Airway & Breathing
Tubes in the Chest
The Pericardium
The Aorta
The Right Heart Can't Take a Joke
100
A patient on mechanical ventilation suddenly develops hypotension, tachycardia, absent breath sounds on the left, and tracheal deviation to the right. What are your next steps?
1. Disconnect the ventilator
2. Needle decompression (or finger thoracostomy) of the left chest.
100
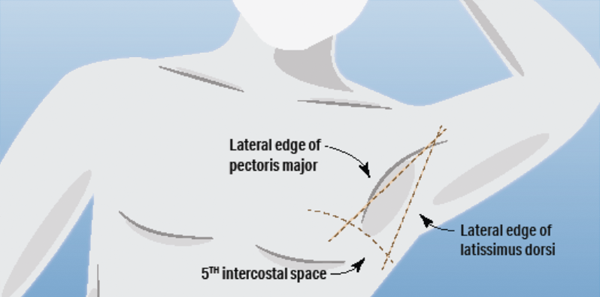
What is the recommended anatomical site for lateral chest tube insertion in traumatic pneumothorax?
The 4th–5th intercostal space at the anterior or mid-axillary line (triangle of safety).
100
On bedside echo, what is the MOST SPECIFIC echocardiographic sign of cardiac tamponade?
Diastolic right ventricular free wall collapse.
100
In the Stanford classification, what defines a Type A dissection, and why does it matter?
Any dissection involving the ascending aorta — regardless of where the intimal tear originates. It requires emergency surgical repair.
100
Name three ECG findings associated with right heart strain in acute PE that are independent predictors of hemodynamic collapse or death.
(1) Sinus tachycardia (HR >100),
(2) S1Q3T3
(3) Complete right bundle branch block
(4) T-wave inversions in V1–V4
(5) ST elevation in aVR
(6) Atrial fibrillation.
200
In massive hemoptysis, what position should you patient be placed into?
Bleeding lung down — to prevent blood from flooding the unaffected lung.
200
After chest tube placement for hemothorax, what two output thresholds indicate the need for operative thoracotomy?
>1,500 mL initial output OR >200 mL/hour for 3 consecutive hours.
200
A patient presents with pleuritic chest pain, low-grade fever, and a friction rub. ECG shows diffuse concave-up ST elevation. Name the four classic stages of ECG evolution in acute pericarditis.
Stage 1: Diffuse ST elevation with PR depression.
Stage 2: Normalization of ST segments with flattening of T waves.
Stage 3: Diffuse T-wave inversions.
Stage 4: Normalization of T waves (return to baseline).
200
On CXR, the "calcium sign" — separation of intimal calcification from the outer aortic wall by more than what distance — is suggestive of aortic dissection?
Greater than 5 mm.
200
On bedside echo, a patient with massive PE shows RV dilation with akinesis of the mid-free wall but preserved contractility of the RV apex. What is this sign called, and why does the apex move normally?
McConnell sign. The apex is tethered to the left ventricle and receives traction from LV contraction, so it continues to move even when the RV free wall fails.
300
In massive hemoptysis requiring intubation, why is a single-lumen ETT preferred over a double-lumen tube — and which mainstem bronchus should it be advanced into?
Single-lumen allows a larger internal diameter for bronchoscopic suctioning of clots.
It is advanced into the non-bleeding mainstem bronchus to isolate and protect the good lung.
300
A patient has a retained hemothorax >300 mL persisting after chest tube placement. What procedure should be performed within 72 hours — and why is a second chest tube NOT the answer?
VATS (video-assisted thoracoscopic surgery). A second chest tube has high failure rates for retained hemothorax and delays definitive evacuation, increasing the risk of empyema and fibrothorax.
300
A patient with a large pericardial effusion undergoes successful pericardiocentesis with 1,200 mL drained and initial hemodynamic improvement. Three hours later, they develop acute hypotension and pulmonary edema. What is this complication and what causes it?
Pericardial decompression syndrome — caused by sudden increase in venous return to a chronically underfilled and deconditioned heart.
300
A patient presents with acute tearing chest pain radiating to the back, BP 210/110, and a new diastolic murmur heard best at the right sternal border. CT angiography confirms a Type A dissection with aortic root involvement. What is the murmur and why is this a surgical emergency (aside from just being a Type A dissection)?
The murmur is acute aortic regurgitation — caused by the dissection flap disrupting the aortic valve commisural support (where the cusps attach to the aorta) or by dilating the aortic root.
This is a surgical emergency because acute severe AR causes rapid LV volume overload and cardiogenic shock, unlike chronic AR where the LV has time to compensate.
