Valves & Vibes
Gram negative attitude
Just breathe
Gut feelings
Misc and history of medicine
100
68 y/o M here for f/u. Patient report hx of afib on eliquis and some sort of heart valve surgery correction.
Which specific valve conditions would make this anticoagulation choice inappropriate ????
Severe Mitral Stenosis and mechanical valve!!!!!!
-Bioprosthetic valves >> ok for DOACs.
-TAVR >> DOACs often ok.
-AS/AR >> DOACs ok.
-Mild MS >> DOACs ok.
But mechanical valve and severe MS >> warfarin only!!!
100
78 y/o F resident from White oak comes with fever, cough and right lobe infiltrate on CXR. No recent hospitalizations but she lives at that nursing home. What is the empiric antibiotic regimen for this patients per IDSA guidelines????
beta lactam (ampi/sulbactam or ceftriaxone) + macrolide (azithromycin) OR fluoroquinolone.
nursing home residents fall under HCAP but last IDSA >> formal HCAP category was removed from guidelines because it lead to overuse of broad spectrum antibiotics. current guidance recommends individualizing the decision based on:
local antibiograma, patients personal risk factors, clinical severity on presentation.
100
66 y/o smoker M c.w sob and cough. FEV1/FVC of 0.58, post bronchodilator with FEV1 55% predicted. he is only on albuterol prn. according to gold guidelines, what mantainance inhaler should be initiated??
LAMA or LABA/LAMA combination for gold grade 2
LAMA preferred over LABA as mono therapy.
triple therapy (laba, lama, ics) reserved for frequent exacerbations or eosinophils count > 300!
smoking is the best intervention proven to slow the natural decline in FEV1
100
52 y/o m with alcohol abuse c.w hematemesis and melena. he is tachy and hypotensive. IVF are started. what is the hb threshold for transfusion in this patient?
hb 7.
over transfusion increases portal pressure and rebreeding risk!
100
a nurse calls you at 2 am to report a blood pressure of 182/94 in an asx patient post op. you ask 3 questions before ordering anything, what are they ??
1 is this patient symptomatic (headache etc)
2 baseline bp
3. cuff size
do not treated the number, treat the patient, asx hypertension is hospitalized patient almost never requires emergency treatment.
200
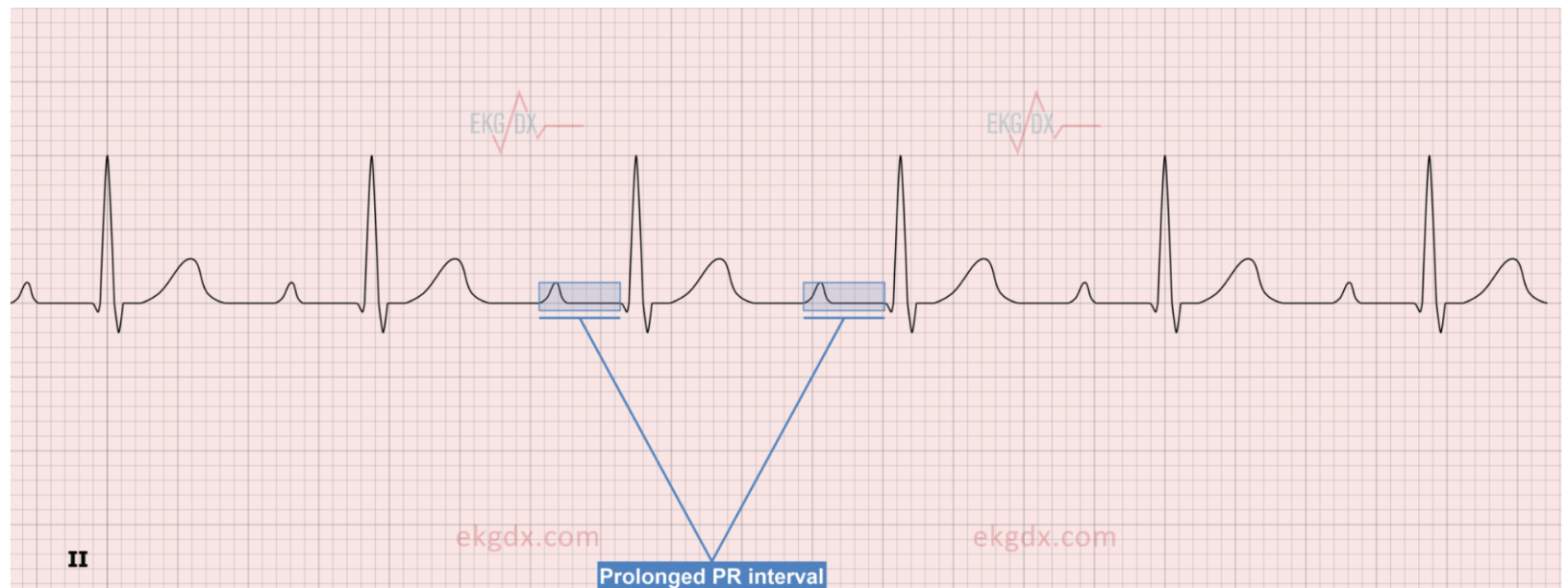 Name this condition?
Name this condition?
