Labs/Tests
Medications
100
This blood test commonly ordered in those presenting with fatigue, weight gain, and cold intolerance measures a hormone that is made in the pituitary gland.
What is a TSH Test?
The symptoms described in the prompt are consistent with hypothyroidism. TSH is commonly ordered to aid in diagnosis of hypo or hyperthyroidism. A high TSH level is usually associated with hypothyroidism while a low TSH is associated with hyperthyroidism. A free T4 test is added if pituitary or hypothalamic disease is suspected. Additionally, if the patient is symptomatic but has a normal TSH level, a free T4 level should be measured.
100
This common drug overdose results in fatigue.
What are opiates?
Drug activation of the pre-synaptic opioid receptor decreases Ca2+ influx in response to action potential. This decreases the release of excitatory NTs, such as glutamate. Activation of the post-synaptic receptor increases K+ efflux and decreases the response of the post-synaptic neuron to excitatory NTs. This is the mechanism by which opioids cause central CNS depression, leading to fatigue, lethargy, and sedation.
200
Which of the following causes of fatigue can be determined with an ESR?
A. Pregnancy
B. Infections mono
C. Anemia
D. Polymyalgia rheumatica
E. All of the above
E. All of the above
ESR is nonspecific test that can show an increase in all of the above conditions.
200
Explain how anti-epileptic drugs cause fatigue.
Anti-epileptic drugs acting to increase the GABAergic activity have the highest incidence of fatigue via CNS depression (with tiagabine as an exception), followed by Gabapentin and Levetiracetam. In contrast, drugs mainly inhibiting sodium channels (Carbamazepine, Eslicarbazepine, Lamotrigine, Phenytoin and Valproate) have the lowest incidence of fatigue as a side effect.
300
A 26 year old female presents to the clinic with worsening fatigue over the past month. She reports a 7lb increase in weight and frequent urination. Her last menstrual cycle was around 3 weeks ago she thinks and states that she usually has irregular flows. She is sexually active with her boyfriend and they use condoms irregularly. What are tests that you can reasonably order to help your diagnosis?
A. Pregnancy test
B. CBC
C. Blood glucose
D. TSH
E. All of the above
E. All of the above
All of these tests are indicated for this patient. She is sexually active with infrequent condom use and of child bearing age. She has fatigue with a history of irregular periods. She has frequent urination and weight gain.
300
A 67-year-old woman visits her physician and reports new-onset fatigue and drowsiness. One month earlier, she was prescribed a new antihypertensive medication. Her temperature is 37.1°C (98.7°F), pulse is 78/min, and blood pressure is 113/75 mm Hg. Findings on physical examination are unremarkable.
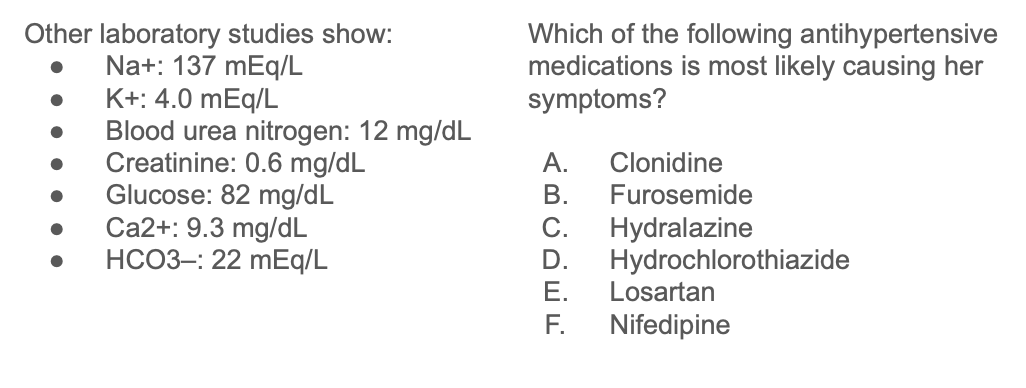
A. Clonidine
This patient presents with new-onset fatigue and drowsiness. These symptoms arose after she began taking a new drug for hypertension. This drug is most likely clonidine, a central α2-receptor agonist. Because clonidine is a centrally acting drug, it affects vessel tone indirectly and does not usually change a patient’s electrolyte profile. Additionally, because it is centrally acting, many of the adverse effects are related to central nervous system (CNS) depression. These symptoms include fatigue, drowsiness, and headaches.
Furosemide, hydrochlorothiazide, losartan, nifedipine, and hydralazine are not typically associated with strong CNS depression. Additionally, furosemide, hydrochlorothiazide, and losartan exert some (or all) of their effects at the kidney tubules, so electrolyte abnormalities are possible.
400
Lab test results affect the outcome for patients presenting with fatigue how much of the time?
A. 5%
B. 10%
C. 35%
D. 50%
E. 75%
A. 5%
Evidence shows that when a patient comes in for fatigue, lab test results indicate the cause of the fatigue only 5% of the time.
400
A 45-year-old man presents to the clinic with severe back pain, muscle weakness, and fatigue. The patient denies any recent trauma or extraneous activity. The patient reveals he recently stopped taking a medication that he was prescribed 2 years ago to treat a hormone imbalance. Prior to starting the physical examination, the patient complains of being cold and nauseated. The patient's blood pressure is 94/68 mm Hg, temperature is 98.6° F (37° C), respiratory rate is 17/min, and pulse is 102/min. Physical examination reveals darkened oral mucosa. A basic metabolic panel revealed hyponatremia and hyperkalemia.
