My Achy Breaky Heart
The Clot Thickens
Bug Out
Bean Bros
Here be Dragons
100
After PCI with DES:
How long is DAPT recommended for?
Chronic CAD: 6 to 12 months DAPT -> Monotherapy
ACS: 12 months -> Monotherapy
*Shorter Duration for High Risk of Bleed*
*PRECISE-DAPT Score: Risk of Bleed
*DAPT Score: Prolonged DAPT > 12 months
100
In Acute PE, give at least 3 features, or lack thereof, that are consistent with a safe outpatient treatment course?
1. Low Risk Score (PESI, Hestia, BOVA)
2. Negative cardiac biomarkers
3. Negative RV strain
4. Does not need supplemental oxygen
100
Extended infusions is useful for antibiotics that exhibit ________ dependent MOA
Time Dependent (-cidal or static)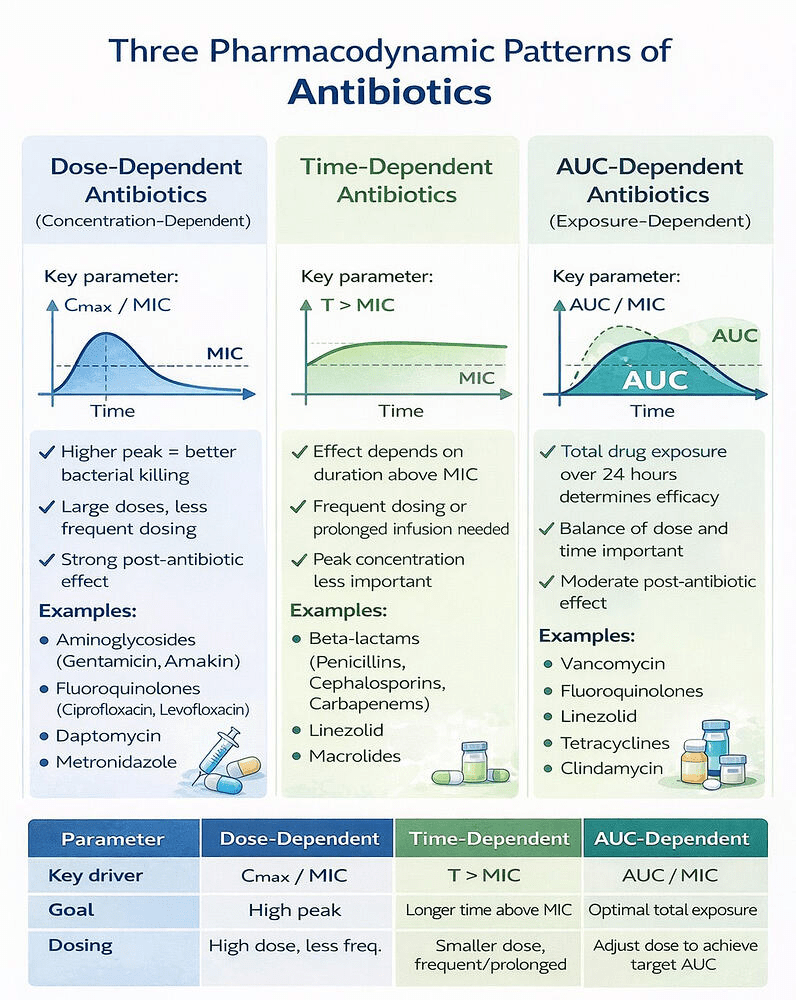
100
CKD
Name the GFR thresholds for CKD3, CKD4, CKD5, and ESRD
CKD3a: 45 to 59
CKD3b: 30 to 44
CKD4: 15 to 29
CKD5: <15
ESRD: RRT or need for transplant (CKD5 + RRT)
100
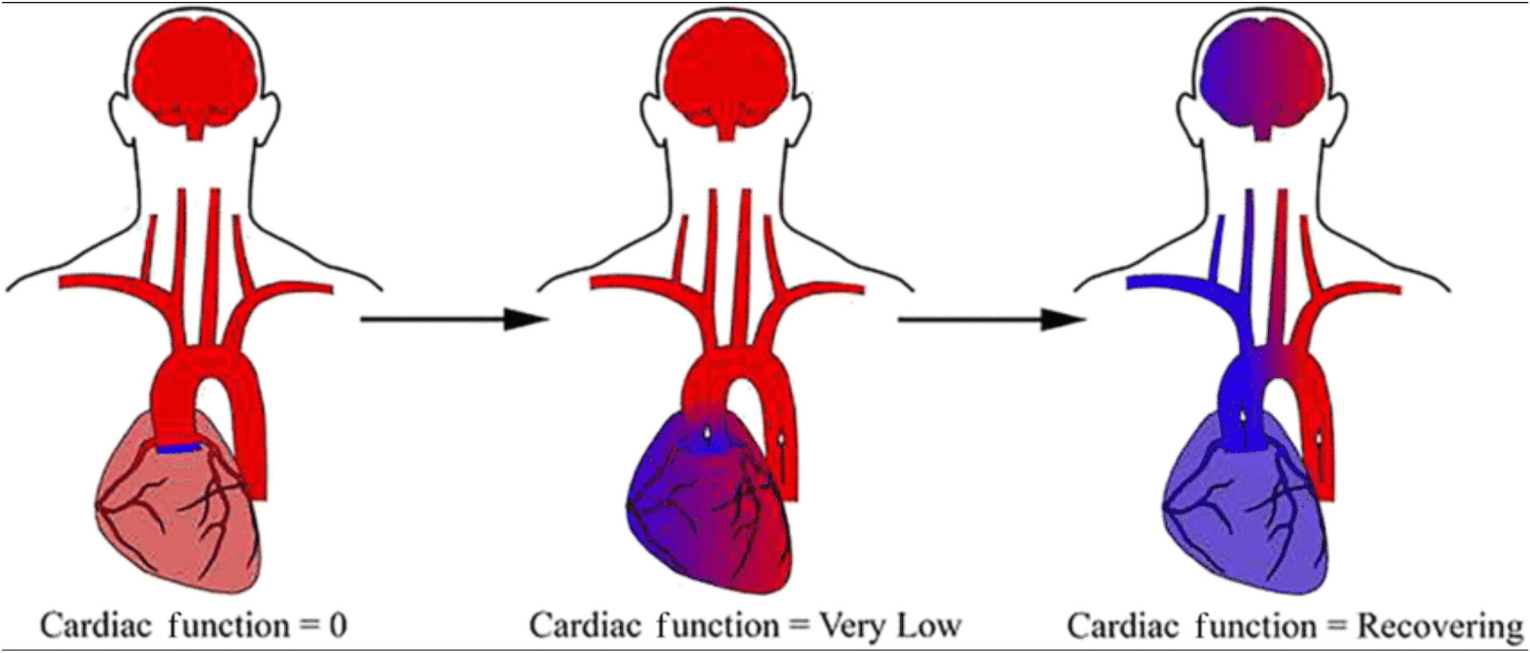
Name this ECMO "Sign" and describe its physiology and what pt will look like if you do nothing (aside from dead)

Harlequin Sign of VA ECMO
