Pathology
Clinical
Pharmacology
Anatomy
100
What type of epithelium normally lines the oesophagus?
How does the epithelium change in GORD? Outline the stages and the end result if GORD is uncontrolled.
Non-keratinising stratified squamous epithelium (NKSSE)
Reflux of gastric acid into the lower oesophagus causes NKSSE to undergo metaplasia into columnar glandular epithelium ('intestinal metaplasia' rich in goblet cells)
--> dysplasia --> adenocarcinoma
100
What are the classic symptoms of GORD?
Reflux, waterbrash
Cough, belching
Bloating
Retrosternal burning pain radiating to the jaw
100
Where is the Chemoreceptor Trigger Zone and what is its function?
In medulla, outside BBB (can detect toxins/chemicals in blood and CSF).
Input from labyrinth (inner ear and vestibular system) and GIT.
Contains receptors - serotonin, dopamine, opioid...
100
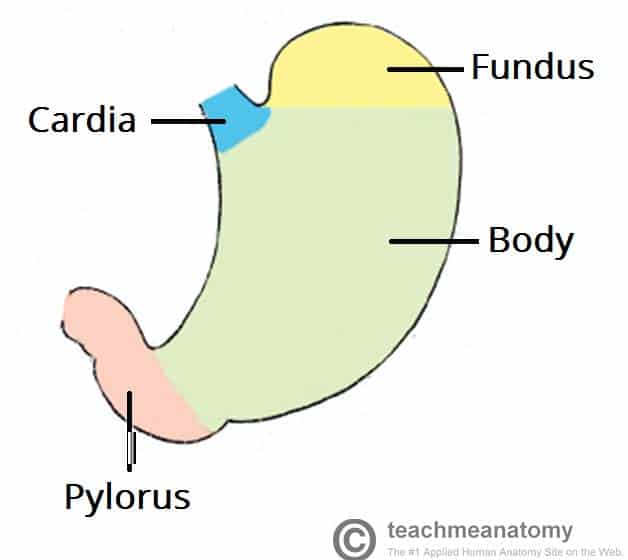
Draw a stomach and label the different parts.
200
What is achalasia?
Lack of coordinated muscle contractions
Impaired relaxation of the lower oesophagus
Retention of food bolus and impaired swallowing
Megaoesophagus complication
'Bird beak' sign
200
List 3 differentials for upper GI bleed
Oesophageal varices
Peptic ulcer
Oesophageal tear (Mallory-Weiss)
Gastric cancer, polyp
200
List the dopamine receptor antagonists used in nausea/vomiting. Which one/s cross the BBB and why is this significant?
Domperidone
Cross BBB - Prochlorperazine, Metoclopramide (can bind to basal ganglia and substantia nigra causing Parkinsonism)
200
Outline gastric acid secretion (the cell types involved).
Parietal cells are stimulated by G cells (gastrin) and ECL cells (histamine) to secrete HCl
300
What are the 2 types of oesophageal cancer? Compare their location & risk factors.
Squamous cell carcinoma - middle/lower oesophagus (heavy alcohol and smoking)
Adenocarcinoma - lower oesophagus, metaplasia (Barrett's oesophagus, GORD)
300
Draw an abdomen with 4 quadrants, and list 2-3 differential diagnoses for abdominal pain in each quadrant.
RUQ - cholecystitis, biliary colic, hepatitis
RUQ/LUQ - pancreatitis, gastritis, GORD, MI, lower lobe pneumonia
LUQ - splenic infarction/rupture, renal colic
LIF - diverticulitis, renal colic, torsion (ovarian/testicular)
RIF - appendicitis, Crohn's, renal colic, torsion (ovarian/testicular)
300
What system is involved in motion sickness?
What receptors are involved and what medications can be used to combat motion sickness?
Labyrinth/vestibular system (inner ear) with acetylcholine and histamine receptors.
Acetylcholine M1 receptor blockers - hyoscine (scopalamine)
Histamine H1 receptor blockers - dimenhydrinate, pheniramine, promethazine
300
There are 3 zones of constriction in the oesophagus - can you name them?
Cervical (cricopharyngeal sphincter)
Thoracic (aortic arch, primary bronchus)
Diaphragm (hiatus)
400
Define 'hiatus hernia' and explain the different types.
Upper part of stomach moves through the diaphragm/oesophageal hiatus into the thorax
Sliding - stomach herniates through the hiatus, impaired lower oesophageal sphincter
Paraoesophageal/rolling - stomach protrudes ALONGSIDE the oesophagus, lower oesophageal sphincter is intact thus there is rarely reflux
400
Thinking about the 4 ways to block a tube, what are some differential diagnoses for dysphagia?
Luminal - foreign bodies
Wall - neoplasm (oesophageal adenocarcinoma), stricture
Extrinsic - mediastinal tumours/mass, thyroid/goitre
Function - achalasia, motor neuron disease
400
What is the MoA of Ondasetron? Explain why it may be useful in surgery and chemotherapy-related nausea.
5HT3 (serotonin) receptor antagonist
Surgery/chemo can cause GIT ECL cells to release 5HT which then binds to 5HT3 receptors in GIT --> impulses sent to CTZ
Ondansetron blocks 5HT3 receptors in both GIT and CTZ
400
Outline the venous drainage of the foregut, midgut, hindgut
Foregut --> portal vein --> IVC
Midgut --> superior mesenteric vein --> portal vein --> IVC
Hindgut --> inferior mesenteric vein --> splenic --> portal --> IVC
500
What are the major causes of chronic gastritis? Briefly explain the pathophysiology
Helicobacter pylori - bacteria colonises the epithelium, causes damage and inflammation, usually antrum location, ulceration
Autoimmune (pernicious anaemia) - antibodies to parietal cells or IF, impaired secretion of HCl and impaired absorption of B12 with megaloblastic anaemia
Reactive - alcohol, toxins directly damage mucous layer
500
What symptoms might someone with a peptic ulcer complain of?
What investigations would you order?
Reflux, retrosternal chest pain/epigastric pain, haematemesis, malena
Burning may increase with food (gastric) or empty stomach (duodenum)
H. pylori urease breath testGastroscopy
500
List 4 types of laxatives based on their MoA and give an example of each.
Stool softeners (allow water to enter stool) e.g. Docusate
Bulk-forming (trap water and increase bulk) e.g. Psyllium husk, bran
Osmotic (draw water in via osmotic pressure) e.g. Macrogol, Lactulose, Mg
Stimulants (increase peristalsis) e.g. Bisacodyl, Senna
500
What is the major arterial supply to the stomach? What branches help to perfuse the stomach?
Coeliac trunk - L gastric, common hepatic, splenic
Splenic - L gastro-omental, short gastric
Common hepatic - R gastric, gastroduodenal, hepatic artery proper
