General Principles
Resuscitation
Trauma
Medical Emergencies
Special Populations
100
Which of the following is a goal of Crew Resource Management (CRM)?
Provide a way for the team leader to direct the decision-making process.
Promote teamwork based on open communication between team members.
Identify ways to divide tasks so each team member has time to rest.
Train individuals to rely on their own experiences when planning missions.
Promote teamwork based on open communication between team members.
Comments: Team communication or lack thereof was identified as a contributor to aircraft accidents in the 1970’s. CRM was designed to mitigate that threat. All other answers are components of CRM, but are not the goals. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 70
100
The flight nurse is preparing to transport a patient to a trauma center. The patient has received 12 units of packed red blood cells in the last hour. The nurse should anticipate administration of:
platelets.
calcium gluconate.
sodium bicarbonate.
cryoprecipitate.
calcium gluconate.
Comments: Massive transfusions can cause hypocalcemia due to the citrate included in the blood products. The flight nurse should be aware that calcium levels should be monitored and replacement calcium be given. Although the other options may be warranted, hypocalcemia should be addressed immediately. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 206
100
The nurse arrives on the scene of a motor vehicle collision and assesses the passenger of a vehicle that was hit from the right side. The patient is tachypneic, tachycardic, and hypotensive. Breath sounds are diminished on the right side. EMS has placed a non-rebreather mask and SPO2 is 89%. What is the most appropriate intervention?
Increase FiO2
Needle decompression of the right chest wall
Prepare for rapid sequence intubation
Apply non-invasive positive pressure ventilation.
Needle decompression of the right chest wall
Comments: The patient is displaying signs of tension pneumothorax. Needle decompression is the immediate lifesaving intervention. Rapid sequence intubation would not be indicated prior to needle decompression. Non-invasive positive pressure ventilation is contraindicated in a patient with a tension pneumothorax. Increasing FiO2 will not improve oxygenation if the tension pneumothorax is not treated. _____Reference: https://www.ncbi.nlm.nih.gov/books/NBK441885/
100
The flight nurse is receiving a victim of a lightning strike from a Basic Life Support unit. The patient is breathing and has a rapid pulse. Which immediate life threat should the flight nurse be MOST concerned for?
Third degree burn
Internal bleeding
Hyperkalemia
Lethal arrhythmia
Lethal arrhythmia
Comments: The immediate life threats from lightening strikes are lethal dysthymias and/or respiratory arrest. Hyperkalemia may manifest within 8 hours of injury. Third degree burns and internal bleeding are life threatening injuries, however a lethal arrhythmia will cause death if not treated immediately. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 280
100
An infant with dehydration and sepsis is being transported for admission to the ICU. Which of the following findings would indicate the need for further fluid resuscitation?
tachycardia
flat fontanelle
urine output of 2 mL/kg/hr
apneic episodes
tachycardia
Comments: Tachycardia is an early sign of hypovolemia. Infants can only increase cardiac output by increasing heart rate. They cannot increase stroke volume. A flat fontanelle is incorrect because in a dehydrated infant the fontanelle would be sunken rather than flat. A flat fontanelle is a normal finding. A urine output here is incorrect because a urine output of 2 mL/kg/hr indicates normal fluid volume status. Apneic episodes are incorrect because apneic episodes are not an indication of volume depletion. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 524
200
In a helicopter safety and landing zone (LZ) presentation to a local EMS service, which of the following is the MOST important instruction for EMS personnel?
Utilize ambulance lights to highlight the LZ.
Approach only from the loading side of the helicopter.
Ensure LZ is at least 200' x 200'.
Proceed toward the aircraft only when directed by the pilot.
Proceed toward the aircraft only when directed by the pilot.