Evidence of cardiac recovery -> DANGEROUS!
200
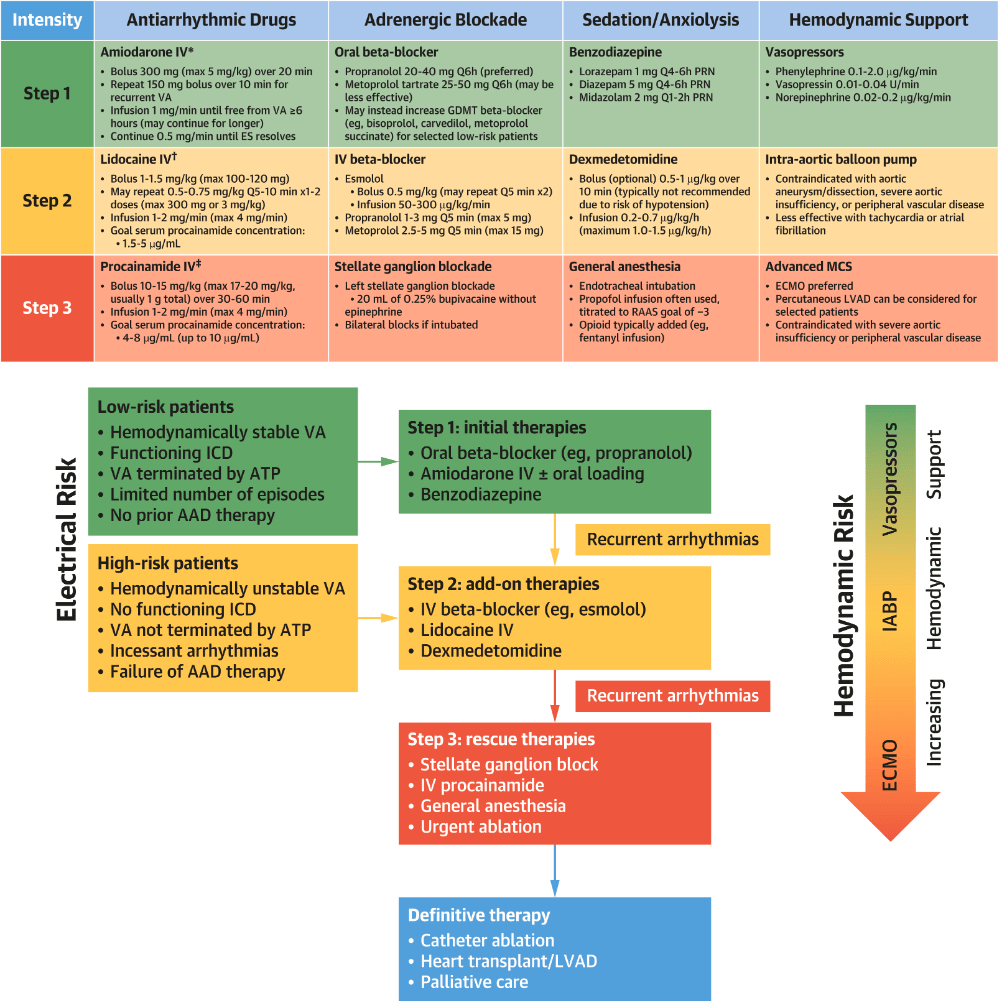
Wide Complex Tachycardia
This condition is defined as at least 3 episodes of VT or VF within 24 hours
VT/VF Storm
200
In PE, what constitutes "Hypotension" or Hemodynamic Instability (Give at least 2 parameters)
SBP < 90mmHg or drop >39 mmHg for at least 15 minutes
SBP < 90mmHg + End organ hypoperfusion
Requirement for Vasopressors to keep SBP > 90
*Watch for Normotensive Shock*
200
Assuming an extended infusion strategy, when would you choose 4.5g over 3.375g, every 8 hours?
1. Pseudomonas aeruginosa
2. Other nosicomial PNA
3. Febrile Neutropenia (NCCN rec q6 hours, std infusion rate?)
4. Hyperfiltration (N. ICU, Sepsis, Trauma, Preg)
200
This eGFR is the minimum need to START an SGLT2i, such as Jardiance
eGFR > or = 20 is needed to start SGLT2i
It is reasonable to continue this medication if eGFR drops < 20
200
ABG: pH 7.20|pCO2 20|paO2 90| SpO2 95%
BMP: HCO3 = 12, AGAP 24
What is the secondary acid base disturbance
Compensation by Winter's Formula
PaCO2 = 1.5 * (HCO3) + 8 +-2
