Thy-Roid Ragin'
Spit Happens
Lymphomaniac
I'm a Liver not a Fighter
Gut Feeling
"I need to speak to your Lab Manager!"
200
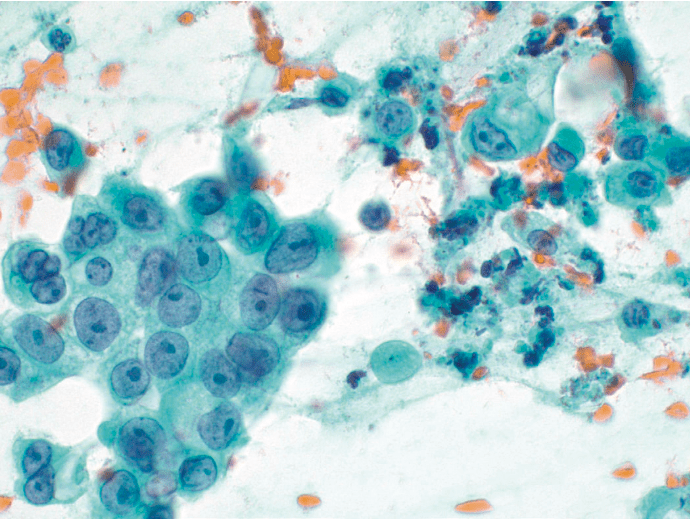
This is the FNA of a thyroid nodule in a 44-year-old woman. What is the best diagnosis?
Follicular neoplasm OR Suspicious for follicular neoplasm
200
Most common salivary gland neoplasm
 Pleomorphic adenoma
Pleomorphic adenoma
Bonus: most common malignant parotid gland neoplasm?
200
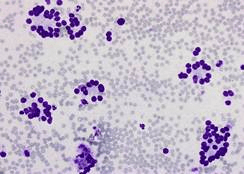
 29M LN FNA. Dz?
29M LN FNA. Dz?
Hodgkin lymphoma
(binucleated Reed-Sternberg cell, CD15/30+)
200
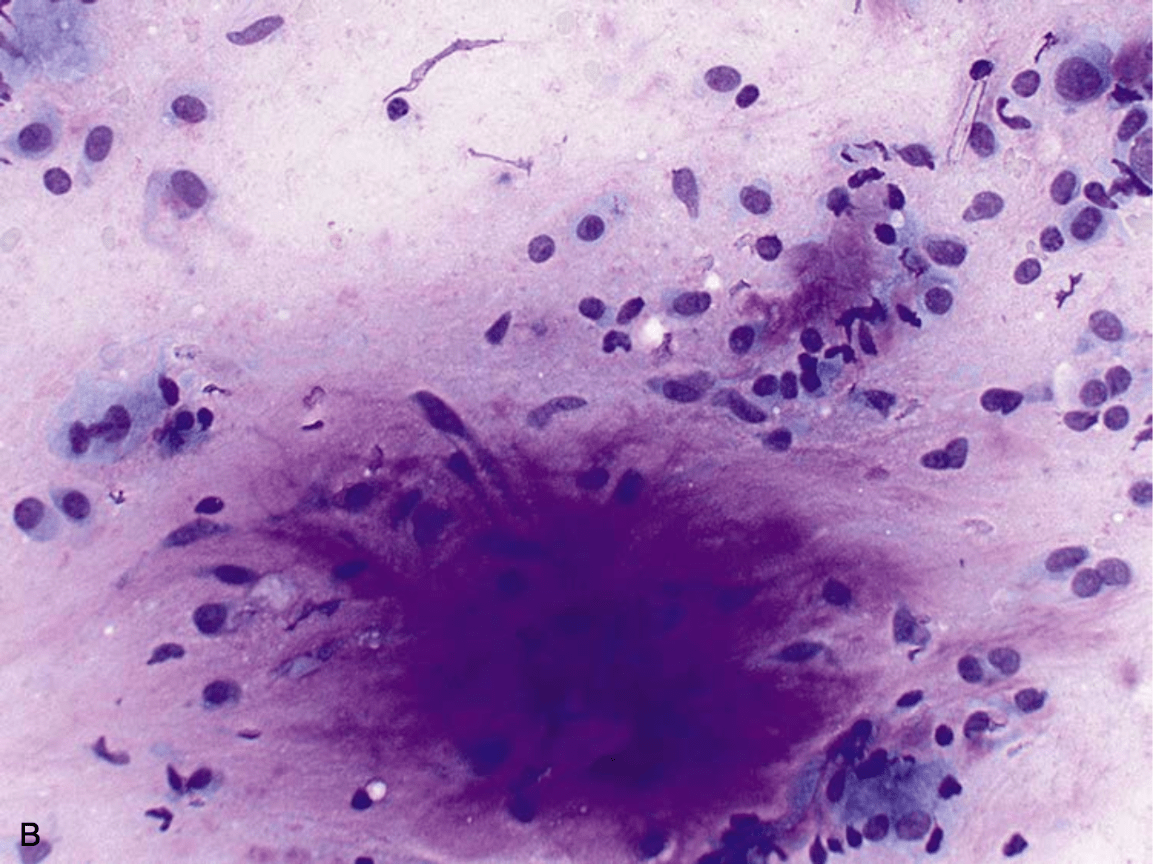
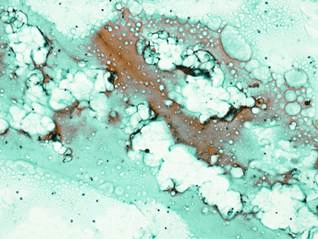
 29M from Vietnam, biliary obstruction, cholangitis. ERCP: biliary brush. Dx?
29M from Vietnam, biliary obstruction, cholangitis. ERCP: biliary brush. Dx?
