Cases
Med/Psych
Cross Overs and Interactions
Randomly Random
Interesting Organisms
200
A 23-year-old man presents to the clinic with recurrent disturbing dreams, insomnia, and inability to concentrate from the past 35 days. He states that he has been disturbed since he has been told about the relapse of his acute myeloid leukemia. He says that he is unable to forget the moment when the physician explained to him about his condition. Throughout his previous chemotherapy sessions, he suffered from similar symptoms and took cognitive behavioral therapy. He says that he has been having nightmares in which “he sees strange tumor cells popping out of his body.” The nightmares have been causing him to lose sleep at night. He further states that he has been avoiding coming to the clinic because of anxiety-inducing thoughts that he gets related to his condition whenever he sees a hospital. On mental status examination, the patient looks anxious and restless, but there is no sign of depression. There is no prior psychiatric history. This is the best pharmacological treatment option for this patient:
A. Selegiline
B. Buspirone
C. Sertraline
D. Trazodone
E. Phenelzine
What is sertraline, first line for PTSD?
200
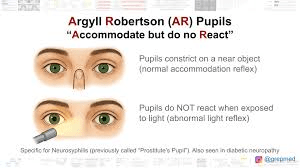
This presents insidiously and variably, at an average age of 52-53 in the US, with memory loss, mood changes, psychosis, seizures, and cognitive changes. Irritability, depression, anxiety, apathy, and agitation are common.
'Clinical features include progressive cognitive impairment (dementia), significant personality changes (apathy or giddiness), mood disturbances, delusions, hallucinations, and speech or writing issues.
Physical signs include tremors, slurred speech, poor handwriting, and, in advanced stages, muscle weakness or paralysis.'
What is tertiary/neurosyphilis ie GENERAL PARESIS OF THE INSANE?
The Mnemonic is PARESIS:
Personality
A ffect
R eflexes (hyperactive)
E ye (eg, Argyll Robertson pupils)
S ensorium (eg, illusions, delusions, hallucinations)
I ntellect (eg, decreased recent memory, orientation, calculations, judgment, insight)
S peech
The CSF is characterized by lymphocytic pleocytosis, elevation of protein levels, elevation of immunoglobulin G index, and reactive VDRL test result. Check the serum fluorescent treponemal antibody absorption (FTA-ABS) test.
Treatment includes penicillin, which is efficacious when administered earlier in the course of the disease. Often a poor prognosis.
200
Number of weeks recommended for a fluoxetine wash-out.
What is 5?
200
This QTc is considered prolonged in men.
What is 450ms?
200
These living fossils have been around for about 250 million years and similar looking fossils may take that back to ~450 million years. Some live on the east coast. They have a blue, copper based blood used medically to test substances for bacterial contamination.


400
A 55-year-old man presents to the clinic complaining of difficulty sleeping at night, and the inability to maintain an erection. He was diagnosed with renal cell carcinoma 9 months ago. He says that since the diagnosis, he has not had a peaceful night's sleep. He usually lays awake, thinking about what will become of his family. He says that this "tension" does not let him concentrate on anything. He feels tense most of the days and does not meet anyone. Current workup of the patient shows the tumor to have shrunk in size. He drinks one can of beer daily. He appears anxious. In addition to psychotherapy, which of the given pharmacotherapy will be best for this patient?
A. Buspirone
B. Escitalopram
C. Propranolol
D. Valerian
E. Amitriptyline
What is A, buspirone?
This is an example of monotherpay GAD treatment with this medication, chosen here for its relative lack of sexual side effects.
400
Ms. A was a 67-year-old female with a medical history significant for hypertension, controlled diabetes, chronic obstructive pulmonary disease, and a diagnosis of late-onset schizophrenia who presented to inpatient psychiatry under a temporary detention order because she was displaying bizarre behavior and responding to internal stimuli. She also appeared to be quite paranoid, carrying knives around with her for protection. Her symptoms were first noticed 8 years before, and she had been admitted to an outside psychiatric facility seven times over the past 2 years with a similar presentation. Ms. A was diagnosed with late-onset schizophrenia and had been treated with risperidone, haloperidol, and paliperidone. Her symptoms only minimally improved with antipsychotic treatment each time, and she had a history of noncompliance with medication in the outpatient setting, because she did not believe she had a psychiatric illness. Over 8 years, Ms. A's symptoms continued to worsen to the point where she could no longer maintain employment. She retired at age 62 and moved in with family members. This is NOT schizophrenia. Taking this history earlier would have lead to an earlier correct diagnosis:
A. Her vaccination history.
B. Travel history, especially to SE Asia.
C. Her sexual health history.
D. Her family history.
E. History of "Up Your Gas" use.
What is her sexual health history?
