RV Sure It's The RV?
Chest Pain
To Tap Or Not To Tap
Valvular Disorders
Phantoms and Pitfalls
100
This "letter" sign can be seen in both volume and pressure overload of the RV
 D-sign
D-sign
100
This "donut-shaped" Echo view at the papillary muscle level is the gold standard for evaluating all three major coronary territories simultaneously
Parasternal Short Axis (PSAX)
100
The inward bowing of the RV during this phase of the cardiac cycle is highly specific for tamponade
Diastole
100
In an IV drug user presenting with fever and hypoxia, you are most likely to find a vegetation on this valve
Tricuspid
100
Failing to place the probe low enough on the patient's chest during an A4C view leads to this common geometric error, which makes the LV look falsely spherical
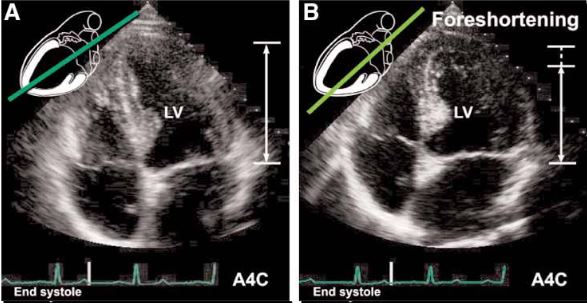 Foreshortening
Foreshortening
200
To differentiate pressure overload (like a PE) from simple volume overload, the D-Sign must be present during this phase of the cardiac cycle
Systole (and Diastole) vs. Diastole alone for volume overload
200
Anterior and Inferior
200
This chamber is usually the very first to collapse (during early systole) when pericardial fluid accumulates
Right Atrium
200
This mechanical complication of an MI typically presents 3 to 5 days post-infarct and is visualized on Echo as turbulent color flow crossing between the ventricles
Ventricular Septal Defect
200
Often mistaken for a massive vegetation, this bright, chunky calcium deposit classically sits at the base of the posterior mitral leaflet
 Mitral Annular Calcification
Mitral Annular Calcification
300
If the RV free wall is >5mm thick it points to this chronic condition
Chronic Pulmonary Hypertension (Cor Pulmonale)
300
You see an inferior wall motion abnormality on Echo. If the aortic root is also dilated, you must assume the dissection flap has sheared off this structure
RCA ostium
300
An Echo finding of >25% resp variation in mitral inflow velocity is the sonographic equivalent of this classic vital-sign abnormality found in tamponade
Pulsus Paradoxus
300
Unlike in chronic MR, the size of this specific cardiac chamber remains completely normal in acute severe MR
Left Atrium
300
This normal, speckled anatomical structure is frequently mistaken for an anterior pericardial effusion, but unlike fluid, it moves with the contracting heart
 Epicardial Fat Pad
Epicardial Fat Pad
400
This specific Echo finding features an akinetic RV mid-free wall with a hyperdynamic, "bouncing" apex, highly suggestive of an acute PE
 McConnell's Sign
McConnell's Sign
400
Anteroseptal and Inferolateral
400
The swinging motion of the heart within a massive pericardial effusion is the cause of this classic EKG finding
Electrical Alternans
400
Three days post STEMI, you see a flail mitral leaflet whipping back into the left atrium, caused by the rupture of this structure
Papillary Muscle
400
An intern frantically calls you about a "massive clot" in the RV, but you recognize this completely normal, thick muscular band that naturally crosses the lower RV cavity
 Moderator Band
Moderator Band
500
This M-mode measurement, taken at the lateral tricuspid annulus, indicates RV systolic dysfunction if <17mm
TAPSE
500
LAD
500
Causing a bloody pericardial effusion, this iatrogenic complication is visualized on Echo as a bright, linear structure completely piercing the RV free wall shortly after device implantation
Pacemaker Lead Perforation
500
A patient with a mechanical mitral valve presents in cardiogenic shock. The leaflets look stuck, but you confirm the diagnosis of stenosis by finding a massively elevated measurement of this parameter
Trans-Valvular Gradient
500
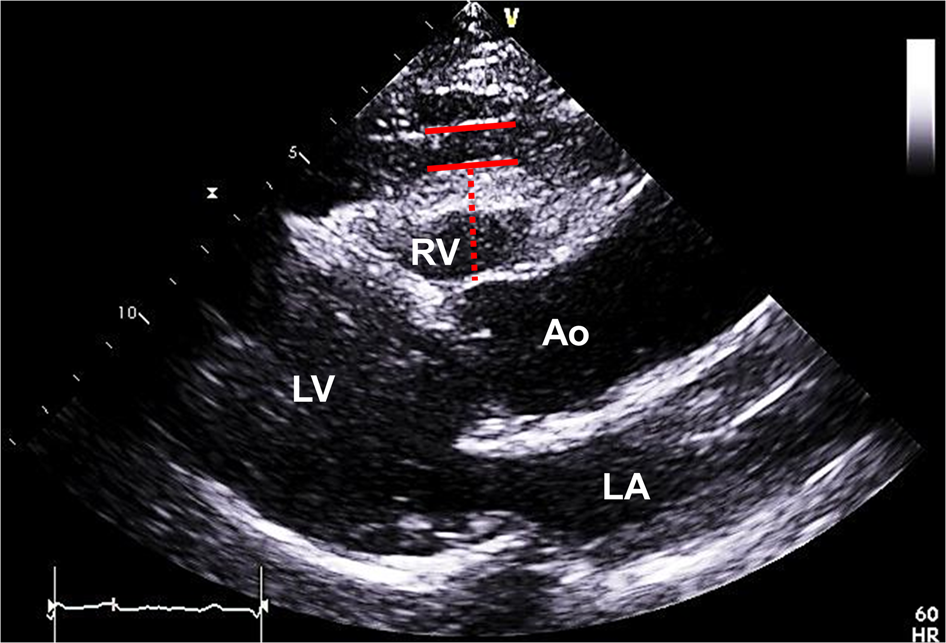
As opposed to a pleural effusion, a pericardial effusion tracks anterior to this circular landmark in the PLAX view
 Descending Aorta
Descending Aorta