Expected paCO2 = 24-28, actual 20
***Concurrent Respiratory Alkalosis
300
In ACS:
Name at least 3 contraindications to early BB use...
1. 1st deg AVB (PR >0.24)
1a. Unpaced 2nd or 3rd Degree AVB
2. Active Bronchospasm
3. Hypotension +/- Shock (including AMI-CS)
4. Severe Bradycardia
5. ACS due to Cocaine
7. Acute Heart Failure
300
In Ischemic Stroke, Individuals can receive thrombolytics up to 9 hours if THIS (type) imaging shows salvageable tissue
AHA 2026 Stoke GL
Individuals with DWI-FLAIR imaging showing mismatch (i.e. salvagable penumbra)
"absence of a clearly visible, or marked, hyperintense signal in the same region on FLAIR as DWI"
Exclusions: NIH >25, Contraindications, > 1/3 MCA
300
What organism can fulfill (IE) mDUKE Major Clinical criteria from a single blood culture?
1. Coxeilla burnetii
Other "Typical Organisms" include
Stapylococci, Strepococci, Enterococci, HACEK
(Hemophilus, Aggregatibacter, Cardiobactium hominis, Eikenella, Kingella)
300
Constellation of HLD, profound Edema, heavy proteinuria, and a renal vein thrombosis should raise suspicion of what disease process?
