Easy Peasy
Kidneys & Hormones
Electrolytes
Fluids/ Transportation
Acid Base Imbalances
100
•How can you prevent hyponatremia in patients with feeding tubes?
•Use normal saline instead of water for irrigation of feeding tubes to avoid diluting sodium levels in the body.
•Ensure that the patient’s fluid and sodium intake is adequately monitored.
100
What do the kidneys do in fluid balance?
•The kidneys are the primary regulators of fluid balance, adjusting the concentration of electrolytes, osmolality, blood volume, and pH.
The kidneys are controlled by hormones, the circulatory system, and the sympathetic nervous system
100
List the normal lab values for Na+, K+, Cl-, Ca+, Mg+, phosphate.

100
•What is included in the compositions of body fluids?
Water, extracellular fluid, intracellular fluid and electrolytes. 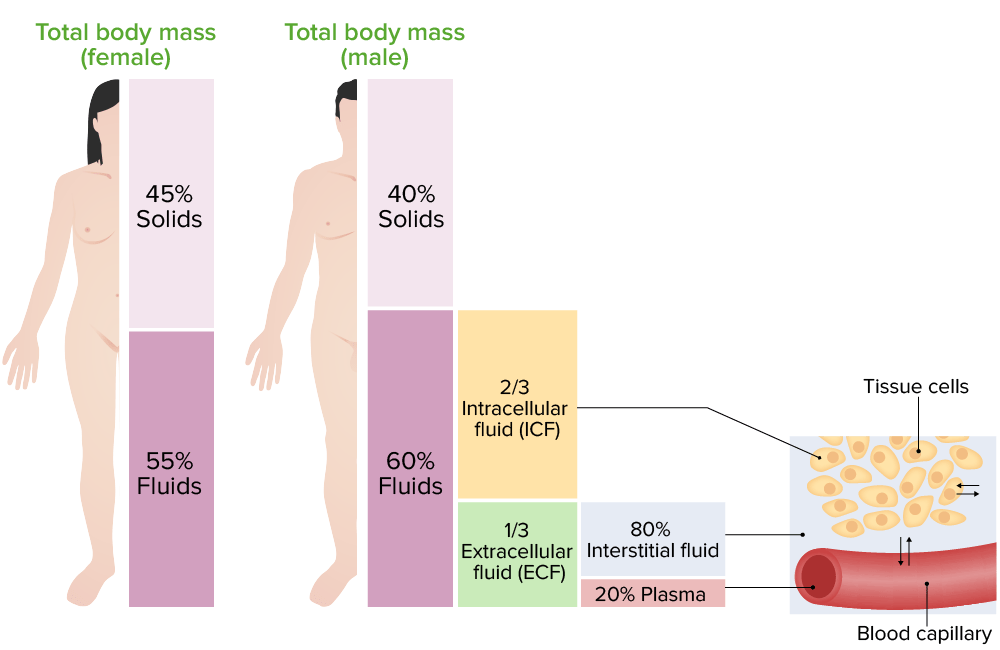
100
What does Metabolic Alkalosis involve? (cause, s/s/, tx/ nursing care)
•Metabolic Alkalosis
•Cause: Increased bicarbonate or loss of hydrogen ions.
•Causes: Vomiting, diuretics, NG suctioning.
•Symptoms: Headache, irritability, lethargy, shallow respirations, nausea, muscle weakness.
•Treatment: Correct the underlying cause.
•Nursing Care:
•Assessment: Monitor vital signs, fluid balance, and lab values.
•Interventions: Prevent electrolyte loss, provide comfort, and use isotonic saline for NG irrigation.
200
What is Fluid Volume Deficit (Hypovolemia and Dehydration):
•Occurs when body water is below normal levels.
200
•Hormones Regulating Fluid Balance Function
•Renin:
•Secreted when blood volume or pressure drops.
•Activates angiotensinogen to form angiotensin I, which is converted to angiotensin II by angiotensin-converting enzyme (ACE).