This is a real case, finally diagnosed at neurosyphilis.
400
The antidepressant without significant activity at CYP2D6:
A. Bupropion
B. Fluoxetine
C. Sertraline
D. Paroxetine
E. Duloxetine
What is C, sertraline.
400
This QTc is considered prolonged in women.
What is 470ms?
400
This hodge-podge of mostly unicellular, eukaryotic organisms is no longer considered a separate kingdom, but divided up into other taxonomic clades.
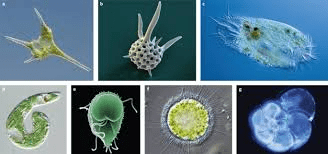

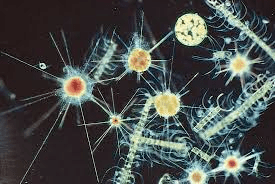
What are the protists?

600
A 28-year-old man presents to the clinic complaining of a one-year history of chronic back pain. He explains that the pain started after getting a job at a logistics company. He does not recall any trauma and does not have morning stiffness or neurological symptoms. He has been seen by 2 other physicians for his back pain who did not establish a diagnosis. The patient also has abdominal bloating and a feeling of constipation that started 3 weeks ago. After doing extensive research on the internet, he is concerned that the symptoms might be caused by pancreatic cancer. He would like to undergo a CT scan of his abdomen for reassurance. He has a history of episodic chest pain, for which he underwent medical evaluation with another healthcare provider. Tests showed no pathological results. He does not smoke or drink alcohol. He reports that he is under significant pressure from his superior due to frequent performance evaluations. He takes multivitamins and glucosamine to prevent arthritis. His vital signs are within normal limits. Examination shows a soft, non-tender, non-distended abdomen and mild bilateral paraspinal muscle tenderness. The remainder of the examination, including a neurological examination, shows no abnormalities. Lab report is normal. X-ray of the spine is normal. This is the most likely explanation for this patient’s symptoms:
A. Illness anxiety disorder
B. Irritable bowel syndrome
C. Conversion disorder
D. Somatic symptom disorder
E. Acute stress disorder
What is D, somatic symptom disorder?
This patient's presentation is most consistent with somatic symptom disorder. Individuals with this disorder show a preoccupation with their health and develop significant distress and fear of severe illness over benign symptoms. This patient's diagnostic workup did not reveal any known medical etiology of his chronic back pain. In patients with somatic symptom disorder, anxiety typically persists despite reassurance by health care professionals and often leads to patients pursuing extensive diagnostic testing, undergoing unnecessary medical procedures, and frequently changing physicians. Illness anxiety disorder is diagnosed in individuals with a persistent fear of having or developing an illness despite having no physical symptoms. Patients also often show maladaptive behavior, such as changing physicians on a regular basis. While this patient has some features of this disorder, his anxiety is caused by physical symptoms, which is not a feature of illness anxiety disorder.
600
This is the most common CNS tumor in adults, affecting a median age of 66 and females at a rate of 2-3/1. Slow growin. They are important in psychiatry for the various psychiatric symptoms associated with them. They prefer growing on the convexity (Often the frontal lobe) and parasagittally. They can create changes in personality ranging from apathy to disinhibition, depression, and in those growing in deeper areas, psychosis. Seen below:
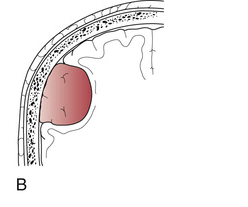
A. Itsa meatball!
B. Meningioma.
C. Neurocystercosis.
D. Liver met.
E. Medulloblastoma
F. Glioblastoma.
What is B, meningioma?
Get brain imaging, especially if you get an odd presentation with soft neurological signs.
600
When starting this ASD mood stabilizer on a patient taking VPA, you need to cut the dose by 50% or more and slow the titration. It has a different titration pack for this scenario.
What is lamotrigine?