Comments: The EMS scene call environment is one of the most potentially hazardous aspects of air medical operations. Safety is of paramount importance and situational awareness must be maintained when working around an aircraft. Ground personnel should only be allowed to approach the aircraft when directed to do so by the pilot or a flight crew member. The pilot in command of the aircraft must be able to see personnel approaching. Mitigating the hazard from air medical operations on ground personnel is the most important instruction. The LZ can be a minimum of 100' x 100'. While some situations may require lighting the landing zone, the MOST important instruction for EMS personnel should be to approach only when directed. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 105-106
200
The flight nurse is transporting a patient with 40% second degree, high voltage electrical burns. The patient weighs 85 kg. According to the recommended American Burn Resuscitation guidelines, initial fluid resuscitation over 8 hours should be:
13.6L
6.8L
4.0L
8.0L
6.8L
Comments: Patients suffering from high voltage electrical burns need to be resuscitated using the fluid calculation of 4ml x kg x % burn. The first half of the resuscitation should occur over 8 hours, with the second half of the resuscitation occurring in the following 16 hours. An isotonic fluid is recommended, with lactated ringer's being the recommended choice. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 281
200
A patient who leaped from a third story window and landed on his feet presents with bilateral lower extremity fractures. What other injury is MOST likely in this patient?
acetabular fractures
wrist fractures
pelvic fracture
lumbar fractures
lumbar fractures
Comments: Lumbar and also thoracic spinal column fractures should always be ruled out in falls or axial loading injuries. Kinetic energy produced by the person's body traveling through space and a sudden deceleration of the body against an immovable object/surface is concentrated in an area of the thoracic or lumbar spine. This axial loading causes the vertebral structures to fracture and subluxate/move. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 246-247
200
The flight team is called to transport a patient diagnosed with pericarditis. It is reported that the patient has sharp chest pain and a pleural friction rub. Upon initial assessment, the pulses are diminished peripherally during inspiration, and return during exhalation. The most likely cause of this is:
Aortic dissection
Tension pneumothorax
Pericardial effusion
Pulmonary embolism
Pericardial effusion
Comments: A main complication of pericarditis is pericardial effusion. Typically pericarditis will present without paradoxical pulses (decreased pulses on inspiration). Paradoxical pulses, in conjunction with other supporting clinical signs like distended veins, muffled heart sounds, and hypotension should make the flight nurse suspect pericardial effusion has developed. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 310
200
When postpartum hemorrhage is identified, the transport nurse should immediately
perform bimanual uterine compression.
place the patient in the Trendelenburg position.
massage the fundus.
administer magnesium sulfate.
massage the fundus.
Comments: The transport nurse should immediately massage the fundus. Fundal massage in the setting of postpartum hemorrhage causes the uterine muscles to contract and this greatly decreases bleeding. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 445
300
A patient receiving mechanical ventilation is noted to have an increased respiratory rate after engine start. The flight nurse knows the PRIORITY intervention is
administer sedation.
abort the start up.
reposition the patient.
restrain the patient.
administer sedation.
Comments: When the engine starts up, the patient experiences vibration, a normal flight stressor. The patient might require more sedation with the increased sensory input. It is not necessary to restrain the patient or abort the startup unless the patient is a danger to themselves or the crew. Repositioning is not indicated in this situation. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 37
300
A transport team is transporting an adult patient with type 1 diabetes mellitus who presents to the emergency department with a one day history of polydipsia, polyuria, vomiting, and generalized weakness. Laboratory results are as follows:
serum sodium 128 mEq/L
serum potassium 3.2 mEq/L
serum chloride 94 mEq/L
serum glucose 550 mg/dL
serum calcium 8.8 mg/dL
blood urea nitrogen (BUN) 40 mg/dL
creatinine level 1.3 mg/dL
CO2 14 mEq/L
The flight nurse should prepare to administer which medication FIRST?