Strongyloides stercoralis
200
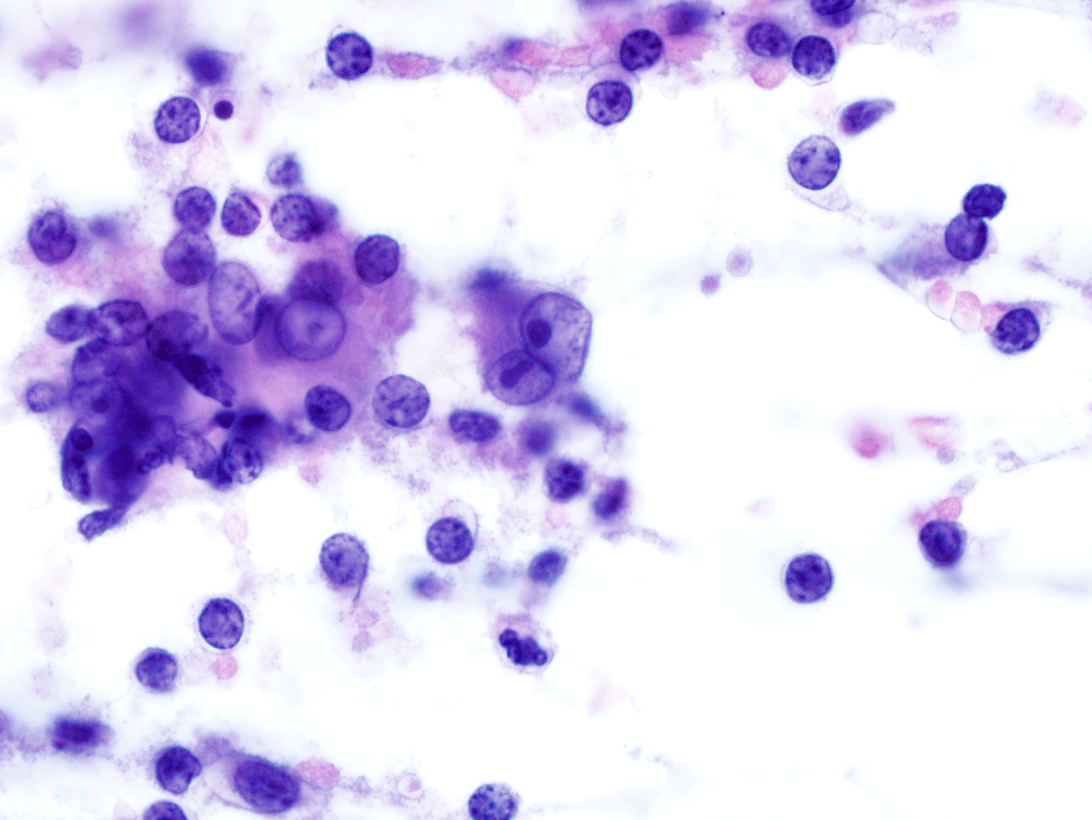
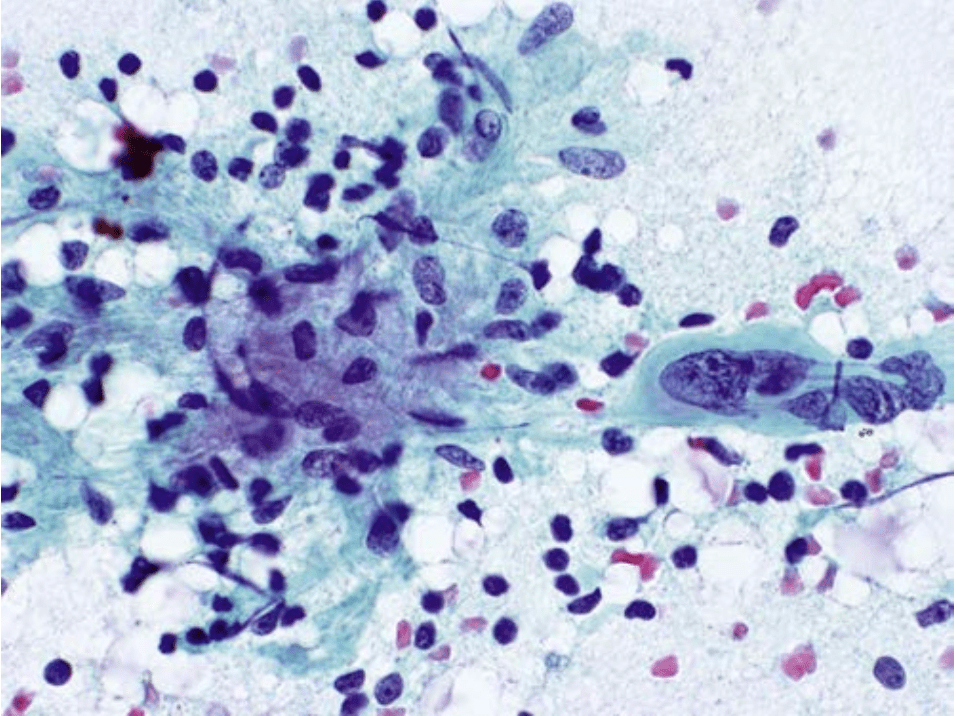
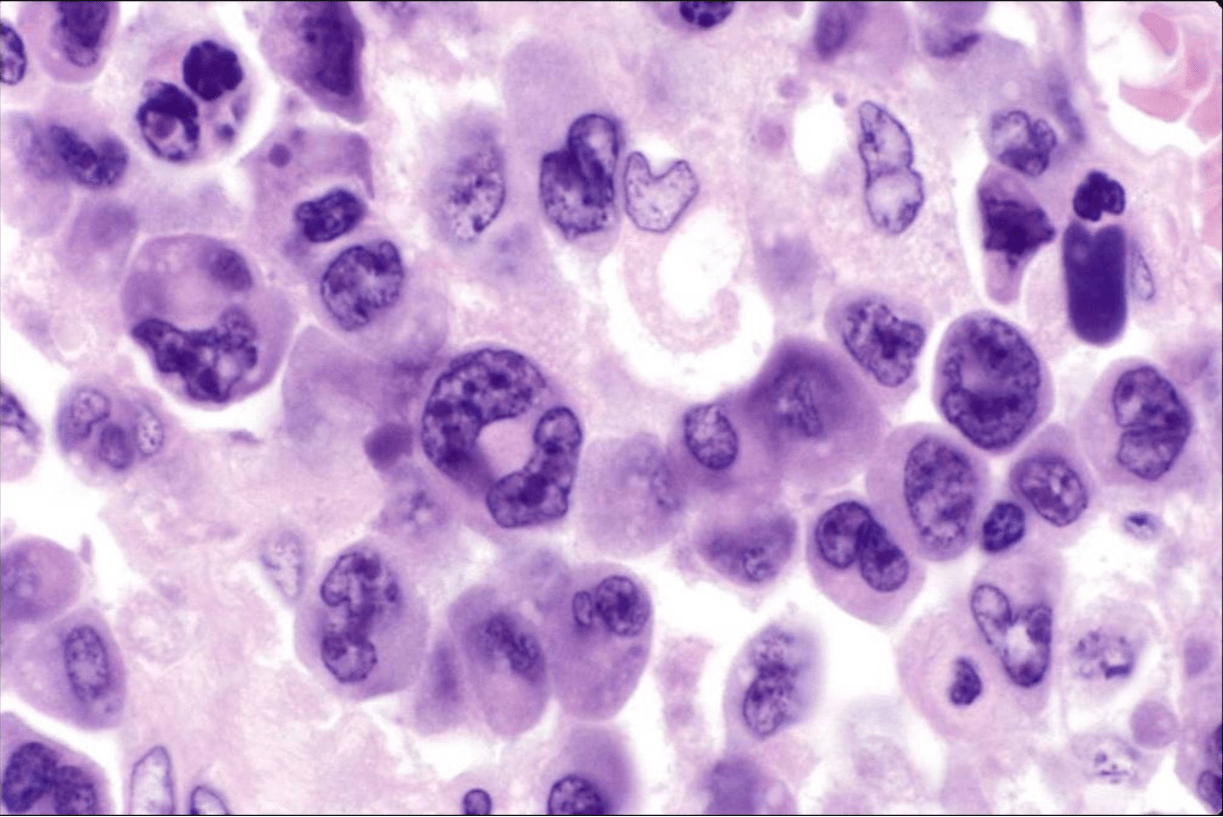
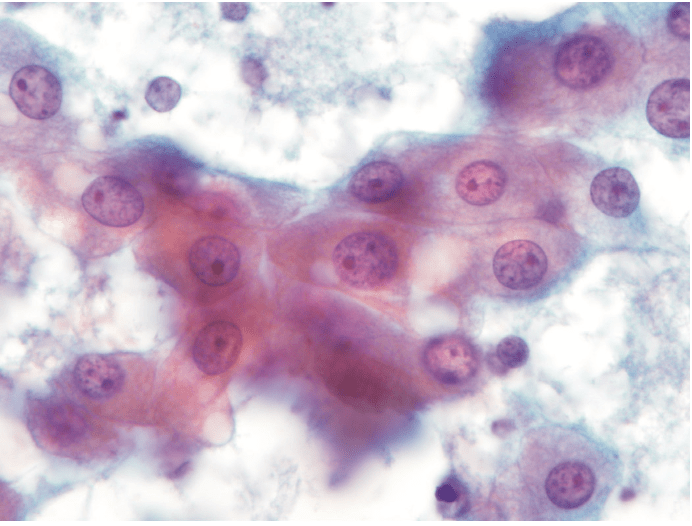
 Esophageal brushing. Dx?
Esophageal brushing. Dx?
CMV infection
Enlarged nuclei, prominent nuclear inclusion surrounded by broad halo, thick nuclear membrane (no multinucleation)
200
When a performance deficiency by a cytotechnologist or pathologist in a particular test is discovered, what is the first step?
Remove the employee from performing that particular test
400
Which gene fusion is seen in follicular carcinomas and follicular variant PTCs?
PAX8-PPAR fusion
400
Submandibular gland mass
Adenoid cystic carcinoma
Cribriform architecture, basaloid cells, variable hyaline matrix globules
