The Sugar Diabetes
The Motherboard: Pituitary and Hypothalamus
Thyroid Time!
Adrenal(ine) rush
Endo Potpourri
100
These are the Hgb A1c cutoffs for prediabetes and diabetes. (ie, give range for prediabetes and cutoff value for diabetes)
What are:
- Prediabetes: 5.7 - 6.4%
- Diabetes: >/= 6.5%
100
Name the six hormones secreted by the anterior pituitary.
What are: Follicle-stimulating hormone (FSH), luteinizing hormone (LH), adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH), prolactin, and growth hormone (GH)?
"FLAT PiG"
100
This is the initial laboratory order to evaluate a thyroid nodule.
What is a TSH level?

100
This medication class is the treatment of choice for primary aldosteronism caused by idiopathic hyperaldosteronism (bilateral hyperplasia of adrenal glands) and in patients with aldosterone-producing adenoma who are not candidates for surgery.
What is aldosterone receptor blocker/MRA (spironolactone or eplerenone)?
Adrenalectomy is effective for unilateral disease and reduces plasma aldosterone and its attendant increased risk for cardiovascular disease. This procedure is only indicated when the adrenal vein sampling lateralizes to the adrenal that is the source of excess aldosterone production.
100
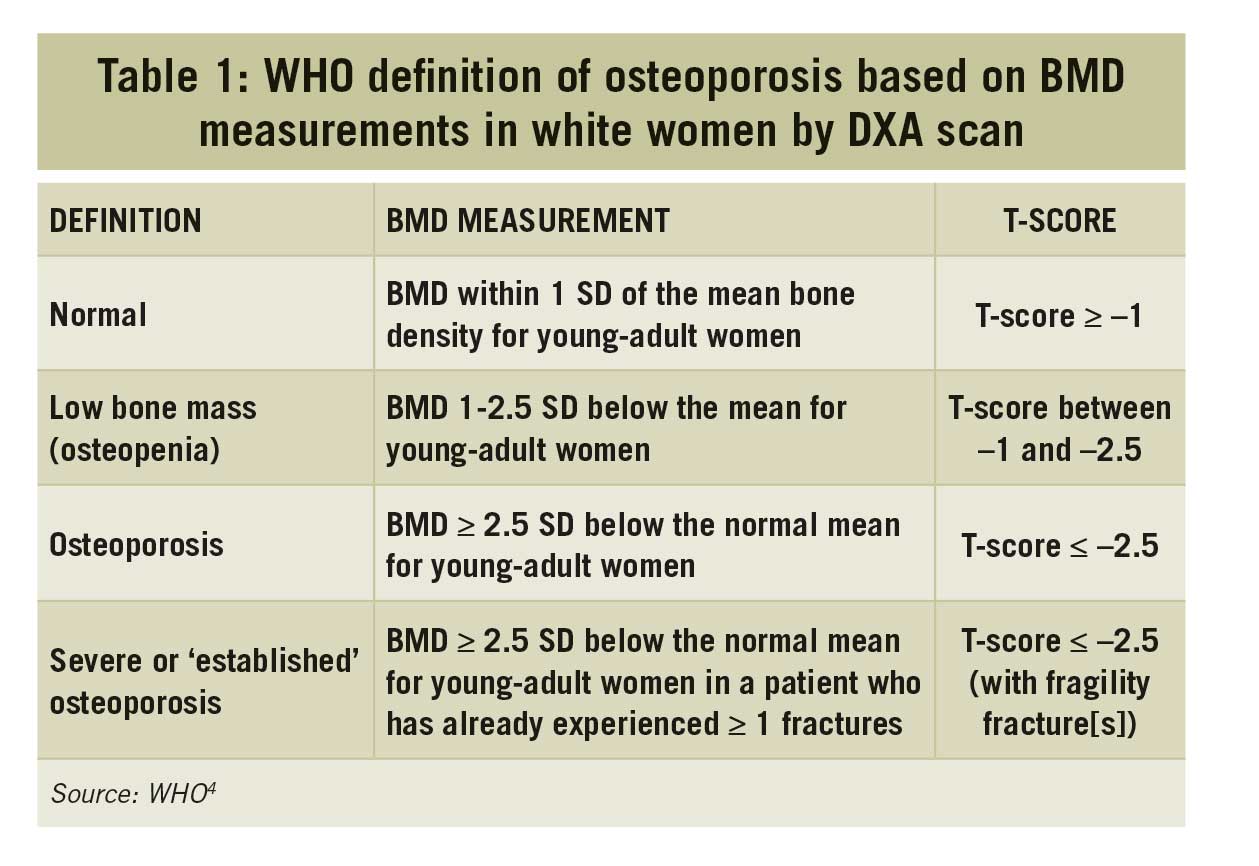
Osteoporosis is diagnosed by either ____ or ____.