first degree AV block. most common in athletes and medication side effect (bb, cubs, digoxin), no treatment in asx patients.
200

55 y/o m with DM admitted with this swollen, erythematous right leg with a defined raised border. What is the most likely diagnosis and most likely causative organism???
ERYSIPELA. Group A strep!
raised, sharply demarcated border distinguishes erysipelas (superficial dermis/lymphatics) from cellulitis.
if cellulitis is suspected mark the border with a skin marker to track progression.
200
71 y/o F post op day 3 from hip replacement develops chest pain, tachycardia, hypoxia and swollen left calf. CTA confirms pe.
What is the Wells score telling you to do before CTPA???
TREAT empirically with anticoagulation before CTPA is no contraindication.
wells criteria:
-clinical signs of dvt +3
-no alternative dx +3
-hr > 100 +1.5
-Immobilization/surgery within 4 weeks +1.5
200
44 y/o W comes with and pain, vomit, lipase 1840, tg of 1200, bun is 22 and creat is 1.4, HCT is 48%, using the BISAP score which findings here increases her mortality risk? what is the most critical early intervention in the first 24 hours?
BISAP is your triage tool at admission.
B > BUN >25
I impaired mental status
S SIRD > 2
A AGE > 60
P pleural effusion
0-2 <1%, 3 5-8%, 4 13%, 5 22%
LR!!! aggressive ivy is the only intervention with mortality benefit regardless of etiology.
200
TRUE OR FALSE. If a patient leaves against medical advice his insurance won't pay the bill????
this is a myth, insurances does not automatically deny ama discharges.
300
19 y/o M collapses during basketball game and is resuscitated from VF. echo showed septal hypertrophy, what's the diagnosis ??
hypertrophic obstructive cardiomyopathy.
hcm is the most common cause of sudden cardiac death in young athletes!
300
67 y/o F on broad spectrum antibiotics for 8 days develops 10 watery stools/day, crampy abdominal pain, abc 28K, ct with colonic wall thickening, stool PCR positive, how do you CLASSIFY severity of this disease and what is the preferred treatment?
non severe C diff. oral vac or fidaxomicin
CDI classification:
non severe >> WBC < 15, creat <1.5
severe WBC > 15 K or creat >1.5
fulminant (hypotension, ileum,megacolon)
fidaxomicin is preferred when feasible due to lower recurrence rates.