400
Lymph node FNA smear. What these structures represent:

Cytoplasmic fragments (lymphoglandular bodies)
LGBs: fragile cytoplasm stripped off during smearing
400
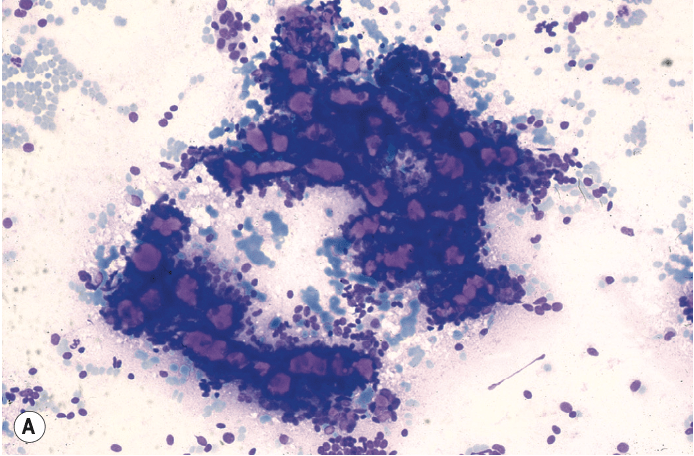
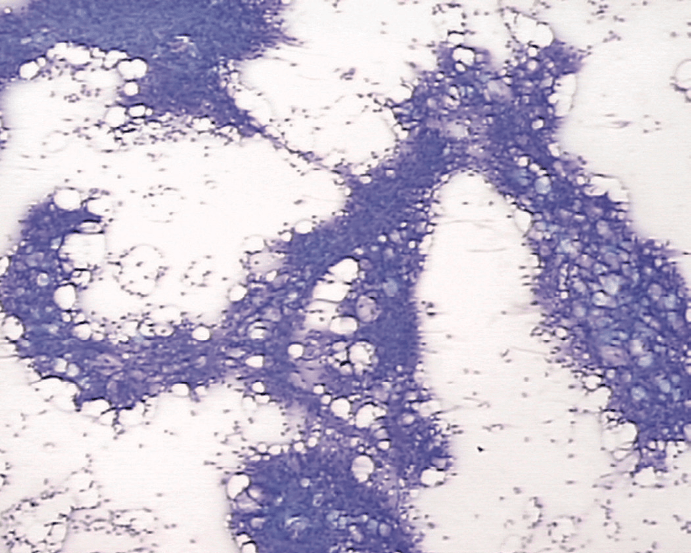
 50M, chronic HepC, multiple liver masses (FNA of largest one, smear). Best Dx?
50M, chronic HepC, multiple liver masses (FNA of largest one, smear). Best Dx?
Hepatocellular carcinoma
400
 EUS-FNA: duodenal wall mass. SMA-, CD117-, DOG1+.
EUS-FNA: duodenal wall mass. SMA-, CD117-, DOG1+.
Gastrointestinal stromal tumor (GIST)
(up to 15% GISTs are CD117 negative)
400
Under CLIA 88, one CLIA laboratory director can be the directory of how many non-waived laboratories simultaneously?
