EKG
Heart failure
Echo
Name that Trial
Misc and more trials
100
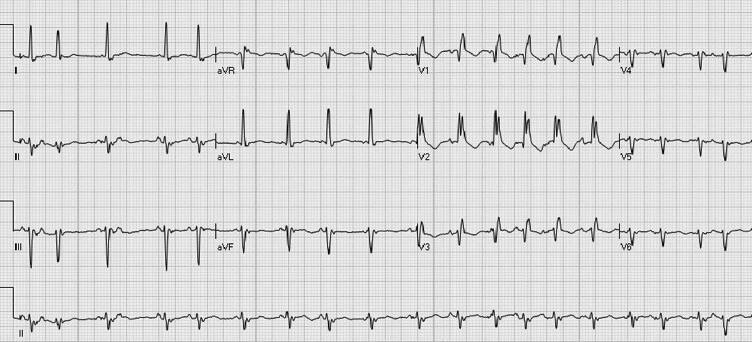
What is the name of the criteria for LVH?
the Sokolow-Lyon index or
the Cornell criteria
100
Name the medication approved for HFpEF and NYHA II and III
SGLT2 2a
ARNI/ARB and MRA 2b
100
Criteria for severe aortic stenosis
Severe aortic stenosis is typically defined by a small valve area (≤1.0 cm2), high peak velocity (>4 m/s), and/or high mean gradient (>40 mm Hg).
100
The trial demonstrated that among patients with LVEF of 35% or less after acute myocardial infarction, a wearable cardioverter-defibrillator did not reduce the incidence of sudden cardiac death but did reduce the secondary outcome of all-cause mortality.
VEST Trial
100
What is the minimal time for washout from ACEI to ARB/ARNI?
36 hours
200
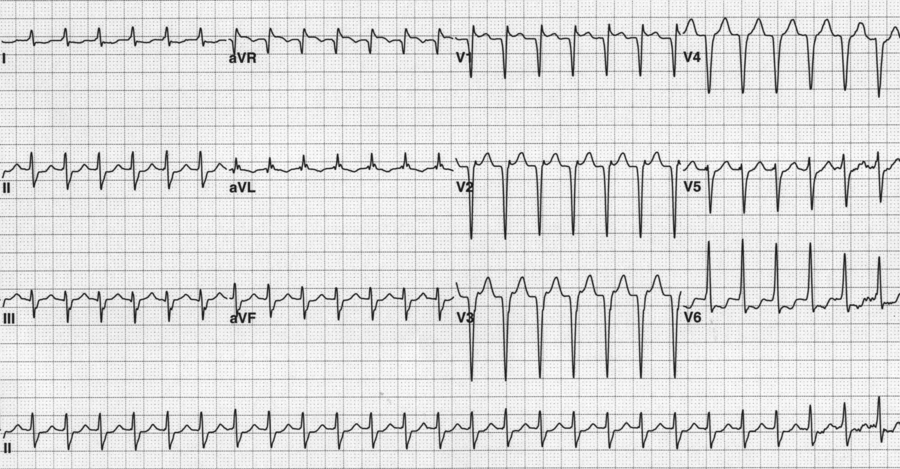
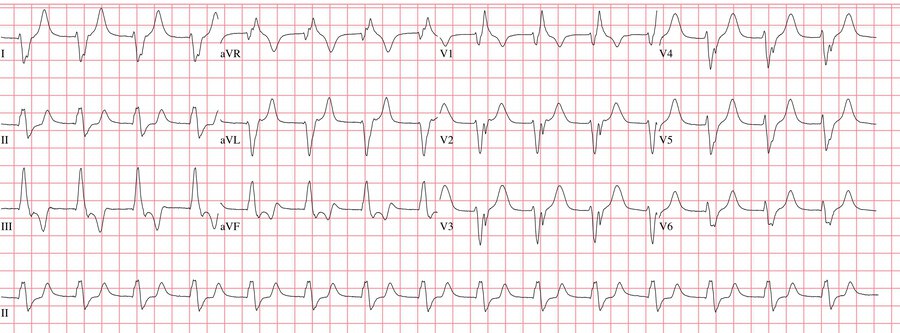
A 63-year-old woman is admitted to the ICU with respiratory failure
Multifocal Atrial tachycardia
200
What is the target dose for SGLT2 therapy in HFrEF?