What is a DEXA T-score of </= 2.5 or history of fragility fracture (fracture from a fall at standing height or lower, or fracture occurring spontaneously regardless of BMD)?
200
Both the ADA and USPSTF agree that all pregnant women should be screened for gestational diabetes at (timing -- weeks) with (test).
What is to screen all women for gestational diabetes at 24 to 28 weeks of gestation (ADA) or after 24 weeks (USPSTF) with an OGTT?
200
This endocrine emergency should be in the DDx in someone who presents with sudden headache, visual change, ophthalmoplegia, and altered mental status. Resultant from a sudden hemorrhage or infarct of this area.
What is pituitary apoplexy?
200
Fine-needle aspiration biopsy is not recommended for (this size cutoff) thyroid nodules unless associated with symptoms, pathologic lymphadenopathy, extra-thyroidal extension, history of childhood radiation exposure, or familial thyroid cancer syndrome.
What is <1cm?
FNAB is indicated for:
- all thyroid nodules ≥1 cm with suspicious sonographic features and a normal TSH level
- nodules <1 cm in patients with risk factors for thyroid cancer or suspicious ultrasound characteristics
200
This is the radiologic cutoff criteria for an adrenal incidentaloma that requires no additional follow-up imaging.
What is a homogeneous mass, density </= 10 HU, any size?

200
This is the most appropriate diagnostic test to perform on a 57-year-old woman who is evaluated for enlargement of her hands and feet. Medical history is significant for HTN. Her only medication is amlodipine.
On physical examination, vital signs are normal. BMI is 24. The patient has a wide nose and enlargement of hands and feet. Prognathism is noted.
What is insulin-like growth factor 1 (IGF-1)?
An insulin-like growth factor-1 level is the best screening biomarker for the diagnosis of acromegaly. Fewer than 5% of patients with GH excess have a GH-releasing hormone-secreting tumor or neuroendocrine tumor.
In patients with an elevated insulin-like growth factor-1 level, the diagnosis of acromegaly can be confirmed with an oral glucose tolerance test.
300
In the management of DKA:
- This is the target range for glucose levels:
- This is the cutoff level of K+ when insulin should be held/not started (until repletion administered):
- This is the cutoff in pH before considering given bicarbonate:
What is:
- Glucose between 150-200
- K <3.5 when you'd hold insulin (or not start it) pending repletion [ideal range 4.0 - 5.0]
- pH <7.0 is when you'd consider sodium bicarbonate (100 mEq in 400 mL of sterile water infused every 2 h to increase the pH to >7.0)
300
A 32yo F w/ PMHx Cushing disease s/p transsphenoidal resection and irradiation has secondary hypothyroidism. This is the appropriate lab to trend, and the range to target, while titrating thyroid replacement therapy.
What is free T4 (thyroxine) to be in the mid- to upper-half of normal range?
After an adjustment in levothyroxine dose, the free T4 level can be rechecked in 2 to 3 weeks.
300
This is the preferred medical management for a 26yo F with Graves Disease who is planning to become pregnant. (Give medication preference and timing within pregnancy course)
What is propylthiouracil (PTU) within the first trimester?
Methimazole has been linked to esophageal or choanal atresia and aplasia cutis (a congenital skin defect), with a twofold increased risk of major fetal malformations compared to propylthiouracil exposure in the first trimester.
Some clinicians transition to methimazole after the first trimester because propylthiouracil can cause rare but clinically significant hepatotoxicity.
300
These are the upper and lower limits on an 0800AM serum cortisol level that exclude and confirm, respectively, adrenal insufficiency. Indeterminate levels between these values should be followed up with this test.
What is an 0800AM cortisol <3 μg/dL confirms cortisol deficiency and values >15 μg/dL exclude the diagnosis?
For nondiagnostic cortisol values, what is stimulation testing with synthetic ACTH (cosyntropin)? A stimulated serum cortisol >18 μg/dL excludes adrenal insufficiency.

300
The Rotterdam Criteria state that in order to diagnose PCOS, you must have at least 2 criteria (name 2 of possible 3).
What are: clinical or biochemical hyperandrogenism, ovulatory dysfunction (oligomenorrhea/amenorrhea), or polycystic ovaries on ultrasound?
Must exclude other causes: thyroid dysfunction, hyperprolactinemia, nonclassical CAH, Cushing Syndrome
400
In a consensus statement, the ADA and KDIGO recommend adding this class/specific medication for patients with T2DM, normal K levels, an eGFR of 25 or greater, and persistent albuminuria (alb-Cr ratio >/= 30mg/g) despite maximally tolerated doses of ACE inhibitors or ARBs to reduce the risk for CKD progression.
What is a nonsteroidal mineralocorticoid receptor antagonist (finerenone)?