5
600
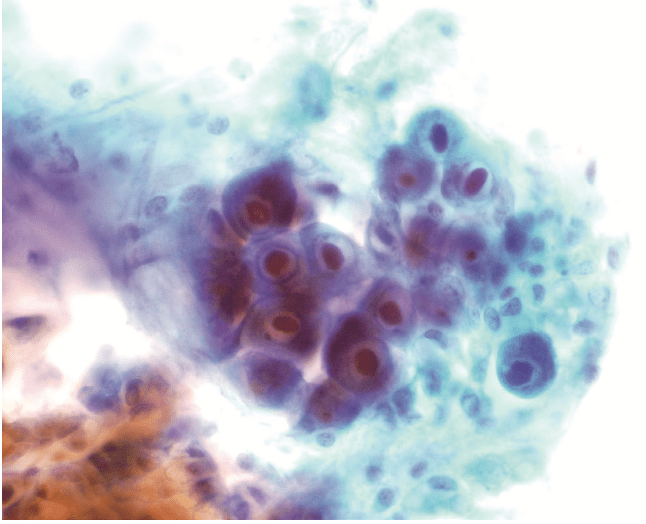
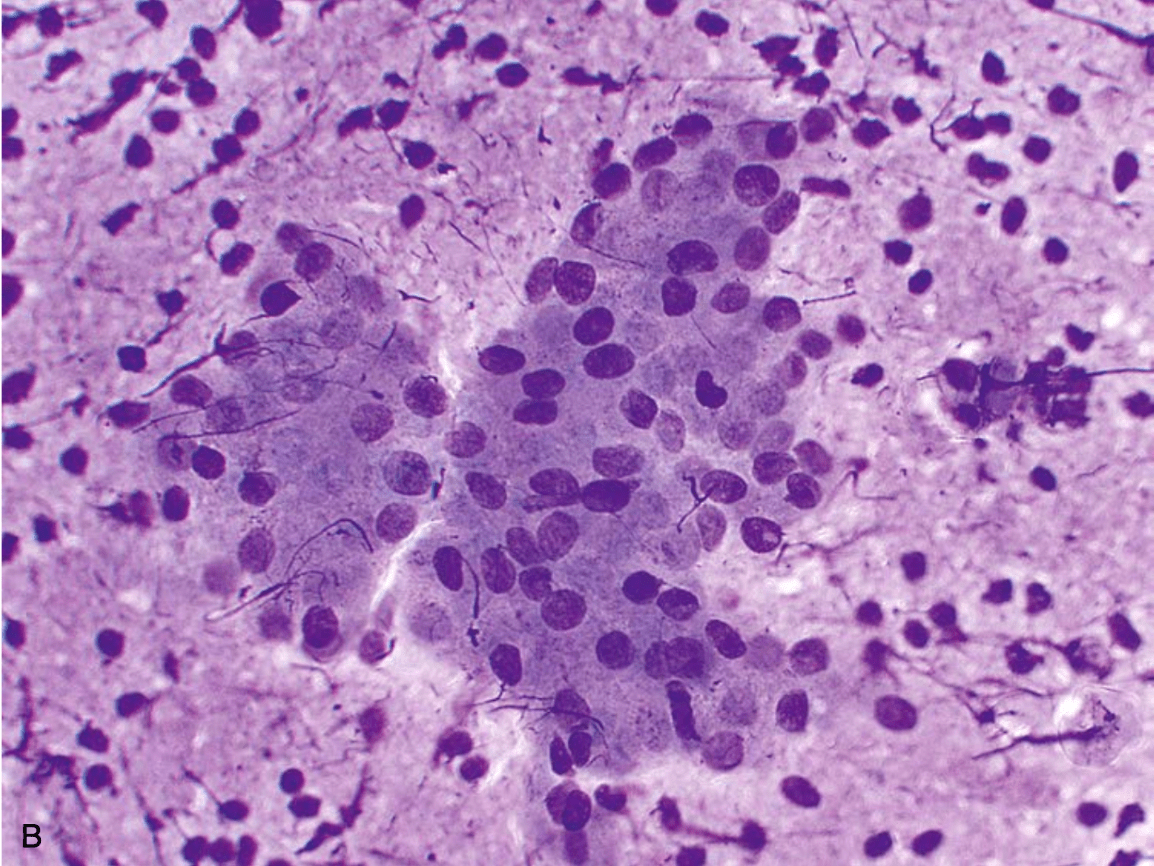
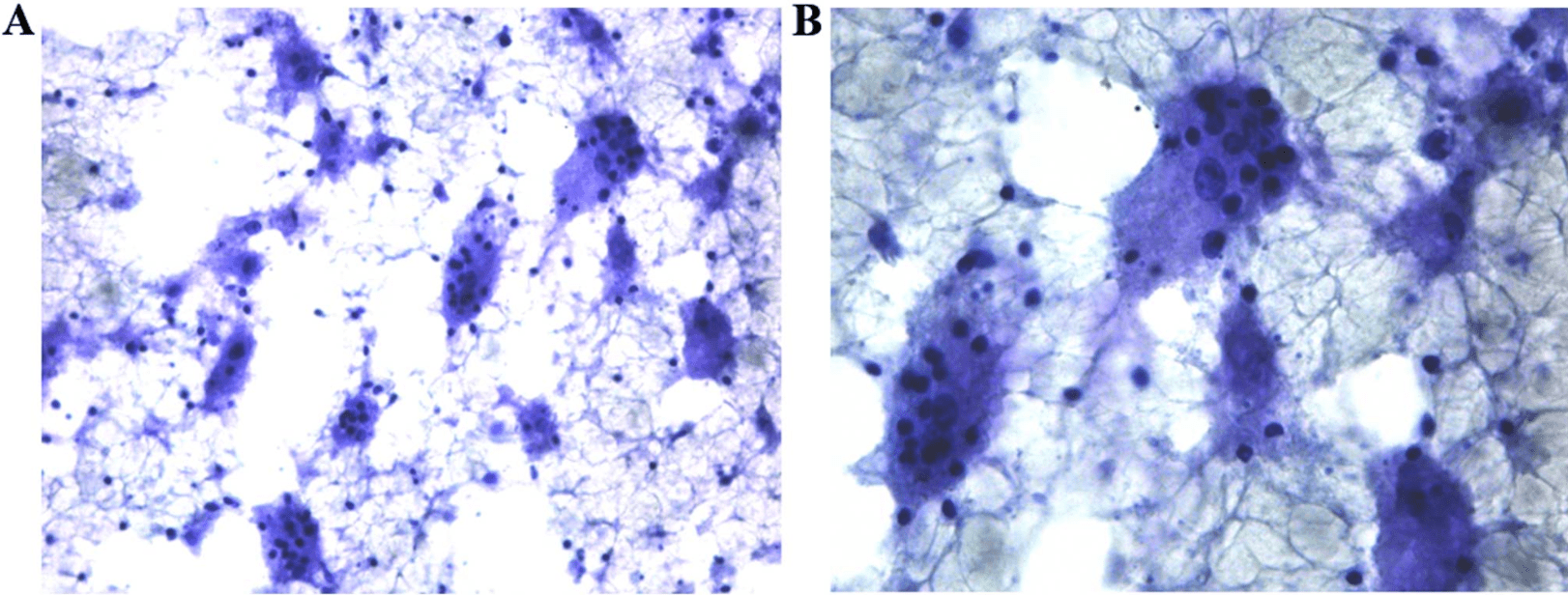
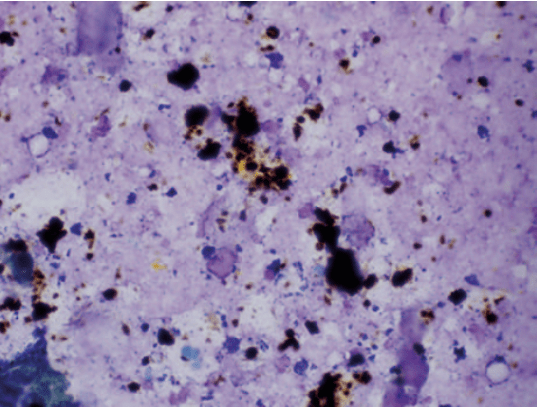
This smear was prepared from a thyroid FNA of a young adult patient who had a prior history of pheochromocytoma. What is the most likely diagnosis?