300
48 y/o f never smoked, c/w 6 months of sob and dry cough. ct showed bilateral ground glass opacities with consolidation in lower lobe, sub pleural and peribronchovascular distribution. BAL showed lymphocytosis. she completed a course of nitrofurantoin 8 months ago for uti. lung biopsy showed organizing pna pattern
what is the diagnosis and causative agent in this case?
cryptogenic organizing pneumonia. -drug induced!
nitrofurantoin is a cause of drug induced lung disease, hypersensitivity pneumonitis and chronic organizing pna patterns. other >> amiodarone, methotrexate, bleomycin and check point inhibitors.
300
58 y/o m with chrons in the terminal ileum c/w 3 weeks of lower quadrant abdominal pain + fever, ct abd showed 4 cm fluid collection adjacent to the terminal ileum with surrounding fat stranding and no free air, CRP is 180 WBC is 16K.
what is the diagnosis and what is the step by step management approach?
ASBCESS!! cover for gram negative and anaerobes. zosyn or cipro+flagyl. percutaneous drainage is preferred over immediate surgery.
surgery reserved for failure of drainage, fistulizing disease, obstruction or perforation.
300
every physician has been in a call blue, it is every resident's nightmare, but why is it call code blue???????
1960s blue was chosen because of cyanosis, the color blue patients get without o2.
400
A warfarin anti coagulated patient CHA2DS2VASc 5 requires elective hip replacement. What perioperative anticoagulation strategy do current ACC/AHA guidelines recommend, and what trial informs this recommendation?
NO BRIDGING! withhold warfarin perioperatively
BRIDGE TRIAL 2015, no reduction in thromboembolism with bridging but significant increase in major bleeding
(exemption mechanical heart valves, very recent VTE)
400
62 y/o M with bioprosthetic aortic valve comes with 3 weeks of fever. echo showed 1.2 cm vegetation on his valve and 2/3 BC came back positive for strep viridans. Apple Duke criteria, does this patient have definite IE???
bonus points if name minor criteria...
yaaaas. major criteria: positive BC > 2 and echo evidence of vegetations.
-predisposing conditions
-vascular phenomena
-immunologic phenomena
-micro evidence > single blood culture.
400
35 y/o M with HIV c.w 3 weeks cough, hypoxia. car showed bilateral perihilar ground glass opacities. LDH is 520. bronch confirms the diagnosis.
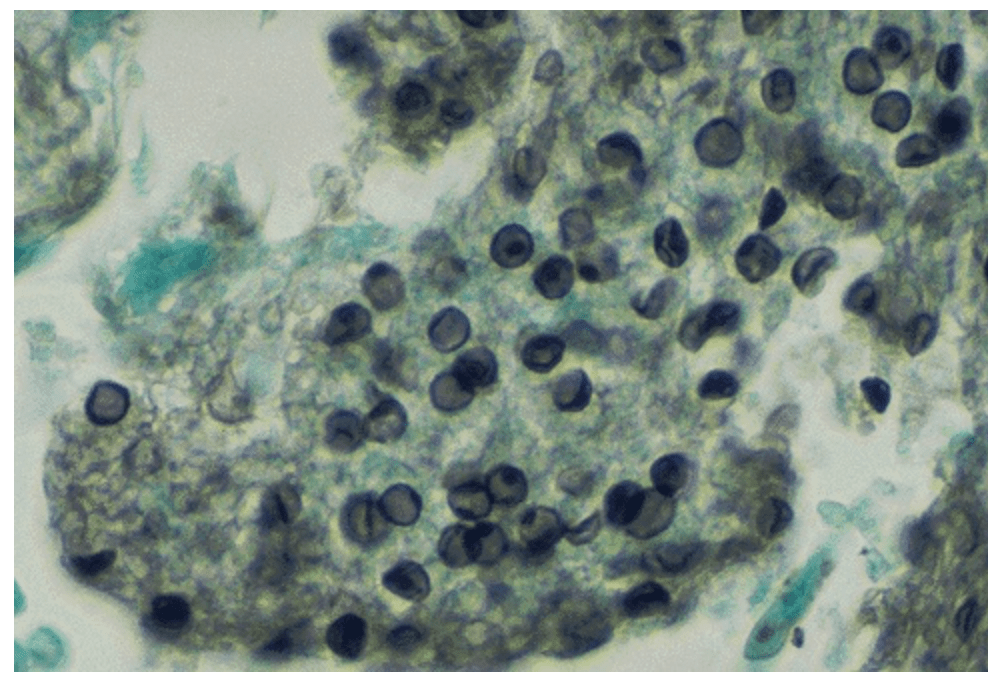
What is the diagnosis and what is this stain???
