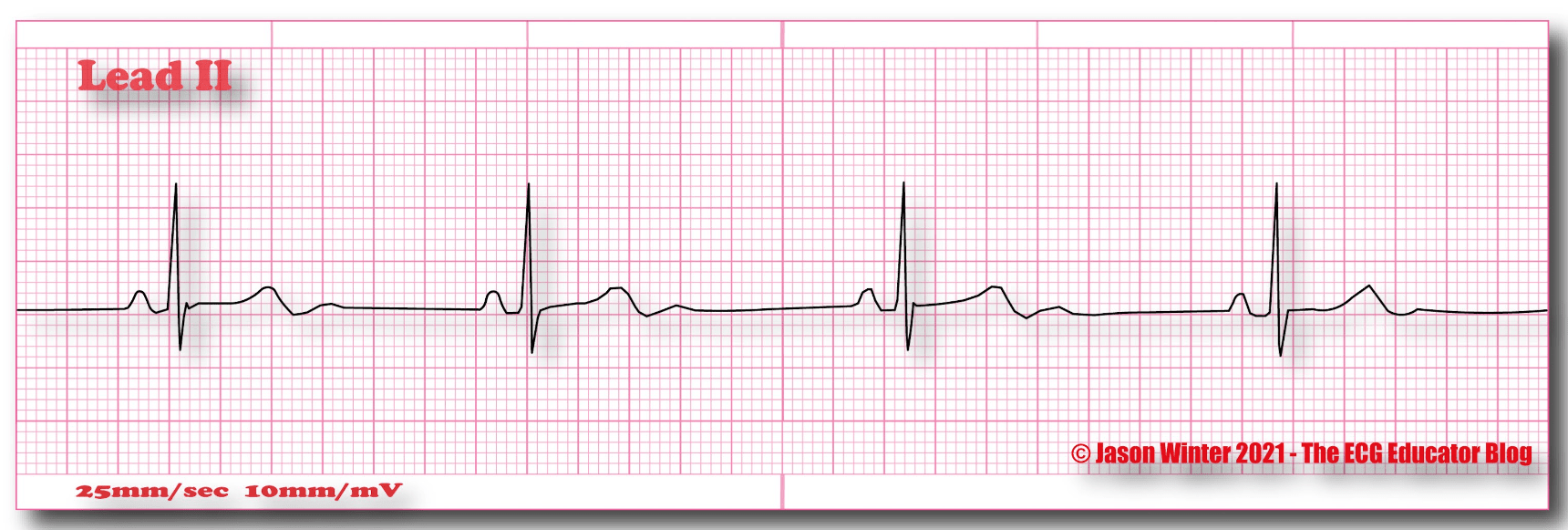
87 year old female presents to ER complaining of syncopal episodes and dizziness upon standing. Patient has dull chest pain with the following rhythm on the monitor. What would be the medication and treatment for this patient?
Atropine
Pacing
600
How should legs be positioned with PVD vs PAD
PVD = Legs elevated
PAD = Legs hanging
600
67 year old male presents to ER complaining of chest pain, SOB, and palpitations, dizziness, patient is pale and diaphoretic. BP 70/45, Temp: 38 C, O2: 84% with the following on the cardiac monitor. What would be the appropriate treatment? 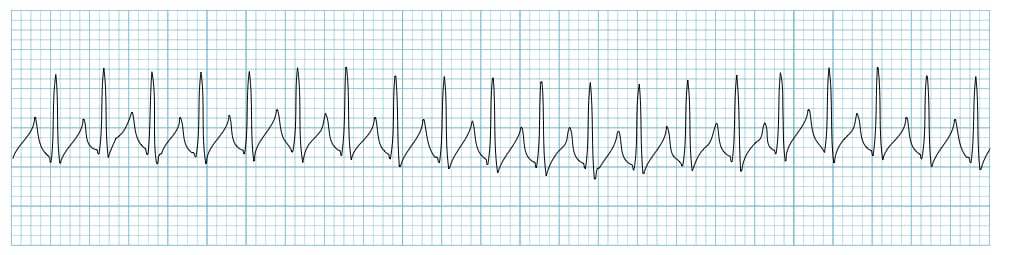
Oxygen
Synchronized Cardioversion
600
What are the vitamins/herbs that should be avoided while taking blood thinners?