Medullary thyroid carcinoma
600
 68M, parotid FNA. Most likely Dx.
68M, parotid FNA. Most likely Dx.
Warthin tumor (cystadenolymphoma, papillary cystadenoma lymphomatosum)
Smooth, dense cytoplasm, background granular debris, lymphocytes with smearing artifact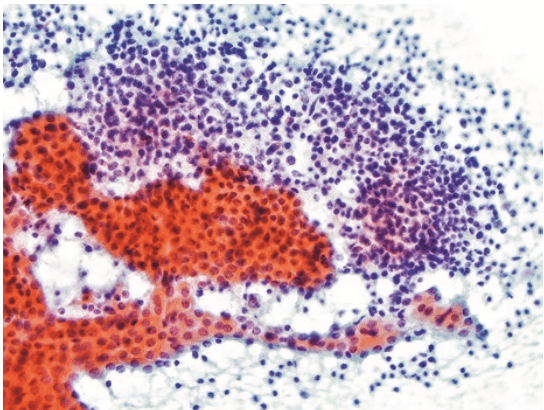
600
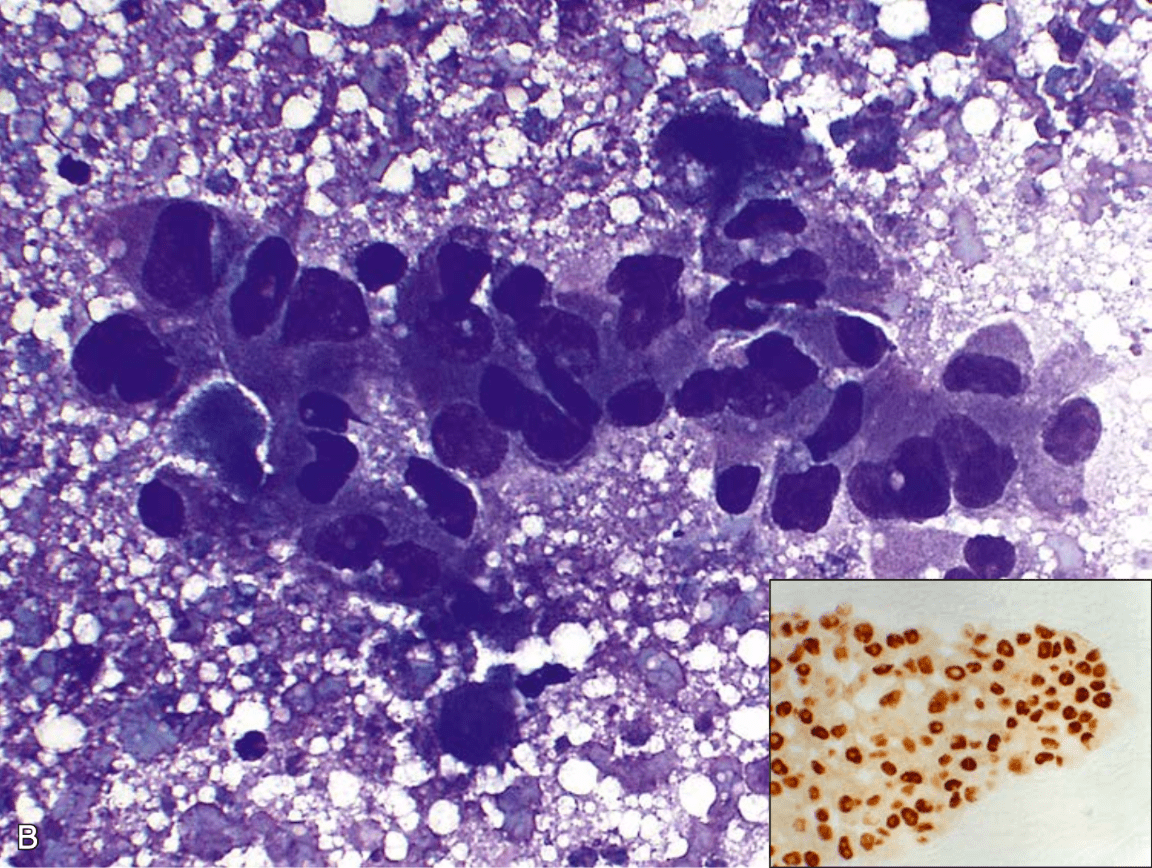
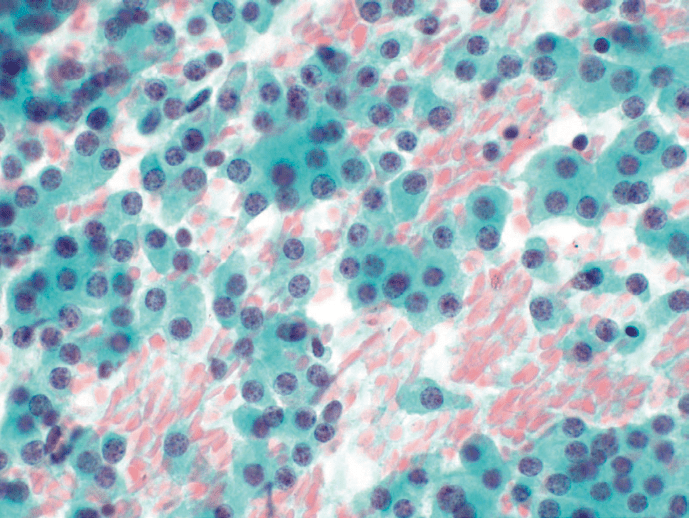
 32M, retroperitoneal LN FNA. Dx?