Steroidal MRAs (spironolactone and eplerenone) reduce albuminuria but lack evidence for kidney disease progression outcomes and carry higher hyperkalemia risk, particularly with reduced kidney function. Guidelines reserve steroidal MRAs for heart failure, hyperaldosteronism, or refractory hypertension rather than for diabetic kidney disease management.
400
A hospitalized patient develops polyuria of 75 mL/kg/24 hours (normal: <50 mL/kg/24 hours). Labs show:
Serum sodium: 151 mEq/L (normal: 135–145 mEq/L)
Serum osmolality: 308 mOsm/kg (normal: 275–295 mOsm/kg)
Urine osmolality: 90 mOsm/kg (normal: ~300–900 mOsm/kg, depending on hydration status)
After administration of desmopressin, the urine osmolality rises significantly.
This condition best explains the patient’s findings.
What is arginine vasopressin deficiency (central diabetes insipidus)?
400
This somewhat common over-the-counter supplement can cause falsely high free T4, free T3, total T4, and total T3 along with falsely low TSH -- mimicking thyrotoxicosis.
What is biotin?
Patients taking more than 5 to 10 mg/day of biotin, a common over-the-counter supplement, should discontinue it 2 to 5 days before thyroid function testing.
400
Name 3 indications (clinical/radiologic/etc) to test for a pheochromocytoma/paraganglioma.
Possibilities:
1) Adrenergic-type spells (headache, sweating, and tachycardia) with or without hypertension
2) Incidentally discovered adrenal mass with unenhanced CT attenuation >10 HU
3) Resistant hypertension (>140/90 mm Hg) on three-drug therapy including a diuretic
4) Hypertension with onset age <20 years
5) Idiopathic cardiomyopathy
6) Hypertensive episode induced by anesthesia, surgery, or angiography
7) Paraganglioma
8) Familial syndromes that predispose to pheochromocytoma or paraganglioma: VHL, SDHx mutation, NF-1, CSD, and MEN2
9) Family history of pheochromocytoma or paraganglioma
400
What ancient Greek physician used to diagnose patients with diabetes by tasting their urine?
Who is Hippocrates (no, not Bear Grylls)?
500
In the workup for fasting hypoglycemia in a person without DM, provide the following:
- A prolonged fast, up to this time period, should be initiated
- During the fast, plasma glucose levels should be checked at this time interval
- If glucose levels drop to <60 mg/dL, these four tests should be ordered/trended
What are:
- Prolonged fast up to 72 hours
- During the fast, glucose levels to be checked q6hr
- If plasma glucose <60, should order: C-peptide, insulin, proinsulin, and beta-hydroxybutyrate

500
This is the minimum screening recommendation for a pregnant patient with a known pituitary macroadenoma. (Include test and frequency)
What is visual field testing each trimester?
Headaches or visual field changes should prompt a non-contrast pituitary MRI to evaluate for change in tumor size.
Surgical tumor debulking before pregnancy or continuing dopamine agonist therapy (preferably bromocriptine) throughout pregnancy may be required in these patients. If surgery during pregnancy is necessary, the second trimester is the preferred time.
500
A 68yo F is admitted to ICU for urosepsis. PMHx notable for hypothyroidism, but no levothyroxine is present on med rec.
Vitals: T 93.2F, BP 90/40, HR 64, RR 8, and SpO2 90% (RA)
PE: periorbital edema, 3+ pitting edema in BL LE's, absent deep tendon reflexes, lethargic and slow to respond to questions
Labs: Na 130, TSH 29, free T4 0.1, serum cortisol 21
This is the most appropriate medical management (include recommended dosing).
Myxedema coma:
What is IV Levothyroxine? Loading dose of 200-400μg, followed by an oral dose of 1.6 μg/kg/d.
Oral levothyroxine administration is inappropriate because the severe hypothyroidism may cause bowel edema and slowed oral absorption of levothyroxine.
Steroids can be held if random serum cortisol level >18μg.
500
Describe the timing and dosing for an overnight dexamethasone suppression test in someone you have concerns for cortisol excess. Include the post-dexamethasone cortisol level cutoff value that is considered positive.
(Bonus 100pts: These types of medications can lead to false-positive values)
1mg Dexamethasone is given at 11 PM and serum total cortisol is measured at 8 AM the following morning.
A post-dexamethasone cortisol level of greater than 1.8 μg/dL (49.7 nmol/L) is considered a positive result. (Normal would be <1.8)
Bonus: False-positive results may occur with concomitant use of medications (carbamazepine, phenytoin, pioglitazone) that induce hepatic cytochrome P-450 3A4 enzymes and accelerate dexamethasone metabolism.
500
What are the names of the cells in the testes that are stimulated by FSH and LH specifically to induce spermatogenesis?
What are Sertoli and Leydig cells?