Ant Seg
Post Seg
Perimetry
Review
Fun Stuff
100
What is the critical angle at the tear-air interface that causes total internal reflection, making it impossible to visualize the angle without a gonioscopy lens?
BONUS (+200 pts): Sampaolesi's line is a pigmented line seen on gonioscopy. Where exactly is it located, and in which two conditions is it classically seen?
46°
BONUS: +200 Sampaolesi's line is a line of pigment deposited anterior to (above) Schwalbe's line. It is seen in pseudoexfoliation syndrome and pigment dispersion syndrome.
100
For the normal neuroretinal rim, state the order of thickness from thickest to thinnest.
Inferior > Superior > Nasal > Temporal. Violation of this rule (particularly inferior or superior notching) suggests glaucoba
100
Define Mean Deviation (MD) and Pattern Standard Deviation (PSD) on the HVF, and explain which is more affected by media opacity such as cataract.
MD measures the average age-matched sensitivity loss across the entire field (more negative = more loss). It IS altered by media/lens opacity since diffuse depression lowers MD globally.
PSD measures the index of localized (focal) VF loss and tries to account for media opacities by assessing non-uniform deviation patterns (it is less affected by diffuse depression from cataract.
100
What is the embryologic origin of the structure below labeled "A?"
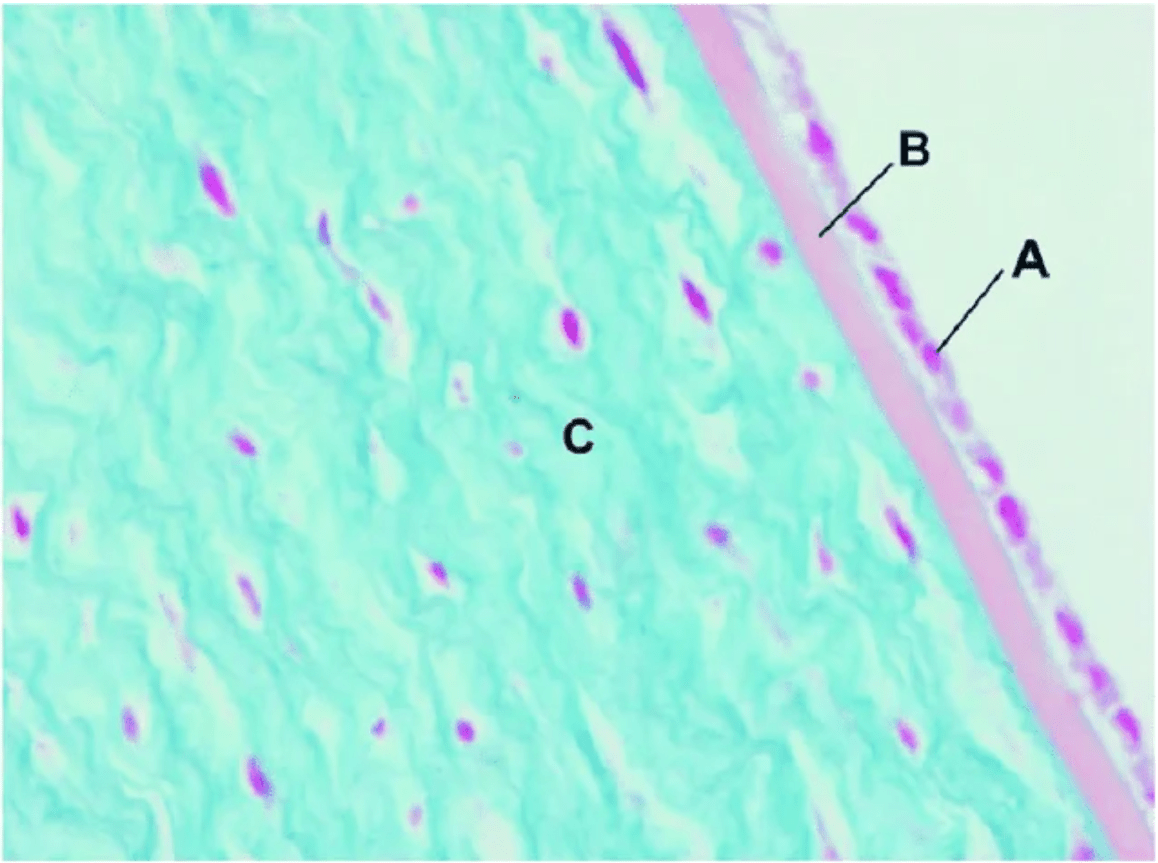
Corneal endothelium => neural crest
100
Interns only:
What is Dr. Recko's wife's name?
Meredith Recko!

200
On gonioscopy after blunt trauma, what are the three specific traumatic angle findings, and what is the structural tear that defines each one?
BONUS (+100 pts): What slit-lamp technique is used to identify Schwalbe's line on gonioscopy, and what does it rely on?
1. Angle recession = tear between the longitudinal and circular ciliary body muscles → abnormally wide ciliary body band. 2. Cyclodialysis = tear between the ciliary body and scleral spur → enlarged suprachoroidal space (appears more white). 3. Iridodialysis = tear between the iris and ciliary body.