600
True or false: You should repeat an EKG when increasing the dose of a QTc prolonging medication by 30-50%
What is true? According to a presentation via MGH. Otherwise, start the med and repeat the EKG in 2-4 weeks
600
Turritopsis dohrnii, a species of jelly fish can revert its mature medusa form into an immature polyp during adverse conditions, rendering is basically biologically _ _ _ _ _ _ _ _. Some species of hydra and flat worm share similar traits.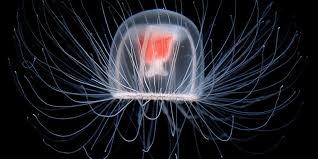
What is immortal?
This small, ocean-dwelling species can revert to its polyp (juvenile) stage from a mature, medusa stage when threatened or damaged, allowing it to avoid death indefinitely.
Hydras can regenerate from populations of pluripotent stem cells they keep their whole lives. Flat worms can regenerate individuals even when cut into small pieces, like Deadpool or Wolverine.


800
A 54F is admitted for the treatment of cancer with chemotherapy after being diagnosed 3 weeks ago. She has been has been more irritable, responds to her husband monosyllabically at times, and is unmotivated to do daily activities. She states she "Lost it" when asked about some agitation/irritability reported earlier today by the nursing staff. The patient has severe, incapacitating nausea and has vomited several times. She reports this as the most distressing symptom. Your initial recommendation:
A. Mirtazapine 15mg PO qHS.
B. Olanzapine 2.5mg PO/IM q4 PRN.
C. Haloperidol 3mg PO/IM q4 PRN.
D. Ondansetron 8mg SL BID.
E. Lorazepam 1mg PO/IM PRN.
What is B, olanzapine PRN?
Useful for severe vomiting, and for the mild agitation/irritability. Mirtazapine is also useful iso CTX related n/v, but less acutely useful here. She may end up needing it...There may be some depressive symptoms brewing.
800
A 65-year-old African American female with a medical history of HIV on active anti-retroviral therapy, HCV with completed antiviral treatment, and hyperlipidemia was admitted to the hospital due to psychotic symptoms lasting for one week. Over the past five months, she exhibited paranoid behavior, including auditory and visual hallucinations, expressing a belief that someone else was speaking for her. Physical examination revealed fearful behavior, with the patient pointing to and addressing an imaginary person. There were no neurological deficits. Initial brain imaging was unremarkable, and her chronic leukopenia remained static at a CD4 count of 294. EEG and CSF analyses only revealed positive West Nile Virus IgG. Despite treatment with risperidone and later aripiprazole, her symptoms persisted, prompting consideration of autoimmune encephalitis. However, a 5-day pulse steroid therapy in the third week of hospitalization showed temporary improvement before relapsing post-treatment. Subsequent plasmapheresis sessions in the intensive care unit led to increased communication and neurological engagement. These are some early history questions you can ask to isolate the diagnosis:
What are you can ask about fatigue, rashes, prior/recurrent fever, joint pain and swelling, alopecia, headaches, cognitive issues prior, Raynauld's, etc.??
This is SLE.
The most common neuropsychiatric manifestations in SLE are cognitive deficit (49.33%), lupus headache (23.11%; in 57.69% of these patients, tension-type), psychoses (12.00%), seizures (10.67%), and cerebrovascular events (9.78%).
800
When cross tapering a patient on to clozapine, it is recommended to start cutting that meds dose once you reach a clozapine dose of _ _ _ to _ _ _mg.
What is 100 to 200mg?
800
"These nutrient deficiencies lead to atrophic glossitis, where the tongue loses its papillae, becomes smooth, and swells. It is often described as a "beefy red" or sore tongue, sometimes appearing with scalloped edges."
What are B9, B12, or iron deficiencies?
800
Caulerpa taxifolia, a species of green _ _ _ _ _ can grow to ~12 inches and is considered the largest single celled organism.

What is a green algae?
1000
A 35-year-old man presents to the clinic with a 4-month history of a productive, occasionally blood-tinged cough. He consumes two bottles of beer daily and has a 20-pack-year smoking history. He works as a car mechanic. A chest X-ray reveals a centrally located opacity in the right middle lobe. As part of further evaluation, he is scheduled for an MRI scan. Upon entering the MRI machine, he begins screaming and appears extremely distressed. He is immediately removed from the scanner. He later reports experiencing similar episodes since childhood, particularly in elevators, buses, and grocery stores, all of which he actively avoids. He states that he rarely leaves his house due to a fear of having another “attack.” He was visibly anxious before the MRI, expressing concern about becoming trapped. This is the most likely diagnosis?
A. Claustrophobia
B. Tomophobia
C. Agoraphobia
D. Social anxiety disorder
E. Panic disorder
F. Bro, chill.
What is C, agoraphobia?
