Going Viral
Scales of truth
Non-Blanching!! :O
WTR
Dermurgent
100
2 1/2 y/o boy, fever one night ago but otherwise well, new itchy rash, some blisters
no foreign travel, sister well aged 9
Chicken Pox (Varicella Zoster)
Free chickenpox vaccination when they’re 15 months old or 11 year olds who have not been vaccinated already/if they have not had a confirmed chickenpox infection.
Two doses of the chickenpox vaccine are more than 90% effective at preventing the disease.
100
3 year old small graze to chin, now has a few lesions as below. Generally well.
Vaccinations up to date, no contacts unwell, no recent travel. 

Staphylococcus aureus and Streptococcus pyogenes, either alone or together, are the most common causes of impetigo.
Manage on severity, topical vs oral Abx. Can develop into bullous impetigo.
Very infectious, avoid sharing towels etc.
100
7 Year old, 12-24 hour history of worsening rash as below. Afebrile, PEWS 1, Relatively well with mum. Possible viral illness 3 weeks ago.

ITP vs Haem malignancy
Hard to tell prior to bloods
High level of concern, check for bleeding.
Be very sure not missing meningococcal.
ITP - Diagnosis of exclusion: • Platelet count < 100k with no other cytopenias or abnormalities on peripheral blood smear
100
Sheep farmers son, painful lesion to the hand over last few days. Generally well.

Orf
Pox virus from sheep/goats
No specific treatment, treat bacterial superinfection as needed.
Preventative advice
100
28 year old man, otalgia for 4 days. Today noted some blood when taking headphone off.
Wife noted facial droop to left side, called ambulance ?stroke.
No PMH of note

Ramsay-hunt Syndrome
- Shingles/VZV of Facial nerve
- Facial Nerve palsy
- Aciclovir or other antiviral + short dose steroid, reduces long term complications.
200
3 y/o boy febrile, cough, coryza and generally unwell. PEWS 7. unvaccinated. O/e: a little grizzly and these:

 Measles (koplik Spots)
Measles (koplik Spots)
- Unvaccinated children, danger to immunocompromised and pregnant
- Contacts can be given MMR if not vaccinated (if not full course)
- Supportive treatment, Vitamin A, can be very unwell or die.
200
6 Month Boy, normally has mild Flexural rash and dry cheeks. Now worsening. Snotty nose but reasonably well. No fevers, rash dry. Given "some creams" by GP use once or twice a day.
Atopic Eczema
- Very common
- Manage as per treatment ladder, most common reason for flare is poor adherence to emollients. Other illnesses can flare.
200
Child with mild URTI symptoms, on full inspection note rash to buttocks. 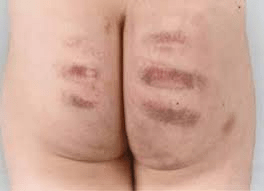
Non-accidental Injury
Symptoms not fitting with presentation.
Look for other red flags
Discuss with senior/Social work team.
200
8 y/o Unwell with arthralgia, low grade fever, fatigue. Family camping holiday last week in US, all other contacts well. Vaccinated.

Lyme Disease
Borrelia Burgofedi
Tick Bites - ticks infected, normally the smaller nymphs.
If not treated can progress to chronic disease.
200
6 year old girl, had otitis media and started course of amoxicillin a 7 days ago. Now very unwell, diffuse rash, sore eyes, sore mouth and arthralgia.
Temp 39.5, Vaccinated, no travel history. 
Steven Johnsons Syndrome
- Scale of Disease from EM -> TEN
- Supportive care, stop precipitating drug.
300
2 year old, Recently been to day care. Currently febrile, with new rash. Generally quite well, PEWS 1. Easting and drinking. Nothing in mouth, is up to date with vaccines.