Bonus: The parallelopiped (wedge) technique. The external and internal corneal light beams converge and meet precisely at Schwalbe's line, identifying it (even when pigmentation is absent).
200
What three layers make up the ganglion cell complex (GCC) on OCT?
Bonus +100: The BCSC notes that the macular RGC layer contains what proportion of all RGCs in the entire retina?
The GCC consists of: RNFL (retinal nerve fiber layer) + Ganglion Cell Layer (GCL) + Inner Plexiform Layer (IPL).
Bonus: More than 50% of all RGCs are located in the macula
200
The 24-2 and 30-2 HVF programs use a 6° grid. What does the '2' in '24-2' specifically mean about point placement?
The '2' means the test points are NOT located exactly on the horizontal or vertical midline. Instead, they are placed 3° above and 3° below the horizontal meridian
The grid straddles the horizontal and vertical meridians. Makes it easier to see whether defects respect the horizontal or vertical midline
200
Extraocular extension of malignant melanoma of the choroid occurs via emissaria that also transmit what other structure(s)?
Vortex veins via the middle emissaria
200
Interns only: Which one of your fellow residents has completed multiple triathlons and enjoyed the sunrise at the 19,341 foot summit of Mt. Kilimanjaro?

300
Your patient has angle closure and you are attempting to distinguish between appositional and synechial angle closure. Your clinic has all imaging modalities available including UBM, AS-OCT. Describe how you would distinguish these pathologies and the role these imaging modalities play.
Dynamic (indentation) gonioscopy must be used. Neither imaging modality can distinguish.
Dynamic applies gentle corneal pressure to force aqueous into the angle, attempting to open it. It distinguishes: (1) appositional closure (the angle opens with pressure) from (2) synechial closure (PAS) (the angle remains closed despite pressure).
300
The three types of retinal ganglion cell neurons are M cells, P cells, and K cells. Match each to its function: motion, color/detail, and blue-yellow response.
M cells (Magnocellular) = large dendritic field and axon diameter, fast conduction → Motion. P cells (Parvocellular) = small dendritic field and axon diameter, slow conduction → Color and Detail. K cells (Koniocellular/bistriate) → Blue-yellow response (short wavelengths).
300
Standard automated perimetry (SAP) is described as 'white-on-white.' What does this mean, and what algorithm does the Humphrey Field Analyzer use?
White-on-white = a white stimulus presented on a white background. The HVF uses SITA (Swedish Interactive Threshold Algorithm), which uses a database of normal patient responses to generate probability values for sensitivity at each location.
300
The 4 attachments to Whitnall's tubercle.
BONUS (+100): This tubercle is inferior to what suture?
Check ligament of lateral rectus, Lockwood ligament, lateral canthal tendon, lateral horn of Levator aponeurosis
BONUS: Frontozygomatic suture
300
Which of your fellow residents was awarded a big athletic scholarship in college and where did this person play?
Florida Southern College
400
In the Spaeth grading system, iris insertion is described by letters A through E. What does each letter represent?
Bonus 100: Iris configuration uses four letters. What does 'b' stand for, what does 'c' stand for, and what does 'p' stand for?
A = Anterior to TM (at Schwalbe's line); B = Behind Schwalbe's line; C = posterior to sCeral spur; D = Deep into ciliary body face; E = Extremely deep ciliary body.
Bonus: b = bowing anteriorly; c = concave, bowing posteriorly; p = plateau iris configuration. (Also: f = flat/regular.)
400
What is this?
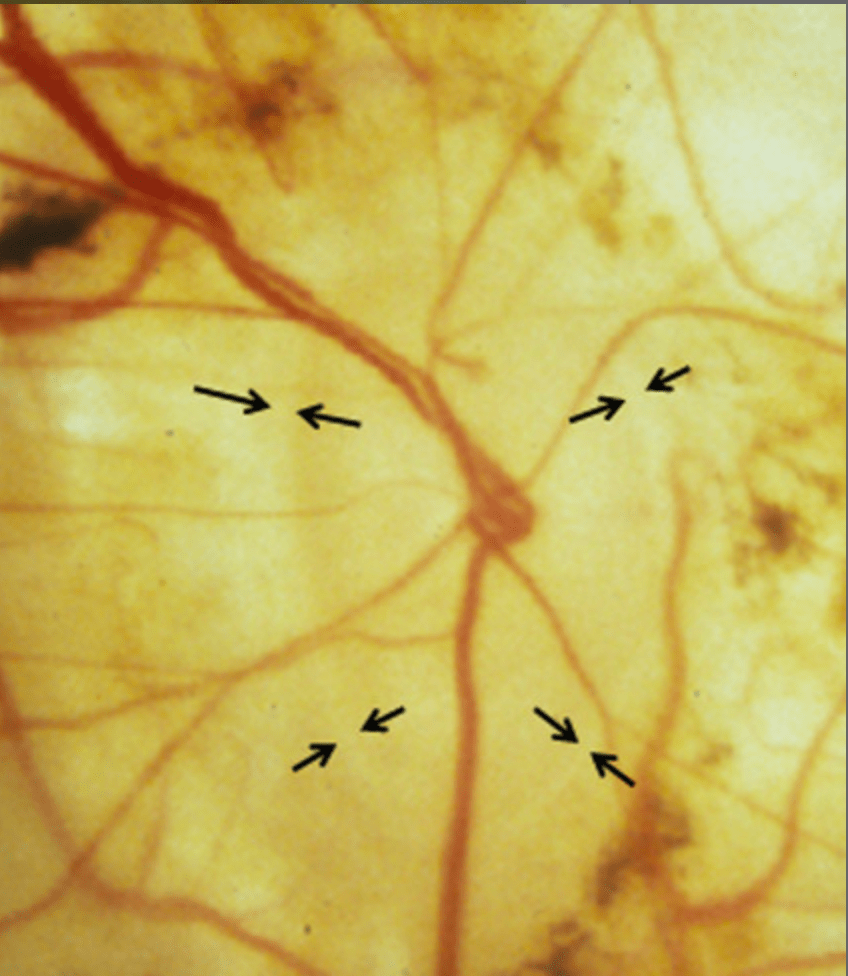
The peripapillary ring (PPR) or the Ring of Elschnig is a rim of connective tissue located between the optic nerve and the surrounding choroidal/scleral tissue. It forms the border between the neural tissue of the optic nerve head and the adjacent sclera/choroid.