potassium chloride
calcium chloride
regular insulin
sodium bicarbonate
potassium chloride
Comments: Potassium chloride should be administered first. Potassium Chloride: Low serum potassium occurs as insulin promotes the return of potassium into the cell and metabolic acidosis is reversed. The potassium level must be 3.3 mEq or greater before insulin therapy is initiated. The potassium level must be checked frequently as insulin drives potassium into the cell, and serum potassium can drop precipitously. Potassium chloride is administered as soon as the serum potassium level drops below normal. Frequent potassium verification is required while the patient is receiving fluid resuscitation and insulin therapy. Regular Insulin: If serum potassium is greater than 3.3 mEq, then regular insulin is initiated IV at a rate of 0.1 unit/kg/h (in conjunction with a normal saline fluid bolus) to achieve a 50-70 mg/dL decline in glucose level per hour. The insulin drip is titrated each hour to achieve/maintain this rate of glucose level decline. When the glucose level is at 200 mg/dL, the insulin drip is decreased to 0.05-0.1 units/kg/h. Sodium Bicarbonate: Adequate IVF hydration and insulin replacement usually corrects the acidosis related to DKA. Administration of sodium bicarbonate is no longer routine therapy except for severely acidotic patients with a pH less than 7.0. Calcium Chloride: Calcium chloride is not indicated in the initial treatment of DKA. _____Reference: Critical Care Nursing: Diagnosis & Management, 8th Ed. (2018), p. 735-740
300
The flight nurse arrives on scene of an accident where the patient fell 20 feet. Vital signs are as follows:
BP 80/40 mmHg
HR 55 beats/min
RR 24 breaths/min (shallow)
O2 sat: 93% on a nonrebreathing mask
The nurse should recognize that the PRIORITY medication to administer is
atropine.
dexamethasone (Ozurdex).
norepinephrine (Levophed).
morphine.
norepinephrine (Levophed).
Comments: The patient has lost vascular tone due to a probable spinal cord injury, and is in neurogenic shock. The priority is not pain management. Steroids are not indicated. Atropine is not the appropriate medication for neurogenic shock. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 208
300
A 49-year-old patient complains of chest pain during transport. The 12 lead ECG reveals ST elevation in all 12 leads. The flight nurse suspects this is a STEMI imposter due to
hyperkalemia.
digoxin toxicity.
left bundle branch block.
pericarditis.
pericarditis.
Comments: The hallmark of acute pericarditis is widespread ST-segment elevation. A right bundle branch block will result in ST elevation in V1, and hyperkalemia will present with peaked T waves. Digoxin toxicity can lead to a number of dysrhythmias but not widespread ST elevation. _____Reference: Ismail T. F. (2020). Acute pericarditis: Update on diagnosis and management. Clinical medicine (London, England), 20(1), 48–51. https://doi.org/10.7861/clinmed.cme.20.1.4
300
The flight nurse notes that noise from the aircraft has caused a 70-year-old patient who is being mechanically ventilated to become agitated. Which of the following should the nurse administer for further sedation?
rocuronium (Esmeron)
ketamine (Ketalar)
lorazepam (Ativan)
midazolam (Versed)
ketamine (Ketalar)
Comments: Elderly patients can have paradoxical excitation with benzodiazepines and caution should be used. A paralytic is not indicated in this situation. Ketamine can provide a safer alternative for sedation. _____Reference: Sheehy's Manual of Emergency Care, 7th Edition (2013), p. 584
400
During radio transmission of a patient report, the flight nurse should
remain brief, speaking clearly and concisely.
verbalize head-to-toe assessment findings.
relay the patient's name and date of birth.
release the microphone at every pause.
remain brief, speaking clearly and concisely.
Comments: Brief, clear and concise messages are components of effective communication. Head-to-toe assessments affect brevity of communication. HIPAA protected identifiers should not be transmitted over non-secure lines. ______Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 62
400
The flight team is preparing to transport a patient in septic shock who is receiving high-dose norepinephrine (Levophed). The flight nurse understands that, at higher doses, norepinephrine can:
Increase bronchial dilation
Decrease cardiac output
Improve preload
Dilate peripheral arterioles
Decrease cardiac output
Comments: High dosages of norepinephrine result in marked vasoconstriction which can decrease cardiac output in a heart unable to pump against the increased afterload. Norepinephrine has no effect on bronchial dilation or preload and it constricts peripheral arterioles rather than dilating them. _____Reference: Critical Care Nursing: Diagnosis & Management, 8th Ed. (2018), p. 411
400
A patient who sustains bilateral femur fractures in a motor vehicle crash is being transferred to a tertiary center. Examination reveals petechiae on the chest and increasing shortness of breath with an oxygen saturation of 87% on a nonrebreathing mask. The patient is at significant risk for
systemic inflammatory response syndrome.
fat embolism syndrome.
pulmonary contusion.
acute respiratory distress syndrome.
fat embolism syndrome.