10 mg QD
200
What view is this?
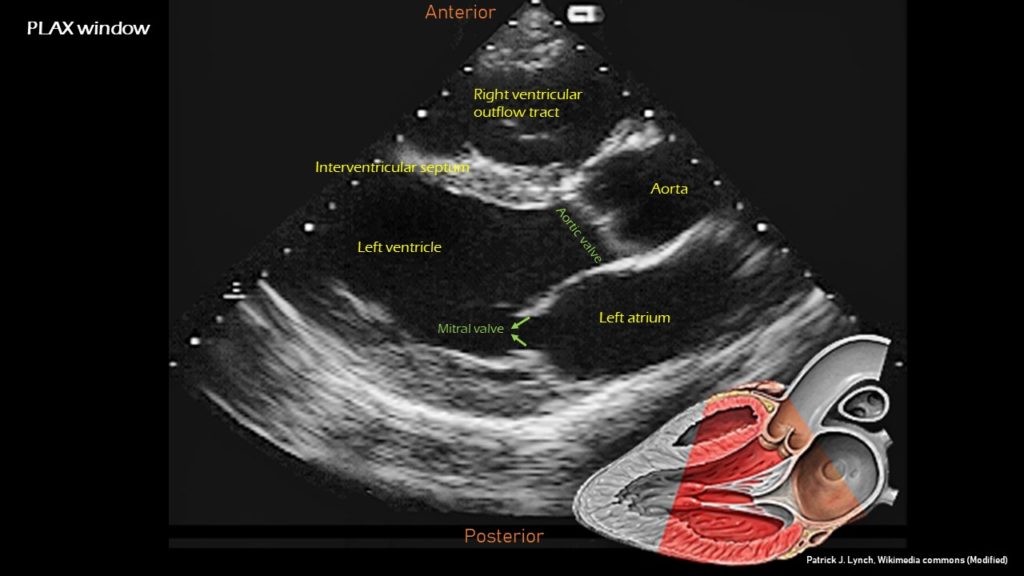
parasternal long axis view
200
trial of spironolactone versus placebo in patients with HFpEF showed no difference in the primary combined end point of death, aborted cardiac arrest, or heart failure hospitalization.
TOPCAT trial
200
What represents a hemodynamic significance in coronary artery stenosis
70% or greater
300
AVNRT
300
Name an alternative for patients intolerant of ARB/ARNI therapy in NYHA II patients
isosorbide dinitrate/hydralazine or bidil
300
What is the echocardiographic equivalent of pulsus paradoxus