300
In a patient with obstructive shock from massive PE, what is the dose of alteplase — and how does the dosing change if the patient is in cardiac arrest?
100 mg infused over 2 hours for non-arrest. In cardiac arrest, 50 mg IV bolus (with consideration of a second 50 mg bolus). CPR should continue for at least 15 minutes after administration before considering termination.
400
An open pneumothorax is initially managed with a three-sided occlusive dressing. The patient subsequently develops worsening hypotension and respiratory distress despite the dressing. What are the next steps?
Lift or remove the dressing to relieve a developing tension pneumothorax, then proceed to tube thoracostomy.
400
A patient with a right lower chest stab wound has a chest tube placed that initially drains 400 mL. Output then slows — but over the next several hours, the chest tube begins draining persistently again. What occult injury should be suspected?
Diaphragmatic injury with underlying liver laceration — the chest tube suction pulls blood from the injured liver through the diaphragmatic defect into the pleural space, creating a persistent or recurrent hemothorax.
400
In acute Type A aortic dissection complicated by hemopericardium and tamponade, why is full pericardiocentesis generally avoided, and what is the recommended approach?
Full drainage may precipitate recurrent aortic hemorrhage by removing the tamponade effect that is limiting the bleeding. The recommended approach is limited pericardiocentesis — drain only enough to restore hemodynamic stability as a bridge to the OR.
400
Per ACC/AHA guidelines, what are the initial heart rate and systolic blood pressure targets for medical management of all acute aortic syndromes, and what is the first-line drug class?
HR <60 bpm, SBP 100–120 mmHg, using IV beta-blockers as first-line agents.
400
A patient with confirmed PE is hypotensive on norepinephrine at 20 mcg/min. Per the 2026 AHA/ACC PE guidelines, why is escalating norepinephrine above 15 mcg/min problematic, and what agent should be added instead?
Above 15 mcg/min, norepinephrine begins to increase pulmonary vascular resistance — worsening RV afterload. Add vasopressin.
Dobutamine (up to 10 mcg/kg/min) can also be added as an inotrope to augment cardiac output.
500
What is the definitive treatment of choice for massive or refractory hemoptysis?
Bronchial artery embolization. The bronchial arteries are the source in ~90% of cases.
500
After chest tube placement for a large pneumothorax that has been present for >3 days, the patient develops acute hypoxia, cough, and new unilateral infiltrates on the ipsilateral side. What is this complication?
Re-expansion pulmonary edema (REPE).
Prolonged lung collapse causes increased capillary permeability; rapid re-expansion then allows protein-rich fluid to flood the alveoli.
Risk factors include collapse >3 days and rapid/complete drainage. Management is supportive — supplemental oxygen, HFNC or CPAP, and in severe cases mechanical ventilation. Prevention involves controlled, gradual re-expansion rather than immediate wall suction.
500
A patient presents with chest pain and diffuse ST elevation. What pattern should make you reconsider pericarditis and consider STEMI instead?
ST elevation in lead III greater than lead II.
This has an odds ratio of 21 for STEMI over pericarditis — it localizes to the inferior territory (right coronary artery), which produces greater ST elevation in III than II due to the axis of lead III.
500
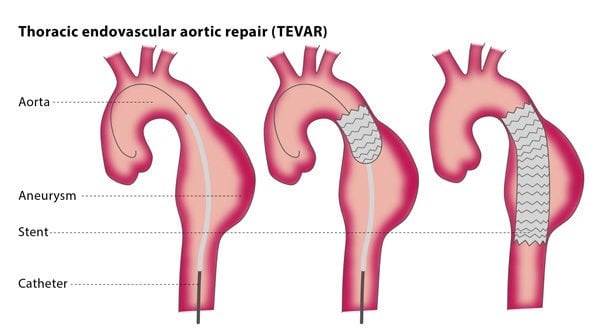
Name three specific complications of acute Type B aortic dissection that change management from medical therapy to procedural intervention and what is the preferred intervention.
(1) Rupture
(2) malperfusion (visceral, renal, or limb ischemia)
(3) refractory pain or HTN despite maximal medical therapy.
The preferred intervention is TEVAR.
500
A patient with massive PE and RV failure needs intubation. After induction, the patient immediately arrests. What is the physiologic mechanism of peri-intubation arrest in acute RV failure, and what specific meds and ventilator strategy should be used if intubation is unavoidable?
(1) sedation abolishes the sympathetic surge maintaining SVR and (2) PPV reduces RV preload and increases RV afterload
Use low TV, low PEEP; avoid hypercapnia via increased RR, and high FiO2 for pulmonary vasodilation.
Ketamine is preferred for hypotensive patients. Etomidate can be used for normotensive patients to avoid HR and BP spikes.