DKA
Urethral Obstruction
Stat
Seizures
IMHA
100
What do we use to determine that a patient is in DKA and not just diabetic?
Elevated BG, Ketones in the serum or urine, Acidosis
100
Male cat presents screaming, vomiting and not eating. Patient is lateral when you get him. What is the first thing we should check?
If there is a large firm bladder.
100
You have a large breed deep chested dog. Presented for non-productive retching and prayer posture. What should you do?
Stabilize!, can palpate a ping in some from hard air in stomach. Other wise take a right lateral Radiograph to look.
100
Milo is a 2 year old golden that presented for having two seizures in the last two hours that lasted 3 minutes a piece. No previous health issues. What could be causing this?
Idiopathic ( more likely < 6 years of age)
Toxicity
Metabolic ( liver issues vs infection vs other)
Intracranial (brain tumor)
100
Patient comes in with white gums, bruising on the ventral abdomen and legs. Patient is a 7 year old miniature schnauzer that weighs 12 kg. PCV is 8 % what should we test next?
Saline agglutination
Lacuna
Blood smear
BW- T bili elevated
200
You have established on BW that patient is in DKA. Patient's PCV is 60% and they are tacky. Dehydration 8%. What should we do before starting the insulin CRI?
Rehydrate
200
You/VOD palpate and agree there is a large firm urinary bladder. What diagnostics are most important?
Radiographs- is there a stone (this will need surgery)
EPOC at minimum, full blood work recommended. Checking BUN/Creatinine/Phosphorus and POTASSIUM!!!
200
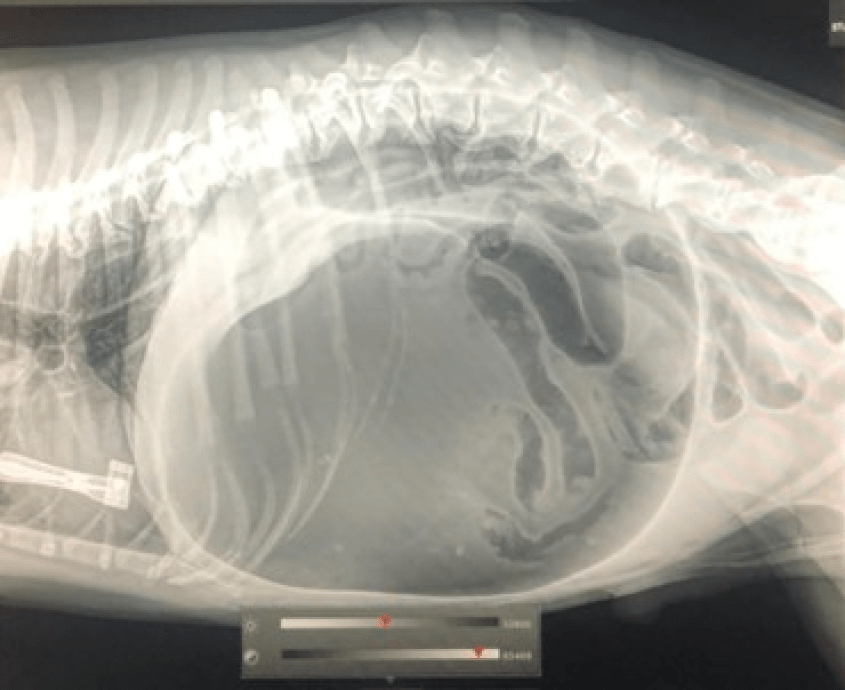
This is your radiograph what are we looking at? should you take the other two images?
Double bubble vs smurf hat.
NO!!!!!
200
What diagnostics should we consider? why?
BW full check for infection, organ function, hypoglycemia, vs other
Radiographs- metal toxicity neoplasia vs other
Perfect world MRI/CT to check brain
200
Blood smear shows what with the two arrows with tails... 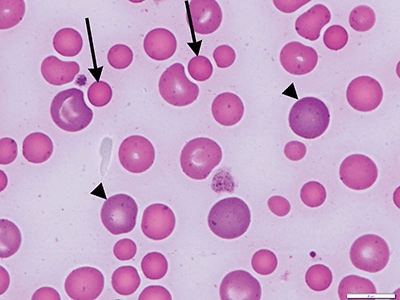
spherocytes
300
The doctor is ready to start Insulin CRI. The dog weighs 9 kgs. Explain to me what you putting in the bag for the CRI. BG is 400 mg/dl.
250 ml Bag 0.9% NaCl
Remove 10 ml from bag
Add 19.8 Units Novolin R
Flush 50 ml through line. Run at 10 ML/h
300
Patient is dull but won't allow us to place u-cath awake. Potassium is 9 and the VOD is worried. Why is this concerning?