•Angiotensin II is a potent vasoconstrictor and stimulates aldosterone release, leading to sodium and water retention.
200
Difference between hyponatremia and hypernatremia involve? (cause, s/s/, tx/ nursing care)
•Hyponatremia (Sodium Deficit):
•Cause: Low sodium levels due to excess water intake or sodium loss (vomiting, diarrhea, diaphoresis).SIADH
•Risk factors: Excessive ADH secretion, heart failure, liver cirrhosis, SIADH, and certain medications.
•Symptoms: Headache, muscle weakness, fatigue, confusion, abdominal cramps, and orthostatic hypotension.
•Treatment: Fluid restriction, IV normal saline or Ringer's lactate, hypertonic sodium if below 115 mEq/L, diuretics (e.g., furosemide), sodium replacement.
•Nursing care: Administer fluids and medications, monitor intake/output, mental status, and lab results. Assist with ambulation if hypotension is present.
Hypernatremia: too much Na not enough water.
s/s: dry mouth, thirsty, swollen tounge.
tx: restrict sodium, dilute with fluids, daily weights/I&Os, lab work.
200
•What is the normal osmolality of body fluid?
•The normal range of osmolality of the body fluids is between 280 and 294 milliosmoles per kilogram (mOsm/kg).
•Osmolarity refers to the concentration of particles per liter of solution.
200
What does Metabolic Acidosis involve? (cause, s/s/, tx/ nursing care)
•Metabolic Acidosis
•Cause: Excess hydrogen ions or loss of bicarbonate.
•Causes: Starvation, dehydration, renal failure, diabetic ketoacidosis.
•Symptoms: Fatigue, confusion, vomiting, diarrhea, muscle weakness.
•Treatment: Correct underlying cause; sodium bicarbonate or Tromethamine (THAM) may be used.
•Nursing Care:
•Assessment: Monitor vital signs, mental and neurologic status.
•Interventions: Administer prescribed medications and IV fluids, reassure and orient confused patients.
300
•What is Fluid Volume Excess (Hypervolemia):
•Occurs when there is an excess of body water.
300
•Hormones Regulating Fluid Balance Function
ADH
•Antidiuretic Hormone (ADH):
•Produced by the hypothalamus and secreted by the posterior pituitary gland.
•Increases water reabsorption in capillaries, concentrating urine and reducing volume excreted.
•Release is triggered by increased plasma osmolality, hypotension, pain, stress, and certain medications.

300
Difference between hypomagnesemia and hypermagnesemia involve? (cause, s/s/, tx/ nursing care)
•Hypomagnesemia: Due to poor absorption or excessive loss (vomiting, diarrhea, alcoholism).
•Often seen with hypokalemia and hypocalcemia.
s/s: rigid muscles, possible seizures, stridor, arrythmias, DTR, mental changes, trousseaus/ Chvostek's.
Tx: Mg, check renal functions prior to admin. Seizure precautions.
•Hypermagnesemia: Often caused by excessive magnesium intake, especially in renal failure or preeclampsia. (antiacids)
s/s: Flushing/ warmth/vasodilation
•Treatment: Correct the underlying causes and provide appropriate supplementation or medications.(ventilator, dialysis, calcium gluconate)
300
What is the transport Processes:
•Diffusion:
•Diffusion:
•Movement of particles from high to low concentration.
•Example: Oxygen moves from alveoli to pulmonary capillaries.
Facilitated diffusion: Carrier proteins help molecules move without energy
300
What does Respiratory Alkalosis involve? (cause, s/s/, tx/ nursing care)
•
•Respiratory Alkalosis
•Cause: Hyperventilation leading to excessive CO2 loss and raised pH.
•Symptoms: Increased respiratory and heart rates, dizziness, irritability, tingling/numbness.
•Causes: Anxiety, fever, pneumonia, trauma, or sepsis.
•Treatment: Treat underlying cause; sedatives and controlled breathing (e.g., breathing into a paper bag).