32M, retroperitoneal LN FNA. Dx?
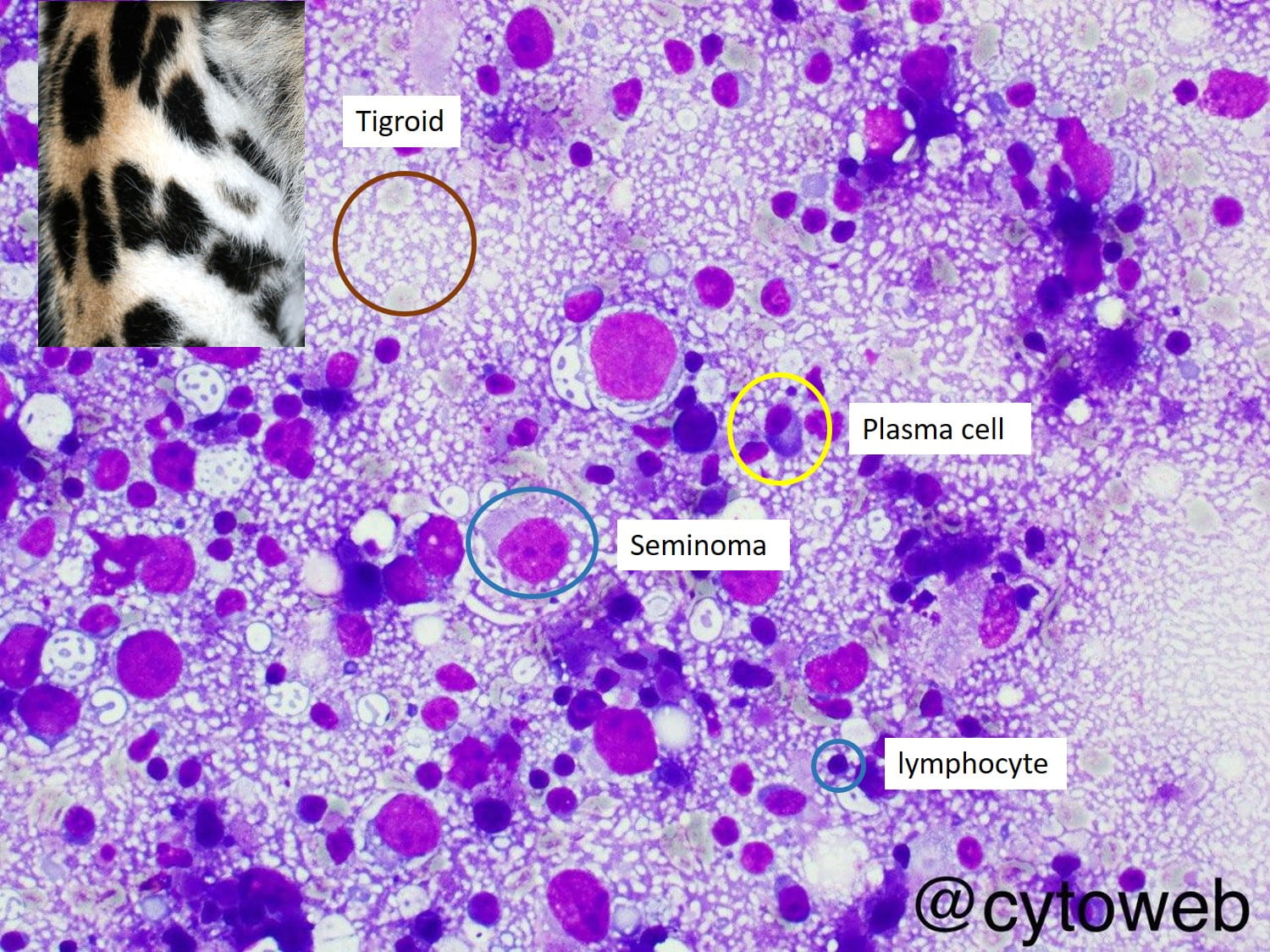 Metastatic seminoma
Metastatic seminoma
600
 34M, tuberous sclerosis, incidental liver lesion. FNA: adipocytes, endothelial cells, abundant blood, spindled/epithelioid cell clusters, hematopoietic cells. Cell block: plump spindle cells, HMB45+. Dx?
34M, tuberous sclerosis, incidental liver lesion. FNA: adipocytes, endothelial cells, abundant blood, spindled/epithelioid cell clusters, hematopoietic cells. Cell block: plump spindle cells, HMB45+. Dx?
Angiomyolipoma
600
 65M, jaundice, weight loss, pancreatic head mass. EUS-FNA: Dx?
65M, jaundice, weight loss, pancreatic head mass. EUS-FNA: Dx?
Pancreatic ductal adenocarcinoma
600
Atypical squamous cell (ASC) to squamous intraepithelial lesion (SIL) ratio is considered a good empirical benchmark for determining if the diagnostician is using ASC too frequently. What is the generally accepted upper limit for this ratio?
3:1
800
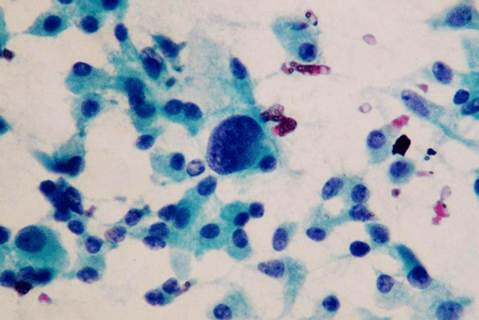
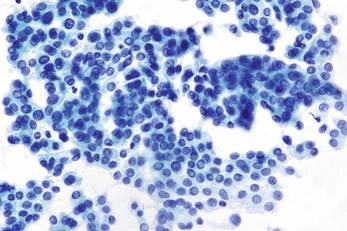
This smear was prepared from the FNA of a thyroid nodule in a 30-year-old woman. What would be the appropriate management for this patient?
