Protecc
Anatomy
Rhytidectomy
Parotidectomy
Rando
100
Most commonly injured nerve in rhytidectomy
What is the greater auricular nerve?
100
Must be answered by a medical student without coaching: The facial nerve runs through this skull-base foramen
What is the stylomastoid foramen?
100
Skin flaps are longer in this type of rhytidectomy?
SMAS rhytidectomy versus deep rhytidectomy
(3-4 cm for deep versus 7-8 cm for SMAS)
100
Name the facial nerve divisions that course superiorly and inferiorly after division at the pes anserinus.
100 extra points to team with any members who know what pes anserinus means in latin.
After it exits the stylomastoid foramen, the main trunk of the facial nerve gives off branches to the posterior belly of the digastric muscle and then runs through the parenchyma of the parotid tissue. It divides into an upper temporofacial division and a lower cervicofacial division at the pes anserinus, which is located approximately 1 to 2 cm from the stylomastoid foramen.
100
A rare disorder characterized by usually bilateral non-progressive facial paralysis and the inability to abduct one or both eyes due to impairment in the facial (VII) and the abducens (VI) nerves.
What is Moebius syndrome?
200
Most commonly injured motor nerve in rhytidectomy (with branch)
What is the zygomatic branch of the facial nerve (travels in loose areolar connective tissue over zygomatic arch), superficial to periosteum.
200
These two parts of the auricle provide touch sensation via somatic sensory fibers of the facial nerve.
Somatic sensory fibers provide sensation to touch of the EAC and conchal skin of the auricle, as well as proprioceptive information from the facial muscles.
200
With regard to the superior-most portion of the modified Blair incision, incision planning differs in this way for female and male patients.
Behind tragus for females, in front of tragus for males to avoid dragging hair onto the tragus.
200
If facial nerve is sacrificed during parotidectomy, name the two most common donor nerves for cable grafting.
What are the sural nerve and posterior auricular nerve?
200
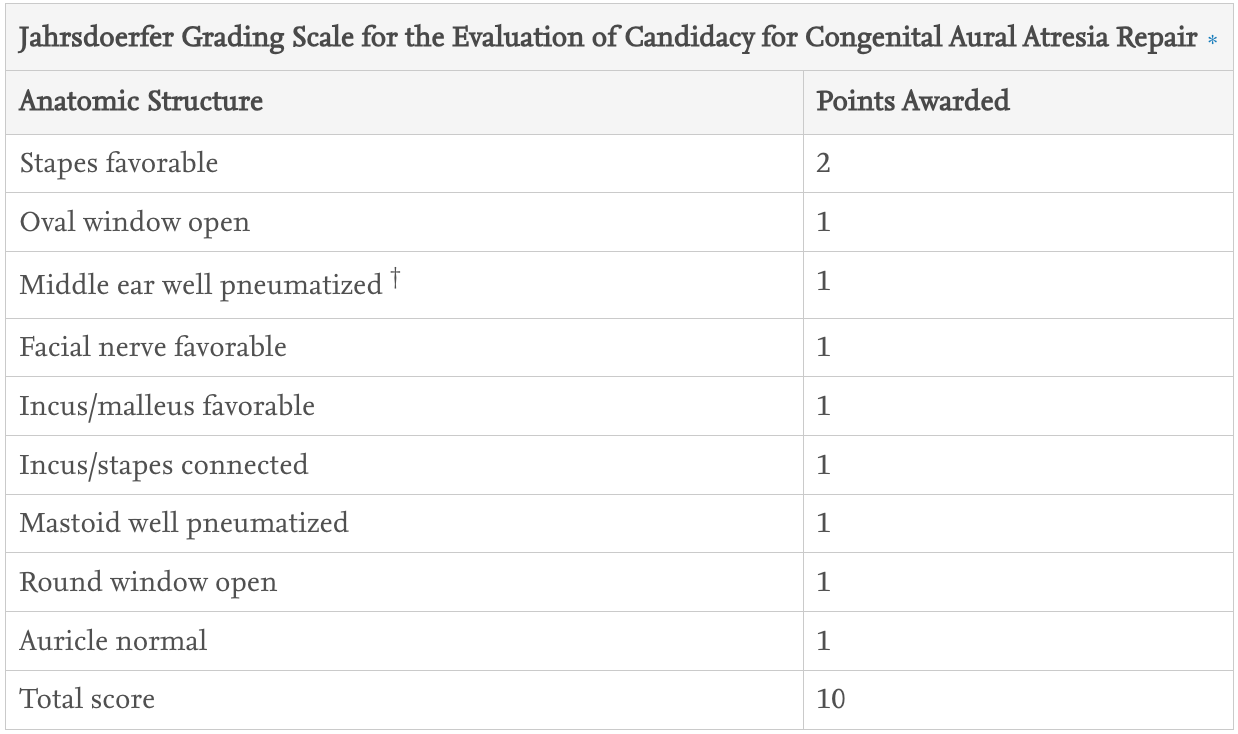
Name the total number of points available in the Jahrsdoerfer Grading Scale for the Evaluation of Candidacy for Congenital Aural Atresia Repair and the number of points awarded for favorable facial nerve position.