Roseola HHV6 (could be a number of viruses)
Febrile illness, normally tolerated. No concerns.
Difficult to distinguish from other viral exanthems.
Very rare to have complications (encephalitis etc)
300
7 year old boy, itchy armpit for 3 weeks. Generally well.
Vaccinated, family well, no recent travel
Tinea Corporis (Axilla)
"Ringworm"
Treat with topical Idimazole, Normally rash will quickly resolve with topical steroid but need to treat underlying fungal infection for 2 weeks after rash disappears.
300
7 year old child, very unwell at home. Mum noted small palpable rash to leg earlier this evening. Temp 39, Tachycardic, Tachypnoeic. 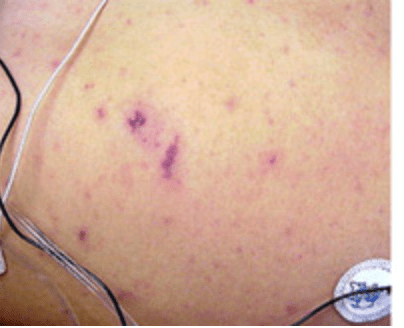
Meningococcal Disease/Sepsis
Treat as sepsis
IV Cefuroxime if <28 days (theoretical risk of Kernicterus and biliary complications)
Ceftriaxone if older
Ben Pen IM if community based and unable to get access.

300
5 year old, unwell for two days with sore throat fever and loss of appetite. O/e widespread rash, red tonsils, tongue as below. Rash feels sandpapery.
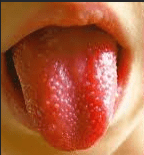
Scarlet Fever
- Strep A bacteria, normally pharyngitis
- More common in school age children
- Rx with penicillins
- Send throat swab for confirmation.
300
5 year old male, Febrile for 8 days straight, last 3 days sore joints, sore eyes and generally unwell.
Vaccinated, No travel.
O/E: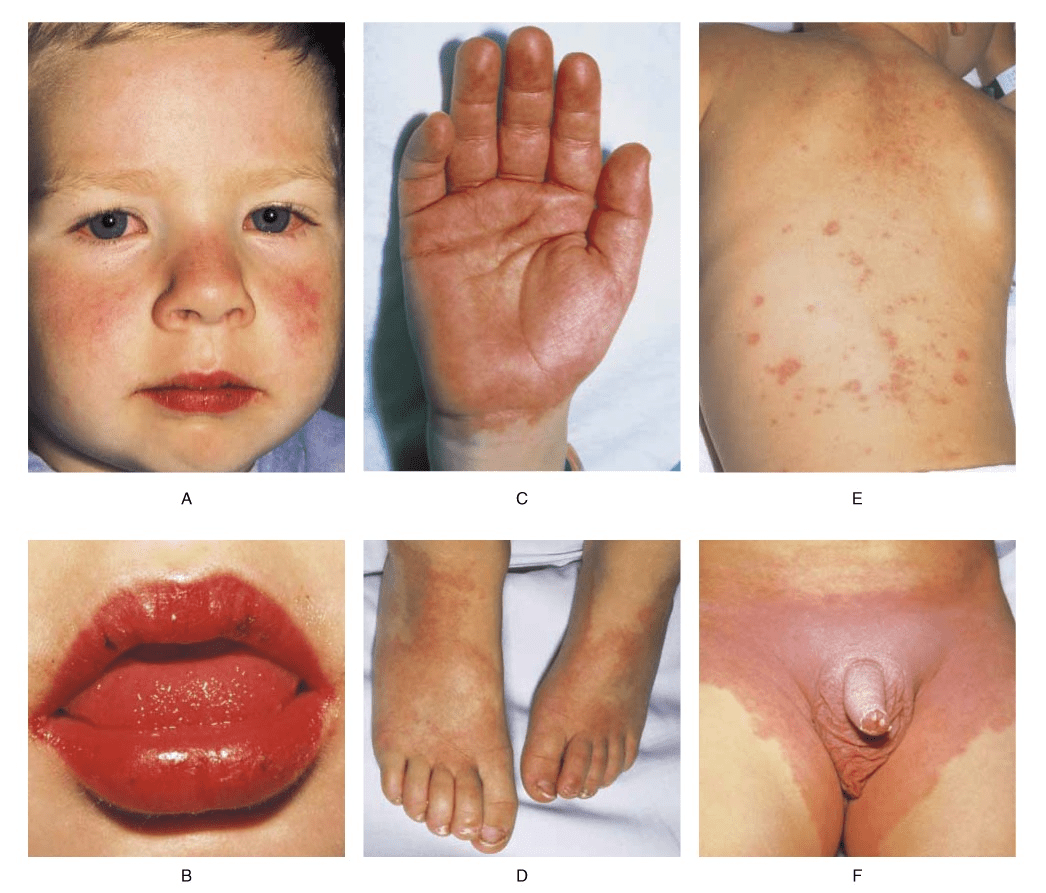
Kawasaki Disease
- Abdominal pain and D & V can be present
- Risk is cardiac complications (aneurysms and myocarditis)
- Treat with IVIG and Aspirin
400
4 y/o Girl, Fever, Grizzly, Burning hot red cheeks and rash developing as below. Vaccinated, no recent travel