PCP pneumonia. classic presentation with elevated LDH (marker of lung injury). Aomori methenamine silver stain showed characteristic disc shaped or crescent cyst.
tx ?????
400
61 y/o M with cirrhosis c.w and distention, paracentesis showed SAAG 1.8, protein 1.4, abc 380 with 68% neutrophils but no organism on gram stain.
what is the diagnosis, treatment and intervention that reduces 90 day mortality?
Spontaneous bacterial peritonitis. PMN > 250 regardless of stain or culture. SAAG > 1.1 confirms portal hypertension. cefotaxime or ceftriaxone + IV albumin >> SORT trial >> reduces renal impairment and 90 day mortality!!!!
400
every medical students remembers their white coat ceremony. invented at a single American medical school.
name the school!!
Columbia university college of physicians and surgeons 1993!!!!!!
500
68 y/o F w/DM and HTN, c/w chest pain. EKG showed ST elevations in leads II,III,AVF, LHC showed 100% occlusion of RCA s/p stent. Once back to her room her bp drops to 80/50, HR 48, JVP elevated, lungs are clear and she is oliguric.
Which specific complication of her MI has occurred and what is the most critical management mistake to avoid?
RIGHT VENTRICULAR INFARCTION complicating inferior STEMI,
avoidddddd hypotension, nitrates, diuretics.
500
52 y.o M PMH liver transplant 8 months ago on tacrolimus, MMF, prednisone c.w headache, low grade fever and confusion. CSF was india ink positive. Cryptococcal antigen is positive in both CSF and serum, you start amphotericin and flucytosine, on day 5 he develops worsening headache, papilledema despite clinical improvement on treatment. what is this patient having??????
IMMUNE RECONSTITUION INFLAMMATORY SYNDROME!! he has sx of rising ICP despite treatment it is not treatment failure, is it paradoxical IRIS, caused by recovering immune function mounting an exaggerated inflammatory response against fungal antigens,
tx >> serials LPs until pressure is < 20
when else we can see this????
500
67 y/o M with HTN admitted for pna, cxr showed right sided pleural effusion, fluid analysis LDH 420 (Serum 210), total protein 4.8 (serum 6.2), ph 7.18, glucose 38, abc 19K with 85% neutrophils.
what type of effusion is this by lights criteria and what does the ph tells you about immediate management?
exudative by light criteria, complicated parapneumonic effusion with early empyema (ph < 7.2, glucose < 40) call CT surgery for chest tube!
light criteria
pLDH/sLDH> 0.6
pProtein/sPROTEIN > 0.5
PLDH >2/3 upper limit of normal serum LDH
500
71 y/o M addicted to ibuprofen c/w melena. he got a scope that showed 1.2 cm posterior duodenal bulb ulcer with visible vessel that is clipped.
NAME THE 4 FORREST CLASSIFICATION CATEGORIES THAT GUIDE ENDOSCOPIC INTERVENTION!!
1a and 1b oozing/bleeding, IIa non bleeding vessel >> all of these require endoscopic intervention
IIB adherent clot controversial tx
IIC pigmented spot and III clean base > medical tx
500
the joint commission banned several abbreviations fro hospital use
name 4
QD >> misread as qid
iu >> misread as IV
trailing zero 1.0 >> patients were given 10 instead of 1
naked decimal .5, misread as 5