Vitamin E, Echinacea, Gingko, Garlic, Ginseng, Omega 3 fish oils
EEGGGO
600
Patient presents to ER complaining of fever/chills, dysuria and hematuria x1 week. Upon assessment patient has the following vitals: BP: 80/40, HR: 154, Temp: 39.2C, O2: 96% RA, abdomen soft, tender to suprapubic area, no rebound, no guarding, no distention +CVA tenderness. What is going on with this patient and how would you anticipate the patient being treated?
UTI = Septic Shock
Fluids
Antibiotics
Pressors if needed
700
Patient presents to ER s/p dialysis, patient became unresponsive and 911 was called. Patient presents with the following rhythm on the monitor. Following ACLS algorithm H's and T's, what would be the treatment for this patient? 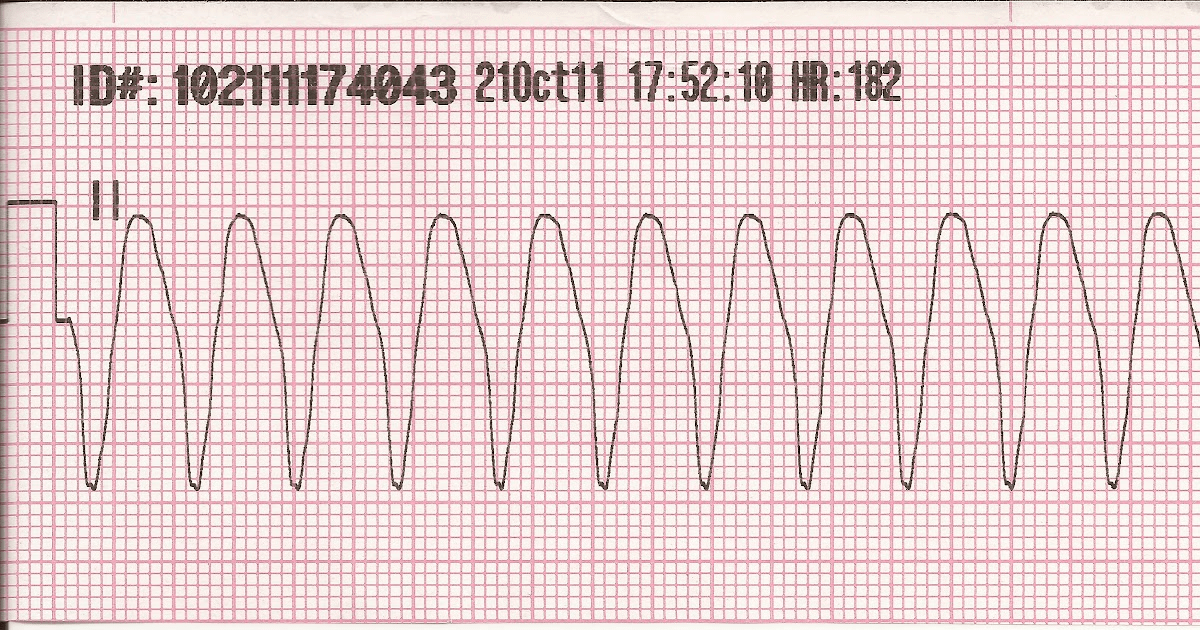
CPR
Epi
defibrillate
Calcium Chloride, Insulin, D50, Bicarb, Lasix
700
What is pulsus paradoxus?
Drop in SBP by 10 resulting in narrowing pulse pressure
700
16 year old male presents to ER with GSW to the back, patient is SOB with unilateral breath sounds, and unable to feel anything below the nipple line. Upon assessment patient shows the following on the cardiac monitor: BP: 65/42, O2: 86%, Temp: 37C, K. 4, Hgb 5, Creatinine 1.2, - what is this patient experiencing and how will we treat him? 