(Must correctly state both for points)
300
This eponymous maneuver involves ligation of the posterior facial vein and superior reflection of the investing fascia below the mandible to preserve the marginal mandibular nerve.
The Hayes-Martin maneuver involves ligation of the posterior facial vein and superior reflection of the investing fascia below the mandible to preserve the marginal mandibular nerve
300
Name the facial nerve segments from emergence from the brainstem to the five main motor branches.
This must be answered by the junior-most resident on the team who may be coached prior to answering but not during.
Cisternal, meatal, labyrinthine, tympanic, mastoid, extratemporal (temporal, zygomatic, buccal, marginal mandibular, cervical)
300
Risk of temporary or permanent facial nerve injury from rhytidectomy as cited in Cummings.
Final Jeopardy style question, both teams write both figures on paper, closest team wins.
Temporary: 7%
Permanent: 0.4-2.6%
300
Name the most likely diagnosis: Patient with a long-standing parotid mass that suddenly undergoes rapid growth over a period of several months, with facial nerve paralysis.
Carcinoma ex-pleomorphic adenoma
300
The facial nerve originates as the nerve of this pharyngeal arch alongside which other nerve.
Must name pharyngeal arch and nerve for points.
The facial nerve (CN VII) primarily develops between the 3rd and 8th weeks of gestation as the nerve of the second pharyngeal arch. It emerges alongside the vestibulocochlear nerve (CN VIII) and innervates all structures derived from this arch, including the muscles of facial expression, the stapedius, and the posterior digastric.
400
Describe favorable facial nerve position relative to the oval window in pre-operative consideration for atresiaplasty.
(Superior, inferior, medial, or lateral)
In favorable anatomy, the facial nerve will lie superior to the oval window in its transverse portion. It will then turn inferiorly at the second genu to pass inferiorly through the mastoid cavity in the vertical portion. In unfavorable cases, the facial nerve may totally or partially cover the oval window and stapes, obscuring the view and thus precluding a surgical approach to the window.
400
Facial muscles which receive facial nerve innervation from the superficial aspect rather than the deep.
Must get all three to receive points.
What are levator anguli oris, buccinator, and mentalis?
400
With regard to deep plane versus SMAS facelift techniques, this vector can be greater achieved by deep-plane facelifting.
What is the vertical vector, specifically in the mid face. Deep plane facelifting is superior in addressing the melolabial fold.
400
Name the triad of essential landmarks for identification of the main trunk of the facial nerve.
Can only earn points for question if not assisted by a PGY-5 during formal response.
Tragal pointer - nerve is 1cm anterior and inferior, mean distance 13.6mm
Tympanomastoid fissure/suture - MOST CONSISTENT, facial nerve is 3.8-4.9mm medial and inferior to the lateral aspect, from here follow to foramen
Posterior belly of digastric - nerve trunk lies at the levee of the superior attachment of muscle to digastric ridge, mean distance 8.8-14.6mm
400
This specific area of the facial nerve is hypothesized to produce a disproportionate number of facial nerve neoplasms due to embryologic diversity.
What is the geniculate ganglion?
Sensory components from hyomandibular epibranchial placode, supporting cells NCC origin
500
Which of these waves when observed during surgery is shown to be correlated with poor post-operative outcomes with regard to the facial nerve?