Clinical follow-up
800
 82M, FNA 4cm salivary mass. Inset: AR IHC. Most common site (majority occur in?).
82M, FNA 4cm salivary mass. Inset: AR IHC. Most common site (majority occur in?).
Most common site = parotid
(majority occur in minor salivary glands)
800
 24M, FNA smear of enlarged cervical LN. Based on morphology, what IHC would render a definitive Dx?
24M, FNA smear of enlarged cervical LN. Based on morphology, what IHC would render a definitive Dx?
ALK-1 (ALCL, hallmark cells)
800
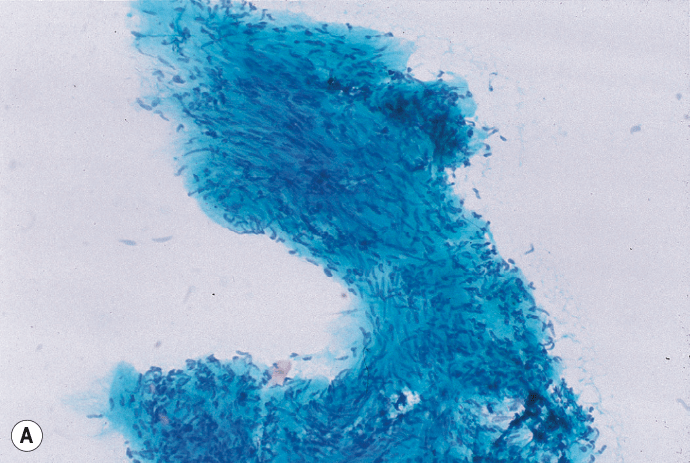
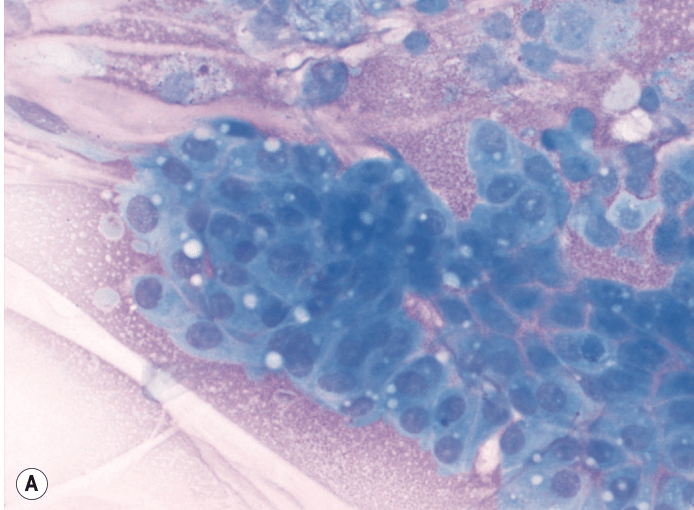
 Img from CT-guided FNA of RLL lung mass. Cells most likely represent?
Img from CT-guided FNA of RLL lung mass. Cells most likely represent?
Normal hepatocytes
Needle may inadvertently enter liver especially if targeting right-sided organs/lesions
800
 42F w/ VHL syndrome, pancreatic head mass. EUS-FNA: Dx?
42F w/ VHL syndrome, pancreatic head mass. EUS-FNA: Dx?
Pancreatic endocrine neoplasm
(VHL: renal cell carcinoma, pheochromocytoma, pancreatic endocrine neoplasms)
800
Per federal requirement, how long must gynecologic cytology slides be retained?
5 years
1000
Which specific mutation in this papillary thyroid carcinoma is associated with frequent extrathyroidal extension?
BRAF V600E
1000
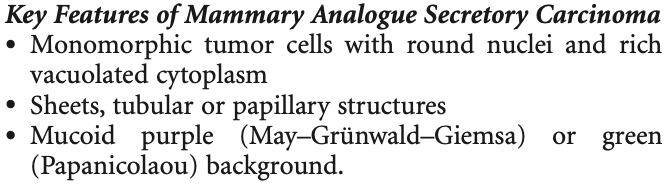
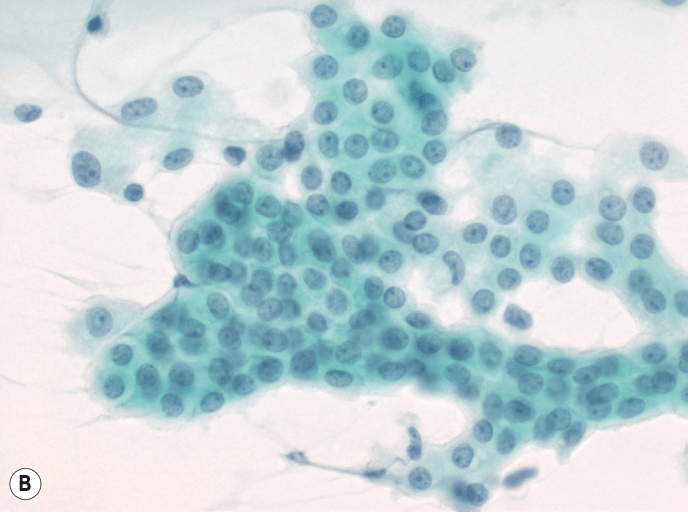 62M, parotid FNA: cellular aspirate, large cells w/ abundant eosinophilic/vacuolated cytoplasm (no granules), round eccentric nuclei w/ prominent nucleoli. S100+. Gene fusion?
62M, parotid FNA: cellular aspirate, large cells w/ abundant eosinophilic/vacuolated cytoplasm (no granules), round eccentric nuclei w/ prominent nucleoli. S100+. Gene fusion?