Comments: Patients with long bone fractures (e.g. femur) should be monitored for shock and are at highest risk of fat embolism. Signs and symptoms of fat embolism are petechial rash and hypoxemia. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 266
400
The nurse responds to the scene of a sporting event. The patient is abnormally tall, has long arms and is complaining of burning chest pain. Lung sounds are clear and there is no jugular vein distention. Vital signs are as follows:
BP: 230/140 mmHg
HR: 109 beats/min
RR: 30 breaths/min
O2 sat: 96% (room air)
The PRIORITY action for the nurse is to
start an esmolol (Brevibloc) infusion.
administer fentanyl (Duragesic).
place nitroglycerin paste (Nitro-Bid).
initiate a fluid bolus.
start an esmolol (Brevibloc) infusion.
Comments: The patient likely has Marfan syndrome and is experiencing an aortic dissection. The treatment is aggressive blood pressure and heart rate management with a beta-blocker and rapid transport to a surgical center. While management should include fentanyl, it is not the priority intervention. Fluids should be avoided. Nitroglycerin (Nitro-Bid) is not the first-line agent for aortic dissection. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 311
400
When administering medications to the geriatric patient population, the flight nurse understands that:
The patient is less sensitive to medication, so larger doses should be administered.
The patient has increased kidney function, so smaller doses should be administered.
The patient has less fat reserves, so larger doses should be administered.
The patient's liver function is lower, so lower doses should be administered.
The patient's liver function is lower, so lower doses should be administered.
Comments: The older adult generally has lower function of end organs and increased fat reserves. Medications should be given carefully as they will not be metabolized as quickly as in the younger adult population. _____Reference: Critical Care Nursing: Diagnosis & Management, 8th Ed. (2018), p. 1005
500
Which of the following BEST describes the result of sympathetic dysfunction in a patient who has a spinal cord injury?
vasodilation
areflexia
hyperreflexia
spastic paralysis
vasodilation
Comments: Vasodilation best describes this result. Vasodilation is the result of interruption of sympathetic outflow below the level of the injury and loss of auto regulation. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 243
500
The transport nurse is preparing to transfer a patient with left ventricular heart failure. Preload reduction is BEST accomplished with morphine, diuretics, and which of the following medications?
nicardipine (Cardene)
metoprolol (Lopressor)
nitroglycerine (Tridil)
nitroprusside (Nipride)
nitroglycerine (Tridil)
Comments: Nitroglycerin produces a vasodilator effect on the peripheral veins and arteries with more prominent effects on the veins. Primarily reduces cardiac oxygen demand by decreasing preload (left ventricular end-diastolic pressure). Metoprolol inhibits beta receptors, causing a decrease in heart rate. It does not affect preload. Nicardipine inhibits calcium from entering the slow channels, thereby causing relaxation of coronary vascular smooth muscle and coronary vasodilation. It does affect preload. Nitroprusside causes peripheral vasodilation by direct action on venous and arteriolar smooth muscle, thus reducing peripheral resistance and will increase cardiac output by decreasing afterload. _____Reference: Rosen's Emergency Medicine: Concepts & Clinical Practice, 9th Edition (2018), p. 981
500
A patient with an unstable pelvis was found 6 hours after falling down a ravine and is being evacuated from the scene via helicopter. They were placed on oxygen at 6 L/min via nasal cannula and have the following vital signs:
BP 80/45 mm Hg
HR 98 beats/min
RR 32 breaths/min
02 Sat 100%
ETCO2 22 mm Hg
The flight nurse recognizes this patient is MOST likely suffering from:
neurogenic shock.
permissive hypotension.
anaerobic metabolism.
pulmonary contusion.
anaerobic metabolism.