Decrease in mitral inflow velocity of more than 25% with inspiration, which is the echocardiographic equivalent of pulsus paradoxus
300
SGLT2 for HFpEF
EMPEROR preserved trial
300
Trial which demonstrated lower CV events and mortality for adults with CV risk (existing clinical or subclinical cardiovascular disease, chronic kidney disease, 10-year Framingham cardiovascular risk score >15%, or age 75 years or older) with intensive BP treatment (SBP target < 120 vs 140)
SPRINT Trial
400
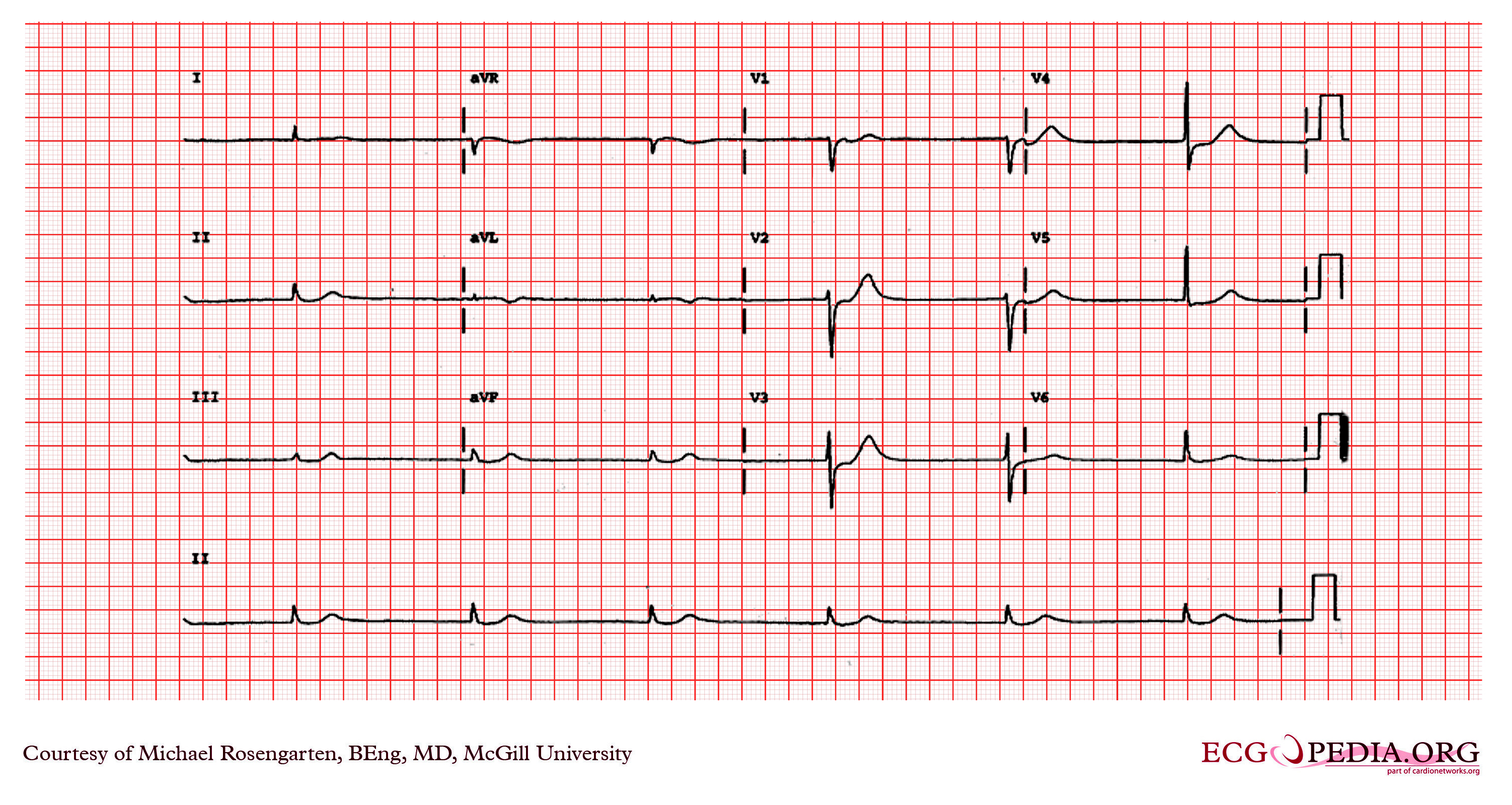
My rate is <40 I am regular, my P wave is inverted before or after the QRS or hidden inside the QRS, my QRS interval is regular. Who am I?