•Nursing Care:
•Assessment: Focus on respiratory status and rate/depth of respiration.
•Interventions: Administer sedatives, reassure, encourage slow breathing.

400
•Diet is a factor in that a person urine PH, what foods make urine alkaline or acidic.
eat citrus fruits and vegetables tends alkaline urine,
eats a lot of meat tends to have acidic urine.

400
•Hormones Regulating Fluid Balance Function
Atrial Natriuretic Factor (ANF):
•Atrial Natriuretic Factor (ANF):
•Released by the atria in response to increased blood volume.
•Promotes sodium and water excretion by the kidneys, inhibits renin and aldosterone release, and causes vasodilation.
•These actions lower blood volume and reduce blood pressure.
400
Difference between hypokalemia and hyperkalemia involve? (cause, s/s/, tx/ nursing care)
•Hyperkalemia (Potassium Excess):
•Cause: High potassium levels due to decreased renal function, metabolic acidosis, or potassium supplement overdose.
•Symptoms: Bradycardia, tachycardia, muscle cramps, weakness, irritability, abdominal cramps, and decreased urine output.
•Treatment: Restrict potassium intake, IV calcium gluconate for arrhythmias, insulin and glucose, beta-agonists, sodium polystyrene sulfonate (Kayexalate), patiromer, or zirconium cyclosilicate.
•Nursing care: Monitor patients for signs of hyperkalemia, especially those with renal issues. Monitor lab results, cardiac rhythm, and adjust potassium therapy accordingly.
Hypokalemia: low potassium
causes: vomiting, NG suction, diuretic such as Lasix, not eating.
s/s: muscle cramps, weakness
Hypokalemia can cause the heart to beat irregularly, potentially leading to life-threatening arrhythmias. (ECG placement)
tx: give K+, sprilactalone, eat more potassium, remember PO k+ makes GI sick) always given dilutes and on IV pump, it will burn,. NEVER PUSH IV K+ = DEATH

400
What is the transport processes:
•Active Transport
•Active Transport:
•Carrier proteins move substances from low to high concentration.
•Requires energy (ATP).
•Example: Sodium pump moves excess sodium out of cells.
![]()
400
What does Respiratory Acidosis involve? (cause, s/s/, tx/ nursing care)
•Respiratory Acidosis
•Cause: Retained CO2 due to hypoventilation, leading to carbonic acid buildup and decreased pH.
•Causes: Pneumonia, drug overdose, head injury, chest wall injury, respiratory failure.
•Symptoms: Rapid heart rate, headache, sweating, lethargy, confusion.
•Treatment: Improve ventilation (e.g., antibiotics, bronchodilators), oxygen, and mechanical ventilation if necessary.
•Nursing Care:
•Assessment: Monitor PaCO2, observe for signs of respiratory distress (anxiety, confusion), and assess respiratory rate, depth, and rhythm.
•Interventions: Encourage fluid intake, elevate the head to 30°, and reorient confused patients.
500
List normal values for
•Diagnostic Tests for Fluid and Electrolyte Balance
•Urine Studies
(You have 5 minutes)
•Diagnostic Tests for Fluid and Electrolyte Balance
•Urine Studies
•Urine pH: Measures acidity/alkalinity. Normal: 4.5–8.0. More acidic in the morning.
•Urine Specific Gravity (SpG): Reflects urine concentration. Normal: 1.016–1.022. High indicates dehydration, low suggests excess fluid.
•Urine Osmolality: Measures dissolved particles. Normal: 250–1200 mOsm/kg.
•Urine Creatinine Clearance: Detects kidney damage. Normal: 85–125 mL/min/1.73 m² (men), 75–115 mL/min/1.73 m² (women).
•Urine Sodium: Reflects sodium intake and fluid balance. Normal 24-hour range: 40–220 mEq/24h.
•Urine Potassium: Reflects kidney function. Normal 24-hour range: 25–125 mEq/24h.