Comments: The low ETCO2 value coupled with vital signs consistent with shock are indicative of a patient in anaerobic metabolism. Neurogenic shock is incorrect because in neurogenic shock bradycardia would be expected. Permissive hypotension is incorrect because there is no indication of an intentional choice to not resuscitate the patient. Pulmonary contusion is incorrect because with a pulmonary contusion it is unlikely the oxygen saturation would be 100% on 6 L. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 198-203
500
A patient with a head injury is being transported with an extraventricular drain in place. The transport nurse notes a sustained intracranial pressure (ICP) elevation. The following waveform is observed:
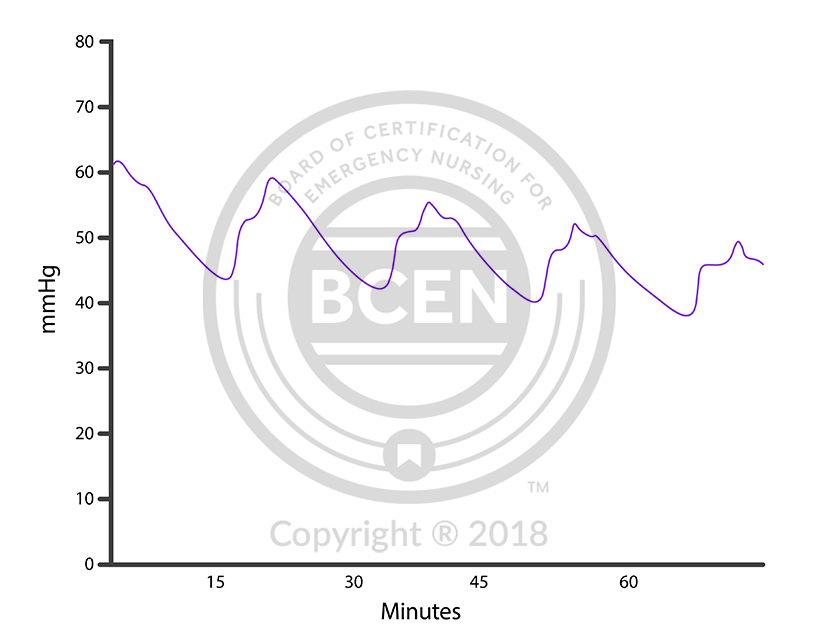
Which of the following is the nurse's BEST action?
Nothing; this is only a temporary spike and should resolve on its own.
Allow cerebrospinal fluid to drain until an acceptable pressure is noted.
Administer mannitol (Osmitrol) 0.5g/kg over 20 minutes.
Elevate the head of bed more than 60 degrees.
Allow cerebrospinal fluid to drain until an acceptable pressure is noted.
Comments: In this patient with intracranial hypertension, the Monroe-Kellie hypothesis describes that drainage of cerebrospinal fluid via the intraventricular catheter will provide an immediate and direct reduction of that pressure. A 60-degree elevation is too much. This would cause an erroneous reading and would need to be re-leveled since the ventriculostomy drain is calibrated to the ventricle. These are "A" waves. They are indicative of severe increasing ICP and will not resolve on their own. Mannitol (Osmitrol) is a possible treatment, but this action takes too much time. _____Reference: AACN Procedure Manual for High Acuity, Progressive and Critical Care, 7th Ed. (2017), p.835-840
500
Specialized transport methods in an isolette are especially important for neonates because
specialty flight teams are covered by separate training and licensure that traditional flight teams do not carry.
traditional flight teams do not regularly interact with neonates.
isolettes provide specialized oxygen concentrations not available through traditional stretcher transport.
neurodevelopmental complications can be caused by excessive vibration and noise.
neurodevelopmental complications can be caused by excessive vibration and noise.
Comments: Infants that are exposed to excessive noise and vibration are at risk for negative physiological responses, increased stress, and neurological damage. Isolettes alone do not provide specialized oxygen concentrations or pressurization. Licensure and training play a role in the need for a specialty team, but should not be a deciding factor for using an isolette. _____Reference: ASTNA Patient Transport: Principles and Practice, 5th Ed. (2018), p. 485