Agoraphobia is correct because the patient exhibits a marked fear or anxiety about situations where escape may be difficult or help unavailable in the event of panic-like symptoms. This includes enclosed places (MRI scanner, elevators), public transportation (buses), and crowded or open public places (grocery stores). His avoidance behavior, particularly the fact that he rarely leaves his house, supports the diagnosis. According to DSM-5 criteria, agoraphobia requires a duration of at least 6 months and fear in at least 2 situations, both of which are met in this case.
1000
"A 55-year-old female who was previously well, presented to the psychiatric service following episodic disorganised behaviour for two weeks duration. For example, she had cooked rice three times per meal without an apparent reason. Also, she had started collecting a large number of vegetables repeatedly in a shopping centre without a clear purpose. At that time her husband had to forcefully stop her. When inquired later she was unable to recall these events. Family members also noticed that the patient is having episodic repetitive facial movements without losing consciousness. General physical and neurological examination was normal." Episodes of behavioral change were sudden in on/offset and brief. The primary dignostic tool to make the diagnosis:
A. MRI brain wwo.
B. Lumbar puncture.
C. RPR/VDRL
D. EEG
E. Anti-CASPR2 antibody test.
F. Bake a cake with her urine and feed it to a dog.
What is D, an EEG? It may take a repeat EEG w/ different probe placement though.
Frontal lobe seizures tend to begin and end abruptly, are brief and frequent. They show a tendency to occur at night and in clusters. Motor phenomena which may include complex posturing and behavioural automatism are usually the most conspicuous feature.
This patient had several bizarre behaviours which could be complex behavioural automatism. The bizarre nature of automatism means that they can often be mistaken for non-epileptic dissociative seizures as well as another psychiatric diagnosis like mania or psychosis.
Read up on Anti-CASPR2.
The last choice was an odd test for witches.
1000
The shortest serving President and the longest serving President.
Who are William Henry Harrison and FDR?
1000
A 35-year-old man presents to the clinic for a follow-up exam. He complains of progressive fatigue, low mood, and weight loss. He was diagnosed with renal cell carcinoma 3 months ago and is currently undergoing chemotherapy. He reports having low mental and physical energy. His temperature is 98°F (36.7°C), pulse is 116/min, and blood pressure is 85/50 mmHg. Physical exam shows tanned skin and bluish-black gums. The abdomen is soft, nondistended, and nontender. Serum report is attached.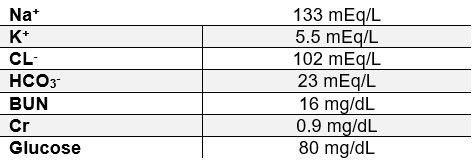
This will be the most appropriate treatment:
A. Glucocorticoids
B. Succimer
C. Fluoxetine
D. Deferoxamine
E. Levothyroxine
F. Mirtazapine
G. Boys trip to Cabo
What is A, glucocorticoids?
Findings of hypocortisolism include lethargy, weight loss, anorexia, gastrointestinal complaints, hypotension (due to decreased catecholamine‑induced vasoconstriction and myocardial contractility), decreased serum glucose (due to increased peripheral glucose utilization and decreased gluconeogenesis), and dilutional hyponatremia (due to increased secretion of antidiuretic hormone). Hyperpigmentation of the skin and gums is caused by the increased production of melanocyte-stimulating hormone.
Succimer is indicated in the treatment of lead poisoning. The gum discoloration due to lead exposure (i.e., the Burton line) appears as a thin line along the gums rather than generalized gum hyperpigmentation.
Fatigue, loss of appetite, and weight loss can be signs of MDD. However, this patient does not have sufficient signs to establish a diagnosis. Moreover, MDD does not account for this patient’s hypotension, hyperpigmentation, and laboratory abnormalities.
Deferoxamine is used in the treatment of acute and chronic iron toxicity. Additional features, such as hepatomegaly, heart failure, arthralgia, and diabetes, would be expected in such a patient.
Levothyroxine is the treatment of choice for hypothyroidism. This patient lacks other features of this condition, such as cold intolerance, edema, etc. to establish a diagnosis.
1000
These colonial cnidarians are considered the longest animals in the world.
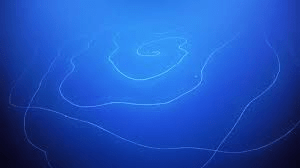
What is a siphonophore?