junctional bradycardia
400
Name criteria for CRT placement
LVEF of 35% or less, NYHA functional class II to IV symptoms despite guideline-directed medical therapy, sinus rhythm, and LBBB with a QRS complex of 150 ms or longer
LBBB and a QRS duration of 120 to 149 ms or those without LBBB but with a QRS duration greater than 150 ms, CRT can be useful and should be considered
400
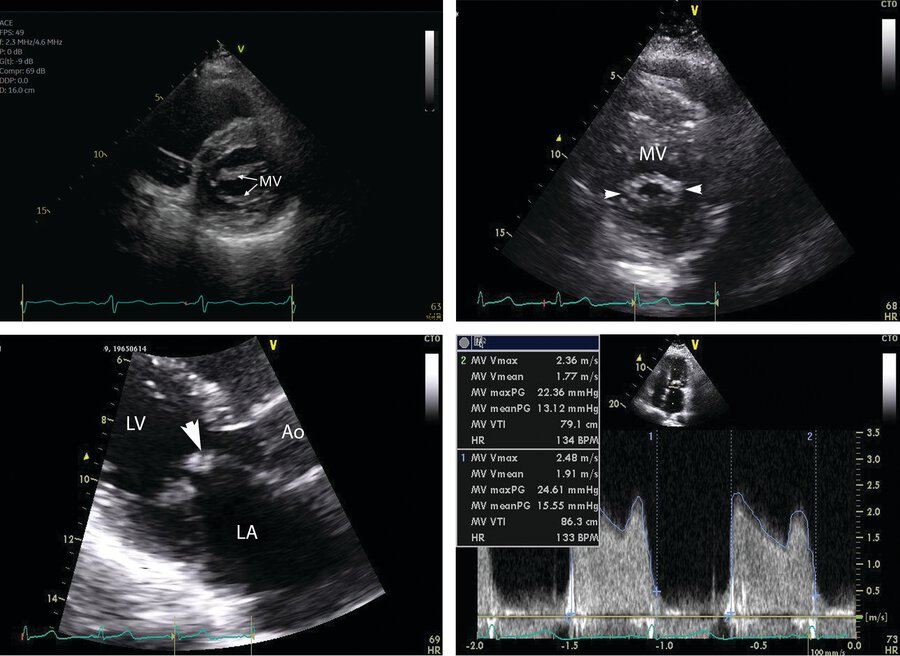
What is the hallmark finding of Rheumatic MS?
In the bottom left panel, diastolic doming (arrowhead) is present with a “hockey stick” deformity from mitral stenosis.
400
The trial in which symptomatic heart failure and LVEF below 40%, valsartan-sacubitril reduced mortality and heart failure hospitalization by 20% compared with enalapril.
PARADIGM-HF trial
400
What is the mechanism of action of ezetimibe?
It blocks the critical mediator of cholesterol absorption, the Niemann-Pick C1-like 1 (NPC1L1) protein. This inhibits the absorption of cholesterol on the intestinal brush border
500
escape rhythm arising from the ventricular myocardium. The QRS complexes are wide (as in all ventricular arrhythmias) and fairly regular. An idioventricular rhythm is typically at a rate between 30/min and 40/min but is considered accelerated when the rate is more than 50/min but less than 100/min. this occurs after reperfusion
500
What year was the 1st beta blocker discovered? bonus for naming which one was discovered
1964 and propanolol by Sir James Black
500
What are the criteria for severe aortic regurgitation?
Defined by the jet width that occupies 65% or more of the LV outflow tract, vena contracta (the width of the regurgitant jet at its most narrow portion) greater than 0.6 cm, holo diastolic flow in the descending aorta, regurgitation volume of 60 mL or more, and effective regurgitant orifice area of 0.3 cm2 or greater.
500
Trial evaluating PCI (with BMS) vs. medical therapy in stable CAD
-No difference in composite of all-cause mortality and non-fatal MI
-No difference in ACS hospitalization
COURAGE Trial
500
This trial compared medical therapy alone with medical therapy plus CABG in patients with coronary artery disease and left ventricular dysfunction.The rates of death from cardiovascular causes and of death from any cause or hospitalization for cardiac causes were lower among patients assigned to CABG than among those assigned to medical therapy.
STICH Trial