400
For the reliability indices on HVF: what fixation loss percentage is considered unreliable, what false-positive rate is considered unreliable, and which is most detrimental?
Bonus 100: Why may a highly attentive patient have a high FN rate>
Fixation loss >25% = unreliable. False positives >15% = unreliable. High FP rate is most detrimental because a patient responding without any stimulus can make a damaged field appear artificially normal
Bonus: Increased variability of sensitivity in damaged areas
400
List the measurements for all of the following:
Foveola is located how far from the center of the ON?
Foveola diameter?
Fovea diameter?
Parafovea width?
Perifovea width?
Range for diameter of the FAZ? Must be within 100 for upper and lower limit of range
Foveola is located how far from the center of the ON? 4mm temporal and 0.8mm inferior
Foveola diameter? 0.35mm
Fovea diameter? 1.5mm
Parafovea width? 0.5mm
Perifovea width? 1.5mm
Diameter of the FAZ? 250-600 um
400
Which one of your fellow residents took up skeet shooting in high school and still plays casually?

500
A female patient presenting with monocular eye pain is noted to have a beaten bronze appearance of her corneal endothelium, a ratty appearing iris and significantly elevated IOP. Which of the following is true of this disease process?
a. Corneal endothelial cells become like epithelial cell, proliferating and migrating and ending on the Schwalbe line, resulting in high PAS
b. Despite, proliferation, endothelial cell count is generally not elevated
c. Specular microscopy reveals endothelial cells with a distinct hexagonal shape
d. Specular microscopy reveals endothelial cells without pleomorphism
a. Corneal endothelial cells proliferate and migrate, ending on the Schwalbe line, resulting in high PAS (extend all the way to the iris)
b. Despite, proliferation, endothelial cell count is generally not elevated (it's low!)
c. Specular microscopy reveals endothelial cells with a distinct hexagonal shape (they lose that shape)
d. Specular microscopy reveals endothelial cells without pleomorphism (significant pleomorphism)
500
What is the difference between alpha and beta zones of peripapillary atrophy (PPA), and which is more specifically associated with glaucoma?
Alpha zone = temporal crescent with hyper/hypopigmentation, seen with glaucoma/nonglaucomatous eyes/myopia. Beta zone = loss of choriocapillaris and RPE leaving a white area adjacent to the disc with increased visibility of the choroidal vessels (specifically associated with glaucoma)
500
Describe the Glaucoma Hemifield Test (GHT)
and
According to the OHTS trial, what defines an abnormal visual field?
Bonus 250: When should you preferentially look at MD vs PSD and what paradoxically happens in advanced glaucoma?
The GHT compares corresponding areas above and below the horizontal meridian.
A VF defect is defined as: PSD with p<5% OR the presence of a GHT result 'outside normal limits' present across 3 consecutive VFs
Bonus:
- In early glaucoma, look primarily at PSD (and the Pattern Deviation plot) because it highlights focal damage while MD may still be only mildly abnormal.
- In advanced glaucoma, MD becomes more useful for tracking further worsening, while PSD may paradoxically decrease as the whole field flattens out.
500
1) +250: The posterior pigmented epithelium of the iris is continuous with what structures in the ciliary body and retina?
2) +250: Describe the orientation of the pigmented and non-pigmented ciliary body epithelium and which maintains the blood aqueous barrier?
1) Non-pigmented epithelium of the ciliary body and neurosensory portion of the retina
2) Apex to apex with inner non-pigmented on the inside and pigmented on the outside. Non-pigmented tight junctions near the apical border (zonulae occludentes)
500
Which attending ran a window cleaning business?
Bonus +1000 What was the name of the business and where was it located?
Brent and Staci Rocke! Pinks in San Antonio