Hemo/Pneumothorax - unilateral breath sounds/penetrating trauma - CHEST TUBE
Hgb 5 = Anemia = BLOOD
O2 85% = OXYGEN / Intubation
Neurogenic shock = Maintain spinal precautions
700
What are the major adverse effects for ACE inhibitors? Lisinopril
angioedema, cough, electrolyte imbalance, Hyponatremia, hyperkalemia
700
Patient presents to ER s/p bee sting, patient has known allergy to bee sting and is now presenting with swelling to face and lips with SOB. patient is tachycardic and hypotensive, what complication is the patient experiencing and how is it treated?
Anaphylactic shock = Epinephrine IM, Steroids - prednisone, Fluids, breathing treatment, vasopressors, Intubation if needed
800
What does this EKG finding indicate? 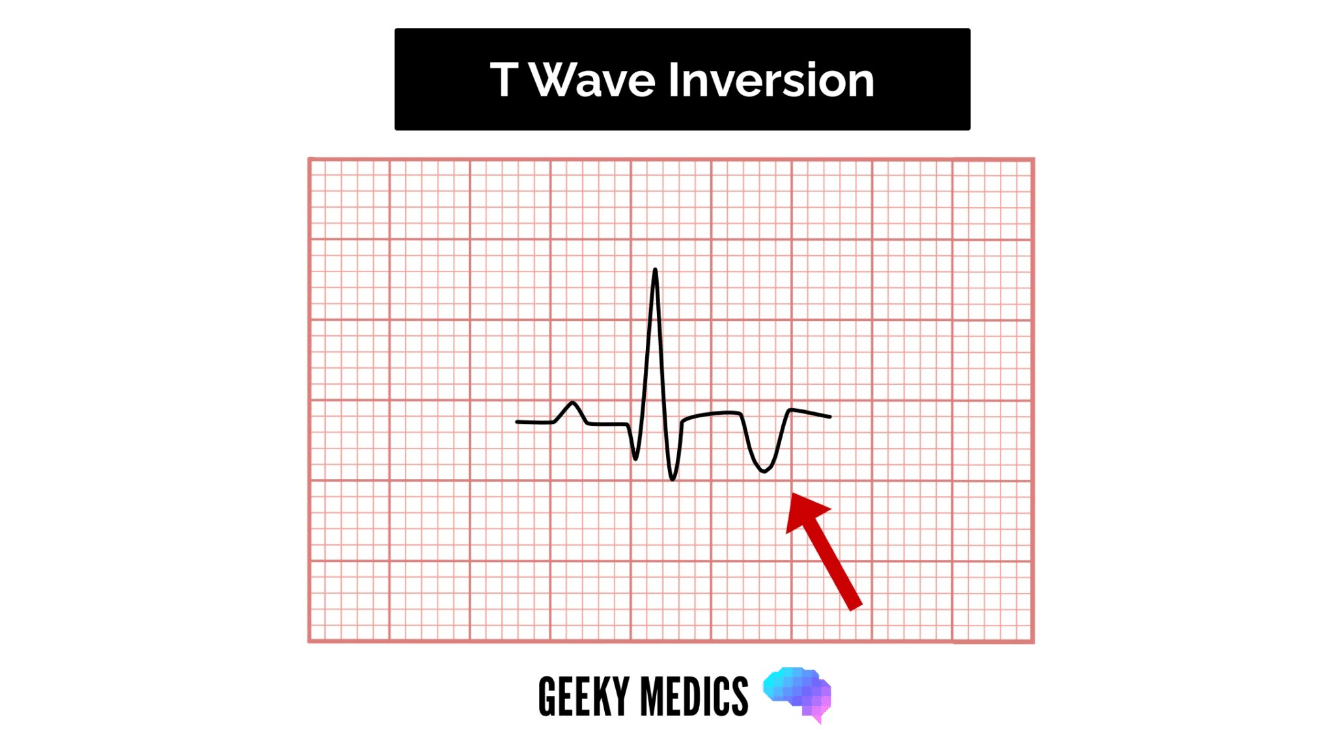
Hypokalemia, Low oxygen
800
58 year old male presents to ER complaining of worsening CP and palpitations, patient with +4 pulses, JVD, and peripheral edema. What cardiac complication could be going on with this patient?