•Blood Studies
•Serum Hematocrit: Percentage of red blood cells. Increased in dehydration. Normal: 40-54% (men), 38-47% (women).
•Serum Creatinine: Indicates kidney function. Normal: 0.6–1.1 mg/dL (females), 0.7–1.3 mg/dL (males).
•Blood Urea Nitrogen (BUN): Indicates renal function and fluid status. Normal: 5–20 mg/dL (under 60), 8–23 mg/dL (over 60).
•Serum Osmolality: Measures blood concentration. Normal: 285–300 mOsm/kg.
•Serum Albumin: Helps maintain blood volume. Normal: 3.5–5.5 g/dL.
•Serum Electrolytes: Includes sodium, potassium, chloride, and calcium. Normal values:
•Sodium: 136–145 mEq/L
•Potassium: 3.5–5.1 mEq/L
•Chloride: 98–107 mEq/L
•Calcium: 8.6–10.0 mg/dL (18-60 years), 8.8–10.2 mg/dL (60+ years).
•These tests help diagnose fluid and electrolyte imbalances, assess kidney function, and guide treatment decisions.
500
•Hormones Regulating Fluid Balance Function•
Aldosterone:
•Aldosterone:
•Released by the adrenal glands in response to renin.
•Increases sodium reabsorption and decreases potassium reabsorption in the kidneys.
•Sodium retention causes water retention, acting as a volume regulator.
•Stimulated by high potassium levels or low sodium levels in the blood.

500
Difference between hypocalcemia and hypercalcemia involve? (cause, s/s/, tx/ nursing care)
•Calcium Imbalance:
•Hypocalcemia: Caused by diarrhea, low calcium/Vitamin D intake, or hypoparathyroidism. Thyroidectomy.
•Symptoms: Tingling, muscle twitches, cramps, and neuromuscular irritability. Chvostek's/ trousseaus
tx: Vit D, phosphate binders(sevelamer hydrochloride) on heart monitor.
•Hypercalcemia: Caused by excess calcium, hyperparathyroidism, or cancer.
•Symptoms: Fatigue, nausea, vomiting, and muscle weakness.
Treatment: IV fluids and medications for hypercalcemia, steroids, calcitonin, phosphate soda and fleets enema.
500
What is the transport processes:
Filtration, osmosis, osmolarity?
( You have 5 minutes to answer.)
•Filtration:
•Movement of water and solutes through a membrane from high to low pressure (hydrostatic pressure).
•Example: Fluid moves from capillaries to tissues or plasma is filtered through kidneys.
•Osmosis:
•Movement of water from a less concentrated to a more concentrated solution.
•Helps balance fluid between compartments.
•Osmolality:
•Concentration of dissolved particles per kilogram of water.
•Higher osmolality means higher solute concentration.
•Controls fluid movement between compartments (intracellular and extracellular).
•Normal body fluid osmolality: 280-294 mOsm/kg.
•Osmolarity: Used in clinical studies, refers to particle concentration per liter of solution.
500
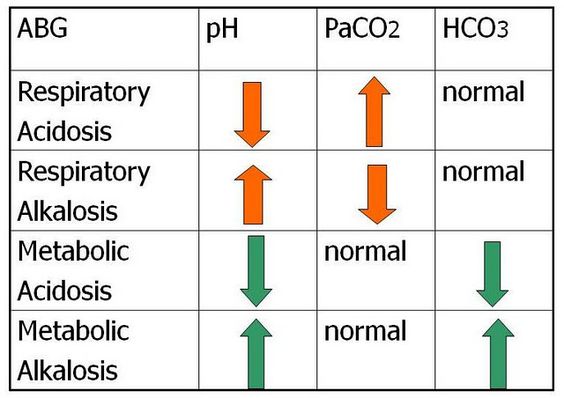
List the ABGs, pH, Paco2 and HCO3 for each acid base imbalance.