Slapped Cheek Syndrome (parvovirus B19)
- Self Limiting
- Avoid Pregnant, Immunosuppressed, thalassemia and sickle cell.
Can also present with very rare purpuric gloves and sock syndrome
400
6 year old Itchy rash, all over but particularly to hands. Worse at night. Family stayed at mountain Hut. Sister also itchy. Systemically well.
Vaccinated.

Scabies (sarcoptes scabiei parasitic mite)
Often transferred in bedding/clothing.
Can try burrow ink test
Treat with permetherin - leave on overnight
Treat whole family
Ask to hot wash all clothes and bedsheets.
If fails can progress to oral treatment (ivermectin)
400
2 year old, tummy pain, refusing to stand. Afebrile. Rash started on bum now spreading down legs. Very little or none above umbillicus.
Henoch-Schonlein Purpura
Small vessel Vasculitis
If well and no renal involvement, treat pain and follow up as per starship.
Watch for haematuria and Blood in stool
400
Recent sniffles given Amoxicillin by GP, seems much better but mum very concerned regarding rash 
Erythema Multiforme
Multiple causes
- Commonly infection (90%), of these HSV1 is most common.
- Drugs (Penicillins, Cefalosporins)
-
400
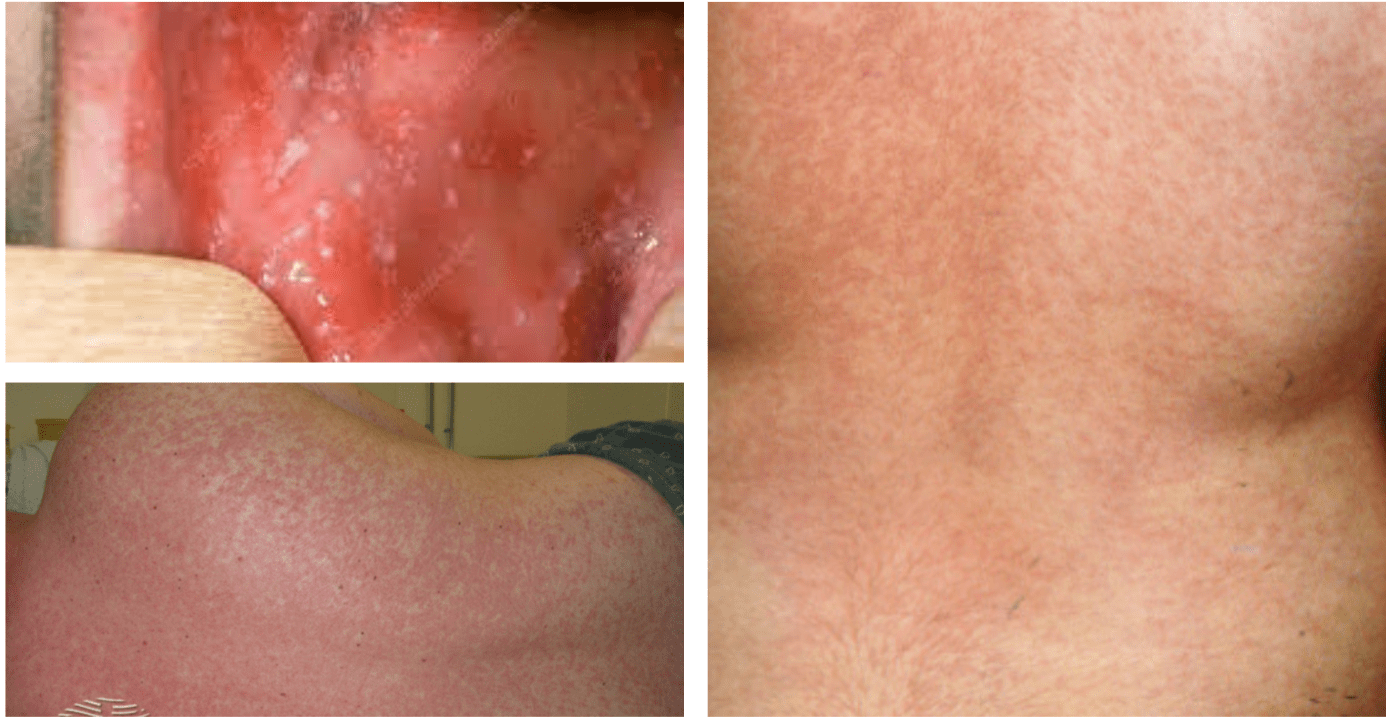
8 year old girl slightly unwell for last week with cold, brother more notably snotty. Background of eczema uses emollients regularly.
Vaccinated, no travel.
Eczema Herpeticum
- HSV-1 in broken skin
- Requires either IV aciclovir or PO valaciclovir
- Close monitoring and Opthal review if near Eye
500
8 year old boy, unwell last week with sore throat and myalgia. Now well, rash started with one lesion now developed to this up to date with vaccines.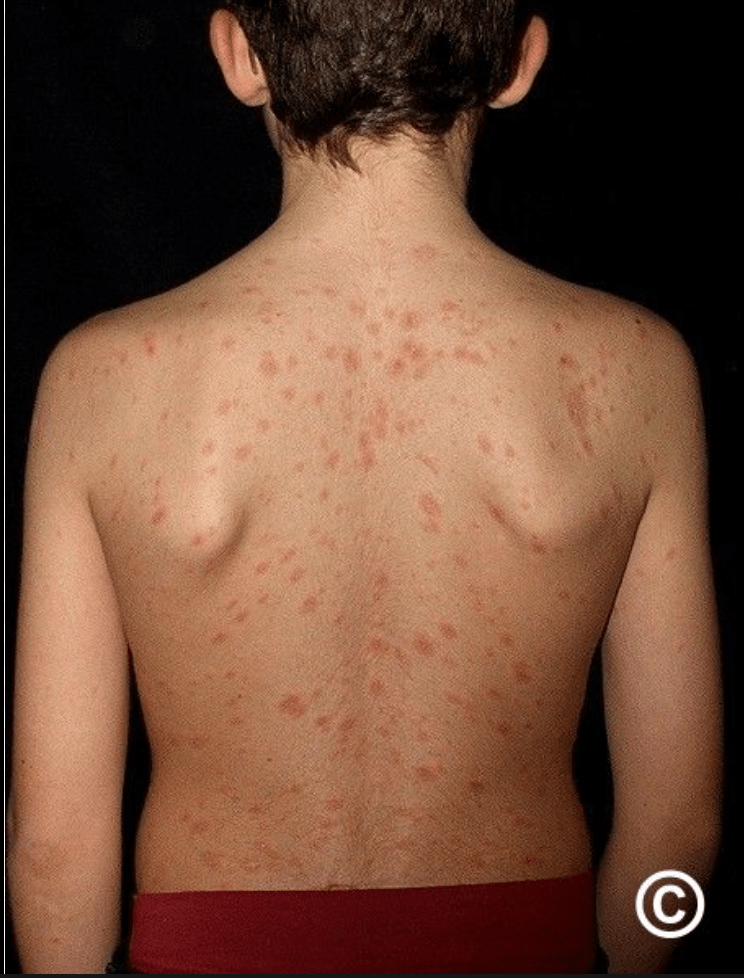