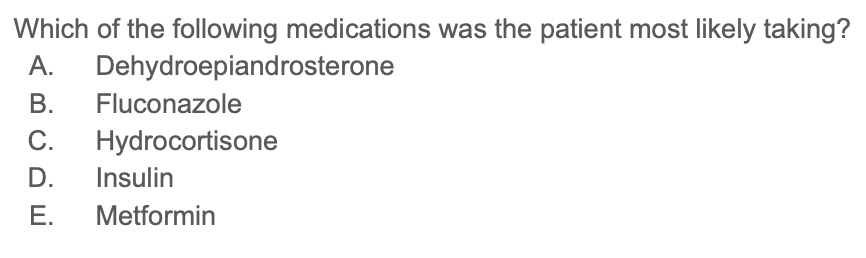
C. Hydrocortisone
The patient has an adrenal crisis secondary to sudden medication withdrawal for his history of adrenal insufficiency. Treatment includes oral hydrocortisone. Adrenal crisis is an emergency precipitated by the sudden cessation of hydrocortisone therapy, due to the rapid decrease in cortisol levels. The predominant manifestation of adrenal crisis is shock, and it must be treated immediately with a hydrocortisone injection.
Adrenal crisis is a medical emergency, and is precipitated by the sudden cessation of hydrocortisone therapy used to treat adrenal insufficiency. The predominant manifestation of adrenal crisis is hypotension, hyponatremia, hyperkalemia and symptoms of extreme fatigue and muscle pain.
Dehydroepiandosterone (DHEA) is an androgen replacement therapy sometimes used in combination with glucocorticoids or mineralocorticoids to treat Addison disease. DHEA withdrawal does not, however, precipitate Addisonian crisis. Abrupt withdrawal of the antifungal fluconazole can lead to headache, rash, gastrointestinal disturbances and hepatitis. Stopping metformin, a biguanide, can cause diarrhea, headache, hypoglycemia, and weakness. Stopping insulin replacement therapy can cause hyperglycemia.
500
A 58-year-old man comes to his physician because of progressive fatigue. He first noticed the tiredness around 1 year ago but just associated it with his increasing age. The past 4 months have been increasingly worse, and he's found it difficult to complete his long days as a janitor. He has a medical history significant for hypertension and dyslipidemia and admits to mostly a fast food based diet. He has a 20-pack-year smoking history and drinks occasionally with his friends. His temperature is 98.6° F (37° C), blood pressure is 135/82 mm Hg, pulse is 98/min, and respiratory rate is 17/min. Examination reveals mild lower abdominal discomfort and a capillary refill of 3 seconds.
What initial lab test will best explain the fatigue and what is his most likely diagnosis?
A. CMP - pancreatitis
B. CMP - hepatitis
C. ESR - colon cancer
D. CBC - colon cancer
E. CBC - diverticulitis
D. CBC - colon cancer
His history suggests that he is a risk for colon cancer and is showing signs of anemia which is commonly seen in undiagnosed colon cancer The best test to determine this would be a CBC
500
A 48-year-old woman with a history of peptic ulcer disease and gastroesophageal reflux disease comes to her primary care physician because she has not felt like herself lately. She reports fatigue, weakness, and feeling more “down” than she ever has before. She also complains of experiencing constipation for the past few days. She has been regularly taking medication for her peptic ulcer disease over the past few years.
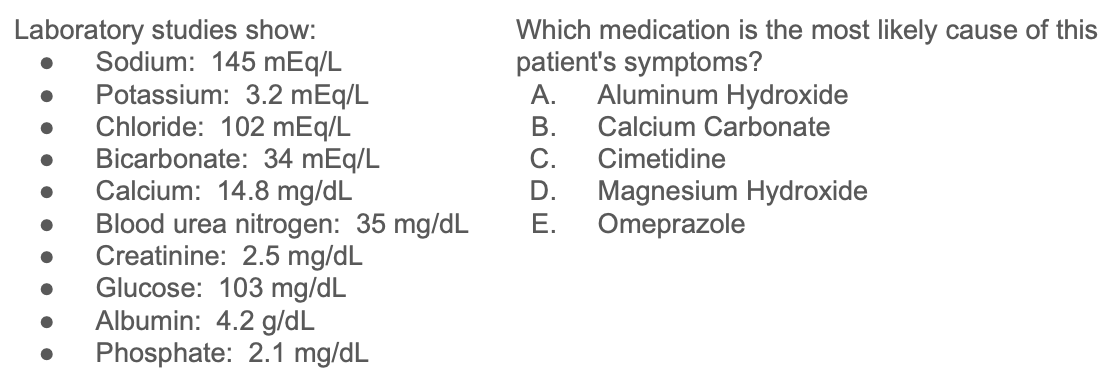
B. Calcium carbonate
Patients who have overused calcium carbonate for long periods may develop milk-alkali syndrome, which includes symptoms of hypercalcemia (depression, constipation, weakness, fatigue), metabolic alkalosis, and renal insufficiency. In addition, long-term overuse of calcium carbonate can lead to rebound gastric acid hypersecretion.
Physical symptoms of hypercalcemia, including fatigue, muscle weakness, depressed mood, and constipation. Labs show elevated calcium level, in addition to low potassium and phosphate levels. These are hallmarks for milk-alkali syndrome. Calcium carbonate, an over-the-counter antacid, is a common cause of hypercalcemia and milk-alkali syndrome (with signs of hypercalcemia, metabolic alkalosis, and renal insufficiency).
Discontinuation of the antacid is typically sufficient to resolve mild cases of hypercalcemia and milk-alkali syndrome. If antacid use continues, severe renal complications (eg, nephrolithiasis) can occur. Overuse of any antacids can change the bioavailability of other drugs by affecting urinary and gastric pH.
Cimetidine is an antihistamine that can cause tiredness and is used for symptomatic relief of gastroesophageal reflux disease (GERD), but it would not cause hypercalcemia.