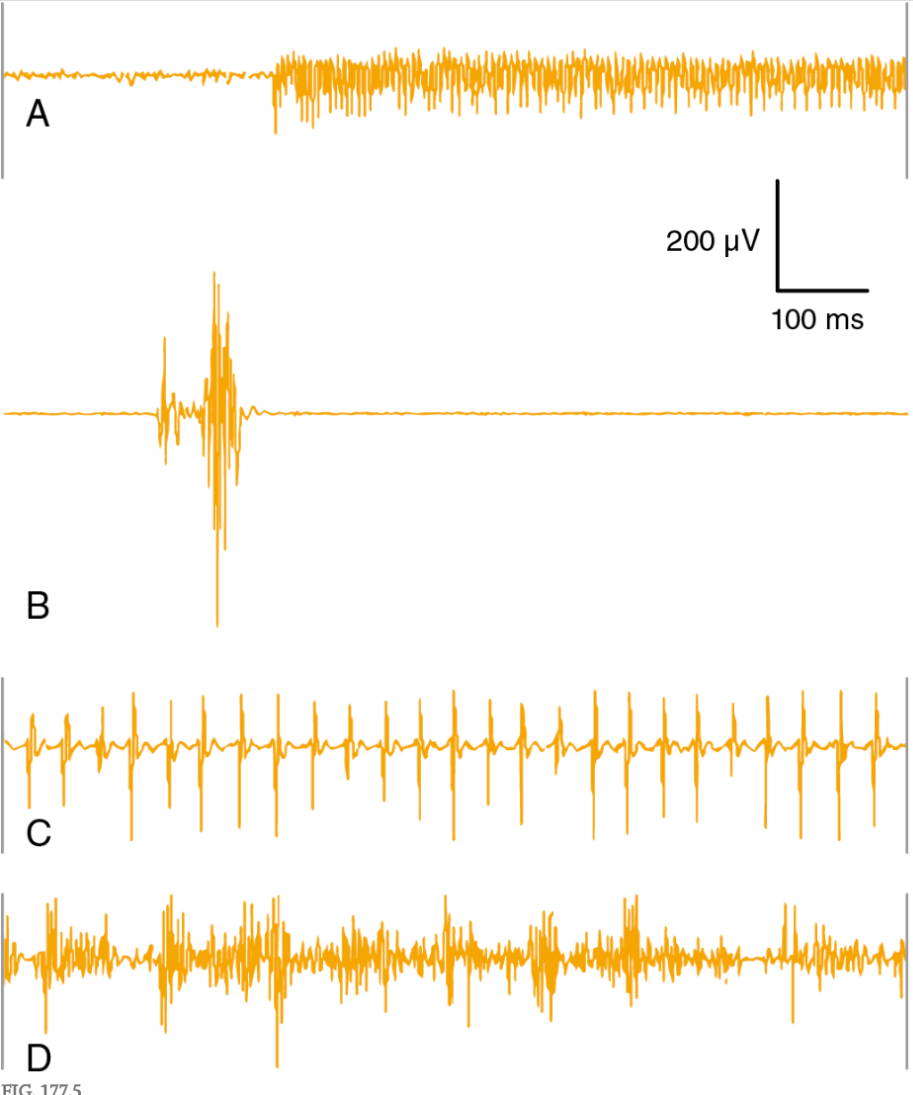
(A) A sudden-onset, high-frequency A-train showing a sinusoidal pattern, which is often associated with nerve stretch and the only pattern that was found to correlate with poor postoperative outcome. (B) Phasic (transient) burst activity typically associated with direct contact with the nerve. (C) A pattern of repetitive spikes at relatively regular intervals, known as a B-train. (D) A pattern of irregular high-frequency train activity with variable amplitude, known as a C-train that is usually benign and often encountered during irrigation of the surgical field.
500
This facial nerve segment is at greatest risk of damage in vestibular schwannoma resection.
The cisternal portion of the facial nerve between the brainstem exit zone and the porus of the IAC is the portion of the nerve at the highest risk of damage because of the splayed nature of the facial nerve in this segment and its adherence to the tumor capsule. Furthermore, precise location of the facial nerve relative to the tumor in this portion is difficult to predict. To achieve improved tumor resection rates while minimizing trauma to the facial nerve, the “inferior long-axis (ILA) facial nerve dissection” technique has been described because it allows for both visual and electrophysiologic identification of the cisternal portion of the nerve in large tumors.
500
This ear deformity results when inadequate peri-lobular skin is left after rhytidectomy

What is a satyr ear deformity?
500
Describe how the marginal mandibular branch of the facial nerve can be identified for retrograde identification of the facial nerve.
This branch can be found by carefully dissecting superiorly along the posterior facial vein. This can be useful when the location of the parotid tumor makes it difficult to identify the facial nerve at its main trunk. The marginal mandibular branch can be traced retrograde to the main trunk in these situations.
500
1901 in Berlin, Germany, on a Polish Aristocrat by Dr. Eugene von Hollander
What is the year, location, patient and surgeon who were reported to have been involved in the first recorded rhytidectomy?