Pityriasis Rosea
Often viral but no cuase found in many cases. Self limiting and no specific treatment
May last 6-12 weeks.
500
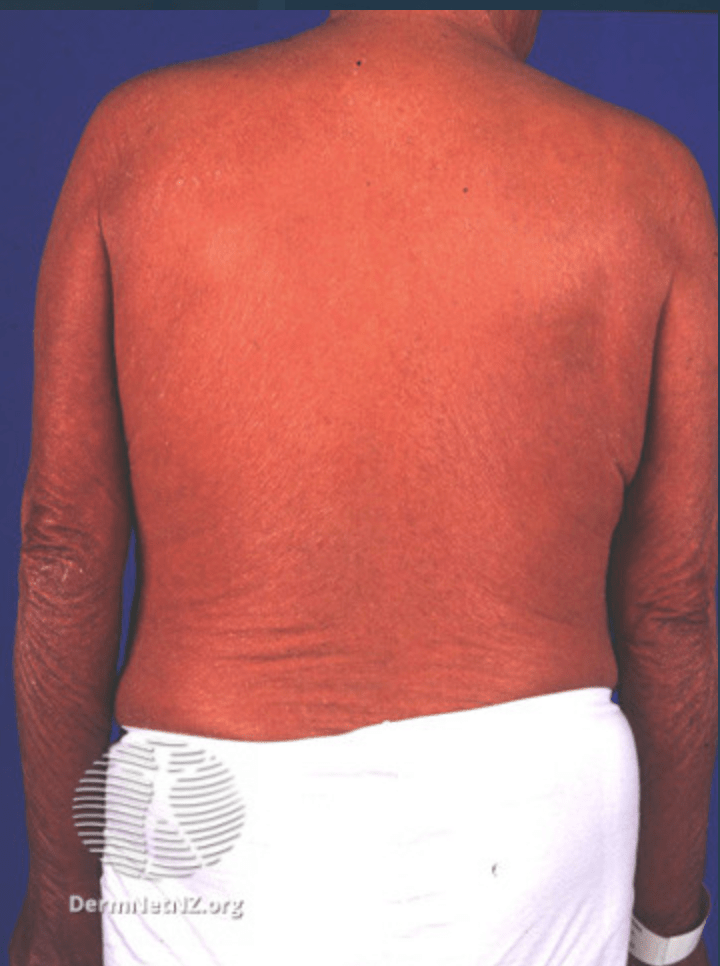 43 y/o man, known Psoriasis. Febrile and looks like below
43 y/o man, known Psoriasis. Febrile and looks like below
Erythromderma
>90% body, erythematous and oedemantous
ABCDE approach admission for emollients, warmth, fluids +/- treat infection
500
7 year old child, Non-bloody Diarrhoea and vomiting for 2 days. Now improving, GP sent stool and viral cause found. Rash above both eyes, some on neck. No spread and all above nipples. 
SVC distribution pressure, coughing or vomiting, Capillary rupture. Not concerning
Other - BP Cuffs etc causing small petchiae.
500
3 year old, mum noticed cluster of lesions in armpit. Saw GP before who said they were ok, now seem to have spread. Mum very concerned. Child well. 
Molluscum Contangiosum (Pox virus)
No specific treatment necessary as benign
Can offer podphyllotoxin, salicylic acid, hydrogen peroxide. Also surgical therapies, none specifically indicated.
Spread by direct contact but also shared towels etc
500
6 year old, Unwell 4 weeks ago with sore throat, did not get treatment as family were away. Now febrile again developing rash and polyarthralgia.
Vaccinated, Maori heritage. 
Rheumatic Fever (Eryhtema Marginatum)
- 5-15 year olds
- Lacy widespread rash
- Jones Criteria (2 majors or 1 major 2 minor)
- Starts on chest, sparing face and extremities.