ETV6-NTRK3
1000
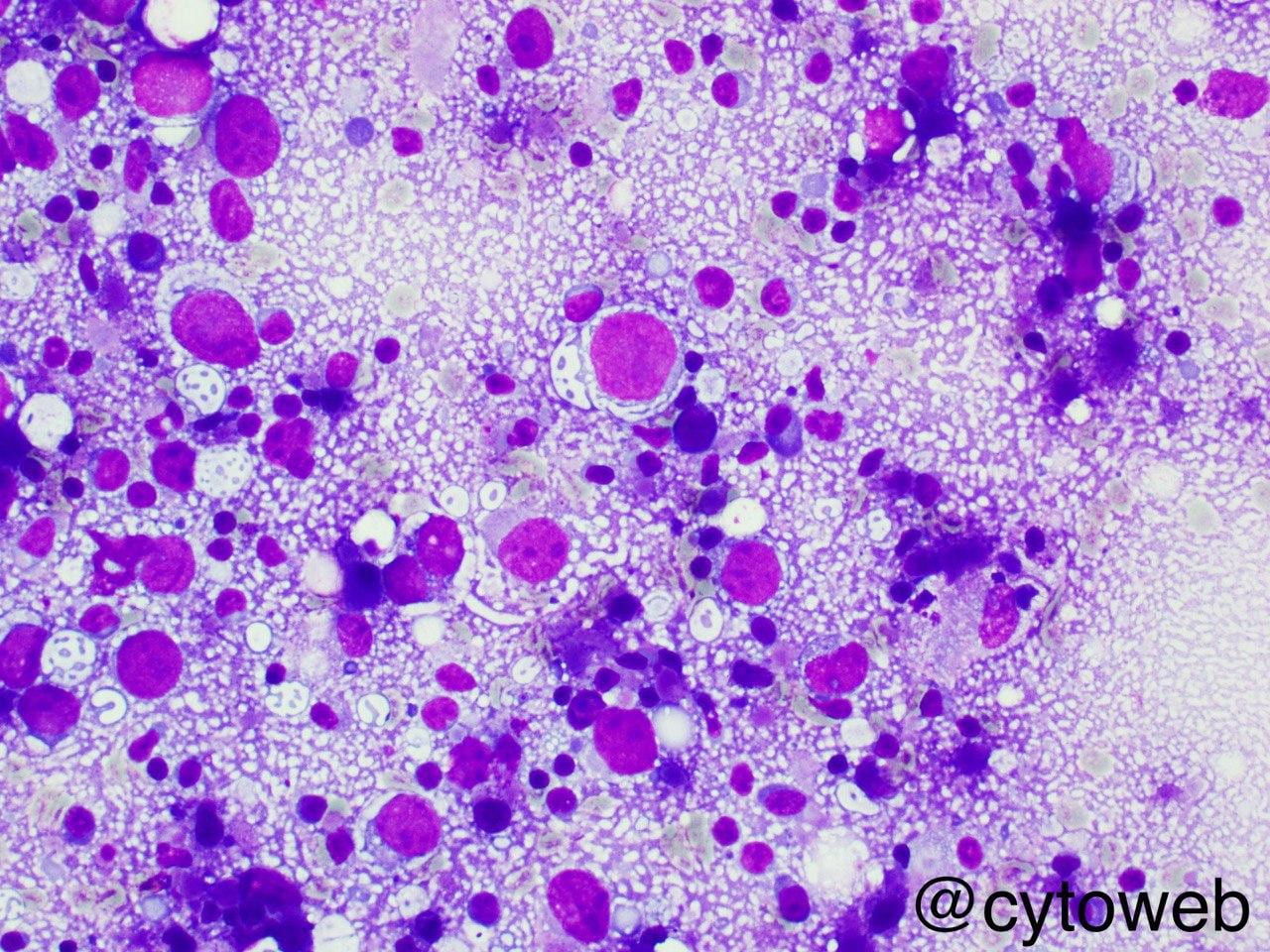
35M, b/l painless cervical LAD, fever, night sweats. FNA smear. Dx?
Rosai-Dorfman Disease

1000
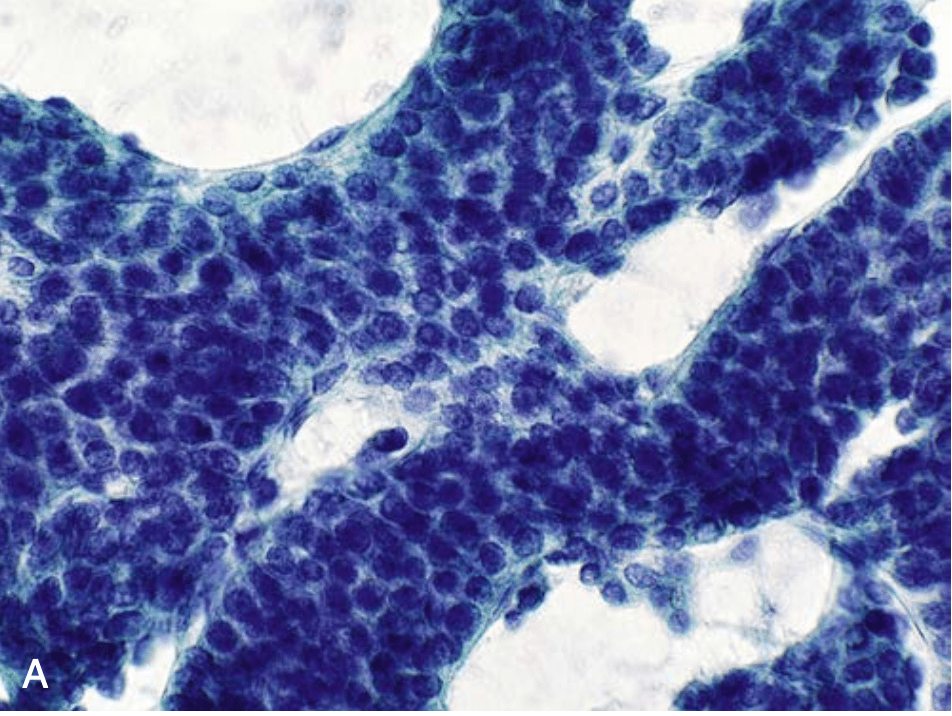
 50M, EtOH cirrhosis, CT-FNA dominant nodule/mass in right liver lobe. Best interpretation?
50M, EtOH cirrhosis, CT-FNA dominant nodule/mass in right liver lobe. Best interpretation?
Regenerative nodule in cirrhosis

DDx: normal liver, focal nodular hyperplasia, nodular regenerative hyperplasia, steatosis, regenerative nodule in cirrhosis
1000
42M, pancreatic head cyst. Dx?
Pseudocyst (Cyst fluid studies results?)
granular debris, macrophages, bile w/o epithelial cells
Cystic panc lesions DDx: pseudocyst, MCN, IPMN, SCA
1000
Per CLIA 88 and CLIA 67, what percentage of negative Paps require prospective rescreening?
10%