Classically: Membranous Nephropathy, anti-PLA2R
Also Consider: FSGS and Class V Lupus Nephritis
300
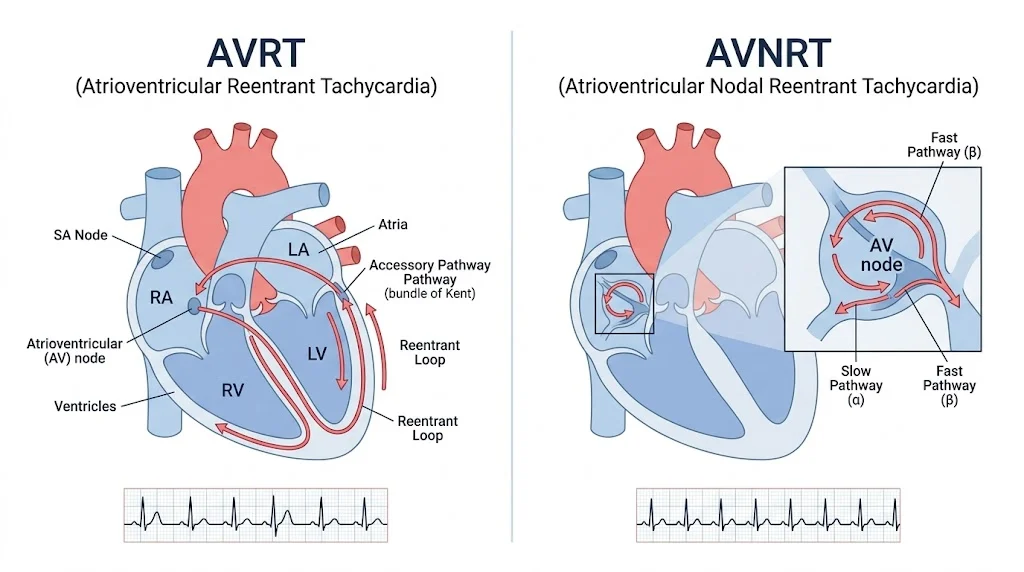
Described the differences between AVRT vs AVNRT in terms of conduction pathway
400
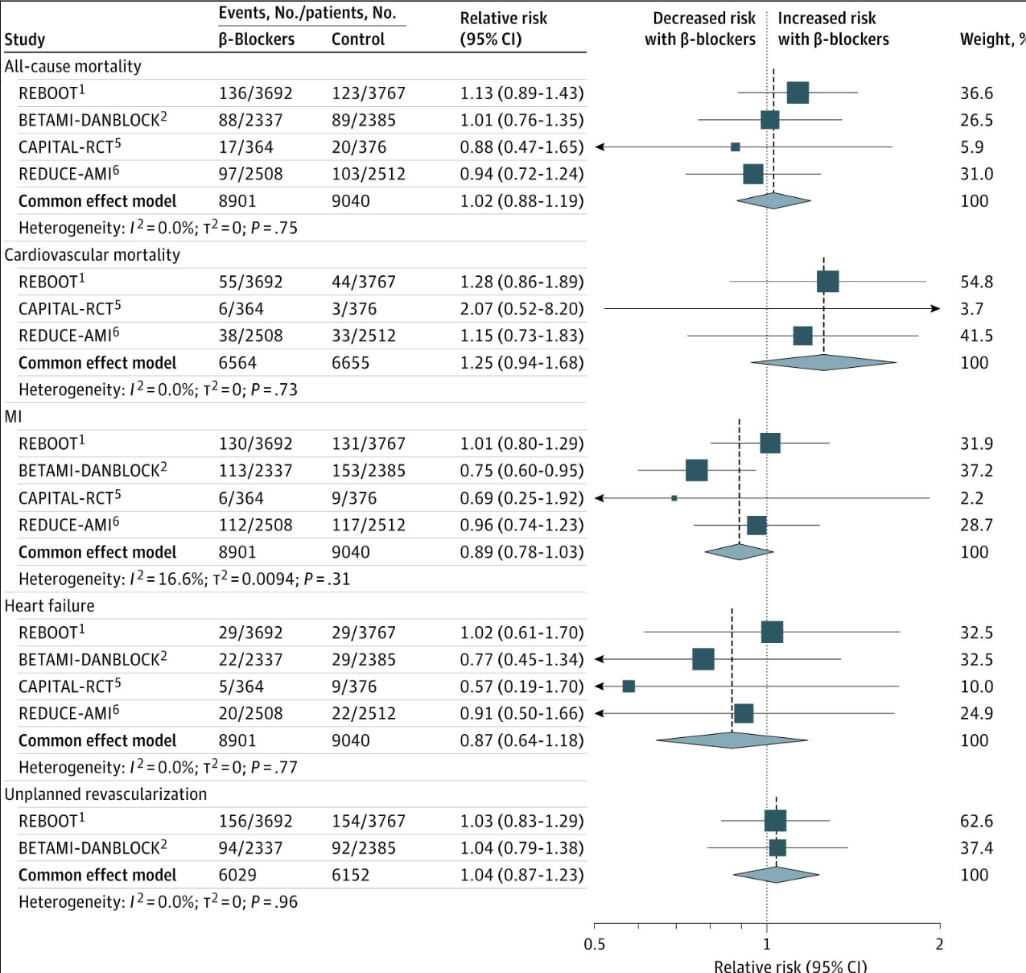
After ACS s/p reperfusion:
Pt's with this TTE finding do not benefit from long term Beta Blocker therapy.
LVEF > or = 50%. No difference in new HF, All cause death, recurrent MI
Uncertainty remains in optimum duration of BB
400
In Superfical Vein Thrombosis
Name at least 2 findings that would warrant anticoagulation
1. Thrombus > or = 5 cm in length
2. Persistent or worsening symptoms despite conservative therapy
3. Clot within 3cm of Deep Vein
4. Involvement of Greater Saphenous
5. Other ongoing risk factors for clotting
**Differences between PPX and Tx AC**
400
Jarisch-Herxheimer Reaction is classically associated with treatment of these types of organisms
Jarisch-Herxheimer: acute, self-limited febrile reaction, usually within 24 hours after starting therapy for a spirochetal infection.
T. pallidum, Borrelia spp, Leptospira
400
_______ is associated with hepatic cysts and intracranial Berry aneurysms and has BP Goal of _______.
Autosomal Dominant Polycystic Kidney Disease