Right sided heart failure - fluid overload
800
Patient presents to ER BIBA RA9, found down at their shelter, LKWT 0300, when patient woke up, they asked members of group home for assistance to the bathroom because she felt "dizzy". No signs of trauma on patient +AV fistula to LUE, appears dirty, unkempt, unable to attain further history on patient. No active bleeding. Patient arrive to room unresponsive to stimuli with shallow respirations at 4 breathing per minute and pinpoint pupils. Respirations are shallow. Skin is pale and cool, no palpable pulse. While high quality CPR is administered, iSTAT is drawn with the following results: NA: 138, K 7, Anion Gap: 28, Glucose: 20, BUN 46, Cr 5.3, Hgb 5 
What would be the ACLS algorithm for this patient?
CPR
EPI
Defibrillate - SHOCK
Fistula = ESRD = Hyperkalemia = Insulin, D50, Albuterol, Lasix, Calcium Chloride, Bicarb
Hgb 5 = Blood
Glucose: 20 = D50
Pinpoint pupils = Drug OD = Narcan
Intubation
800
Name K wasting diuretic and K sparing diuretic
Patient on which medication should avoid potassium rich foods?
Lasix (furosemide)
Spironolactone
Patients on Spironolactone should avoid K rich foods
800
What is normal ejection fraction and what would be considered heart failure?
Normal: 55-70%
Heart failure = <40%
900
60 year old female presents to ER complaining of burning with urination x1 week, states that she feels febrile, nauseated and dizzy. VS: 90/40, HR: 162, O2: 96%, what is this patient experiencing and what would be the treatment?
Septic shock
Antibiotics, fluid resuscitation, vasopressors
900
34 year old male with PMH of methamphetamine and heroin IVDA presents to ER complaining of CP, SOB, fever and chills. upon assessment patient has clubbing to the fingers, petechiae, splinter hemorrhages, osler's nodes, roth spots, janeway lesions, and crackles upon lung auscultation. Temp: 38.4C
What could possibly be going on with this patient?
Endocarditis
900
80 year old male presents to ER complaining of chest pain, and dizziness. Upon assessment patient appears pale and diaphoretic, with ascites, JVD, +3 pitting pedal edema, upon auscultation, heart sounds are muffled. Vital signs: BP 60/30, HR: 158, O2: 72%
What possible condition could this patient be experiencing and what is the treatment?
Cardiac tamponade
Oxygen, Elevate the legs, PERICARDIOCENTESIS, surgery
ANSWER MUST INCLUDE PERICARDIOCENTESIS
900
8 year old male is playing basketball during practice he suddenly collapses and becomes unresponsive, patient has had no history or cardiac symptoms in the past, unknown family history. What could this person possibly be suffering from?
Someone with this known disorder would be on what medical management? Any drug contraindication? What should these patient's be educated to avoid?
Hypertrophic cardiomyopathy
Beta blockers (Metoprolol, atenolol), calcium channel blockers (nifedipine, diltiazem)
AVOID Diuretics, Digoxin, Dilators,
AVOID straining, heavy lifting, sudden position changes, vigorous exercise
900
16 year old male BIBA RA 9 s/p GSW to the back, patient screaming "I CAN'T FEEL MY LEGS!!!!" BP: 80/59, HR: 38, O2: 90%, what is the priority for this patient? What is this patient currently experiencing?
ABC's!
Oxygen, intubate, MAINTAINING SPINAL PRECAUTIONS, atropine, vasopressors, fluids
Neurogenic Shock