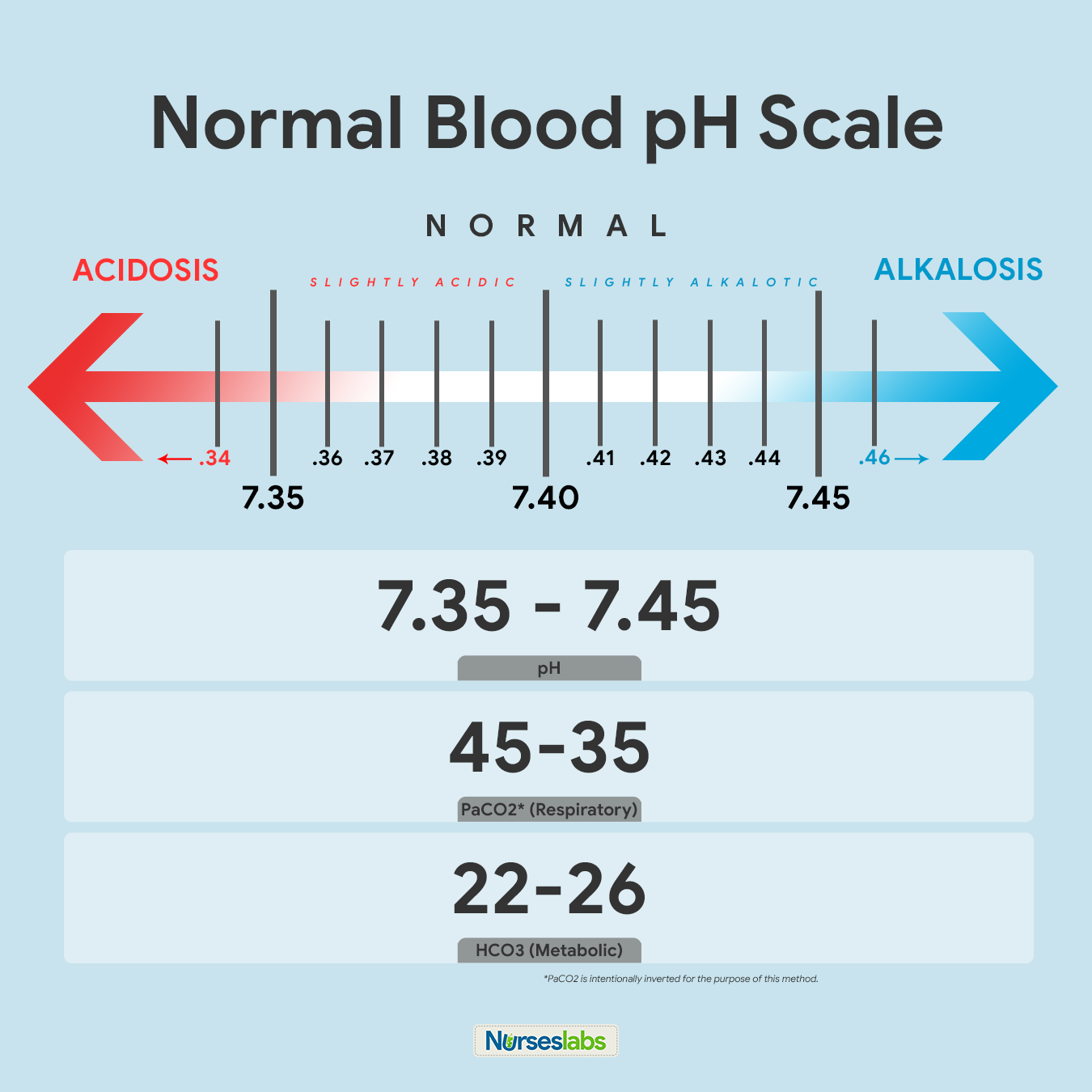
-Normal PH level?
-Normal Paco2 level?
-Normal HCO3 level?
( You have 5 minutes.)