BP Goal < 110/75 for ages <50
If 50 or >, or CKD3 or worse, SBP goal 120 or less
400
This antibody is associated with Immune Mediated Necrotizing Myopathy

500
Name at least 3 EKG Features of Ventricular Arrythmia
1. NW Axis (-90 to +180)
2. AV dissociation
3. Wide QRS (> 140)
4. Fusion or Capture Beats
5. Loss of RS morphology in precordials
6. RS duration > 100ms (2.5 small boxes)
7. Various QRS Morphology criteria
500
In Anti-Phospholipid Syndrome
1. Describe the Clinical Criteria
2. aPL labs and Timing
2023 ACR/EULAR Classification Criteria
1. Thrombosis or Pregnancy Morbidity
- Clot in Artery or Vein, 3 abortions before 10w or 1 after 10w, or premature birth due to pre-E/E or placental insufficiency
1. LA, aCL, anti-B2GPI
- > 99th percentile
2. Labs at least 12 weeks apart
500
What Klebseilla spp produces AMP-C resistance, and name 2 ABX that can be used to treat it
1. K. aerogenes, formerly known as Enterobacter aerogenes
2. AMP-C organisms can be treated by Cefepime, Avycaz, or carbapenems
500
How does this condition present and what is/are the acute treatment(s)??
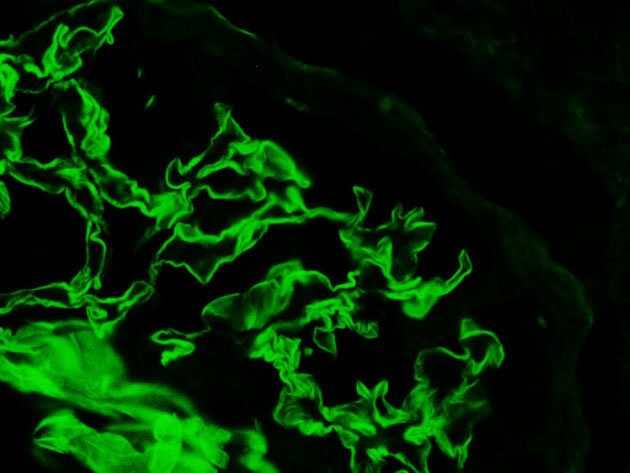
Linear Immunoflouresence of anti-GBM disease
Presentation: Most commonly with RPGN (macrohematuria, proteinuria, RBC casts etc).
Pulm-Renal: Small % with have capilaritis with hemoptysis
Immediate Tx is PLEX within 24H plus immunosuppression with steroids and cyclophosphomide
500
22 yo M with palpitations, EKG, and FH of SCD
What "sign" is present and what "syndrome" does he have?
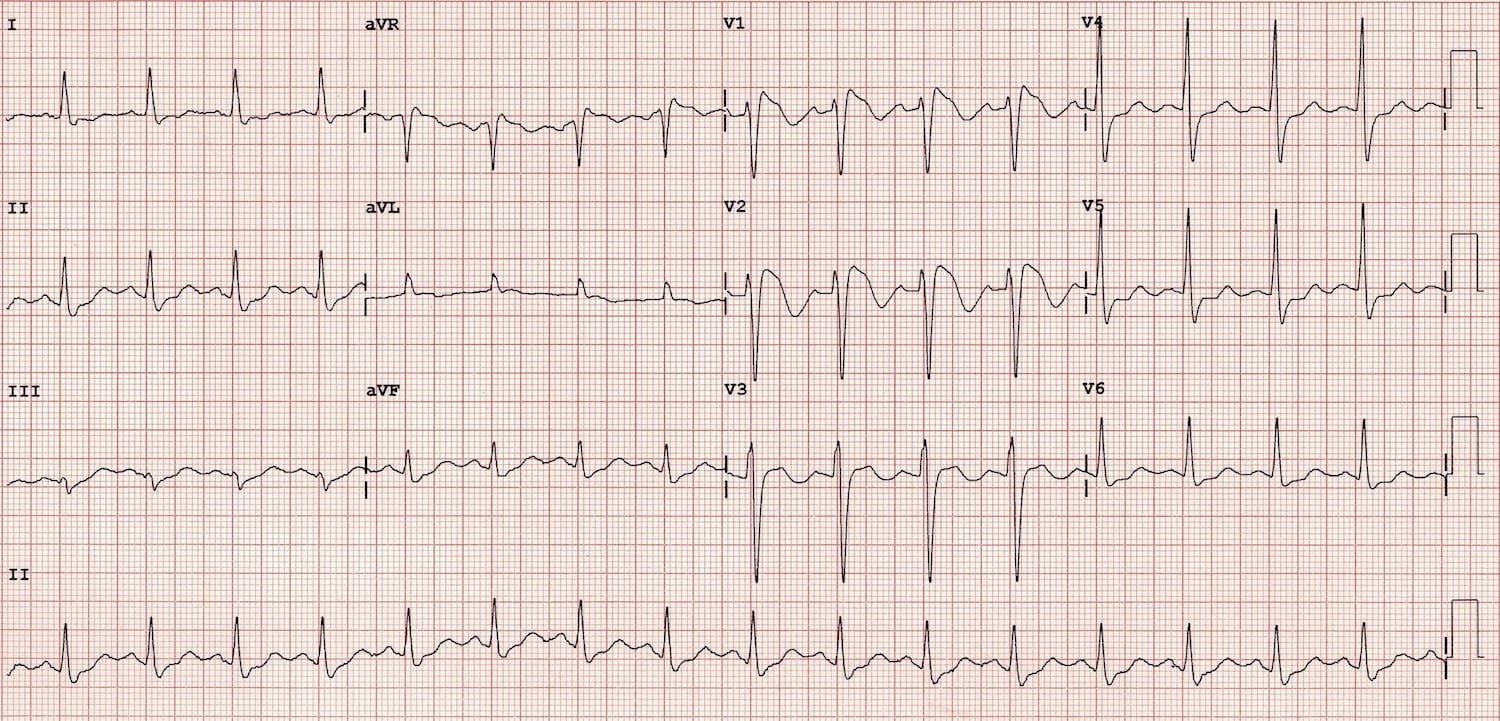
Brugada Syndrome = EKG + Symptoms
Brugada Sign = EKG only