Potassium can be cardiotoxic meaning when we sedate they could go into CPA
300
The VOD sees this and yells at you to start setting up!! what are you doing next?
Depending on people start with double FRONT LEG CATHETERS of the largest bore we have. bolus 1 Liter
Get things to Trochar pet
Obtain at minimum an EPOC if not whole blood work.
If enough people set up for surgery and stomach tube
300
Patient starts to seize during exam. What should we do?
Place IVC and give midazolam 0.5-1 mg/kg depending on doctor
300
We confirm IMHA. We are concerned there are low platelets also. What is the syndrome called when we have both ITP and IMHA?
Evans
400
Based on Recent EPOC the VOD wants to do KCL. Due to patients needs they elect to do KCL CRI. Remember the dog is 9 kg. VOD wants to run KCL at 0.2 mEq/kg/h. We want to run the CRI at 7 ml/h and in a 60 ml syringe. Set it up.
KCL Concentration= 2 mEq/L KCL
(0.2 mEq/kg/hr) x (9 kg)= 1.8 mEq/hr KCL
60 ml syringe/ 7 ml/h= 8.57 hours
(1.8 mEq/hr) x (8.57 hours)= 15.42 mEq
(15.42 mEq)/(2 mEq/ml)= 7.71 ml KCL
Mix 7.71 ml KCL + 52.29 ml Norm-R in syringe and run at 7 ml/h
400
VOD would like to do Calcium gluconate for this pet. What must we monitor while running? why? Does calcium gluconate lower the Potassium?
ECG they can get arrhythmias
No it does not lower it is just cardio protectant
400
EPOC comes back and the VOD faints. What did she see that was so concerning? Why?
Lactate over 6
Anything over 6 is concerned for GI necrosis.
400
Patient came out of the seizure. Diagnostics are normal. Its either idiopathic vs intracranial as we did no MRI. Owners approved hospitalization. Patient has another seizure and VOD wants to start another medication. What should we start? Dose?
Keppra 30-60 mg/kg give slowly
400
Due to the low PCV we decide to start treatment and oxygen. We do a blood transfusion and place in oxygen. Why do we place in oxygen? what is the concern with the blood transfusion?
How long does a blood transfusion RBC last in the body if not destroyed?
We place in oxygen because deoxygenated blood is more likely to be destroyed. Trying to prevent destruction.
Blood transfusion can speed up destruction as it is foreign.
3 days
500
We notice that someone set the syringe pump of KCL up wrong. They did the right amount in the syringe but the rate was set to 17 ml/h. Calculate the kmax to determine if this is safe.
kMax ( mEq/hr)= (0.5 mEq/kg/h) x (body weight kg)
KMAX= 0.5 x 9=4.5 mEq/h maximum
apply to our CRI
concentration 15.42 mEq / 60 ml = 0.257 mEq/ml
17 ml/h x 0.257 mEq/ml = 4.369 mEq/h
Which is less then our kmax and safe thankfully.
500
VOD asks you to do the calcium gluconate. The cat is 4.67 kg. VOD wants to do 0.5 ml/kg of 10% calcium gluconate IV slowly over 15 minutes. Then go straight into unblocking. Our calcium gluconate is 23%. This needs to be diluted to 10% solution to give.
0.5 ml/kg x 4.67 kg= 2.33 ml of 10 % solution.
C1V1= C2V2
2.33 ml x 100 mg/ml = C2 x 230 mg/ml
233 mg = C2 x 230 mg/ml
C2= 1.01 ml ( C2 is ml of 23%)
Then to dilute it you need a total of 2.33 ml. 1.01 ml of 23% ( gives you your 233 mg) then dilute with norm-r with 1.32 ml to reach your 2.33 ml total from beginning.
500
Patient is trochared and taken into surgery. Everything went well and thankfully no necrosis. However the spleen was torn and a splenectomy performed. What should we monitor for after surgery?
ECG for VPCS
500
Patient seized through the keppra at the high end. Did phenobarbital and still no response. VOD discussed with owners doing a propofol CRI. owners approved. They ask you to set it up. Patient weighs 32 kg
We want a 5 mg/kg IV bolus follow by 0.2 mg/kg/minute CRI. Make this for 8 hours. How many bottles will we use? ( 50 ml bottle) as we charge by the bottle for this CRI
Bolus- 16 ml bolus ( 32 kg x 5 mg/kg= 160 mg / 10 mg/ml)
0.2 mg/kg/minute x 32 kg= 6.4 mg/minute / 10 mg/ml=0.64 ml/min x 60 min= 38.4 ml/h (also our CRI rate) x8 hours=307.2 ml total.
needs 6.14 bottles
500
We seem to be improving and on day 4 of hospitalization. We recheck a blood smear to assess. What are these cells?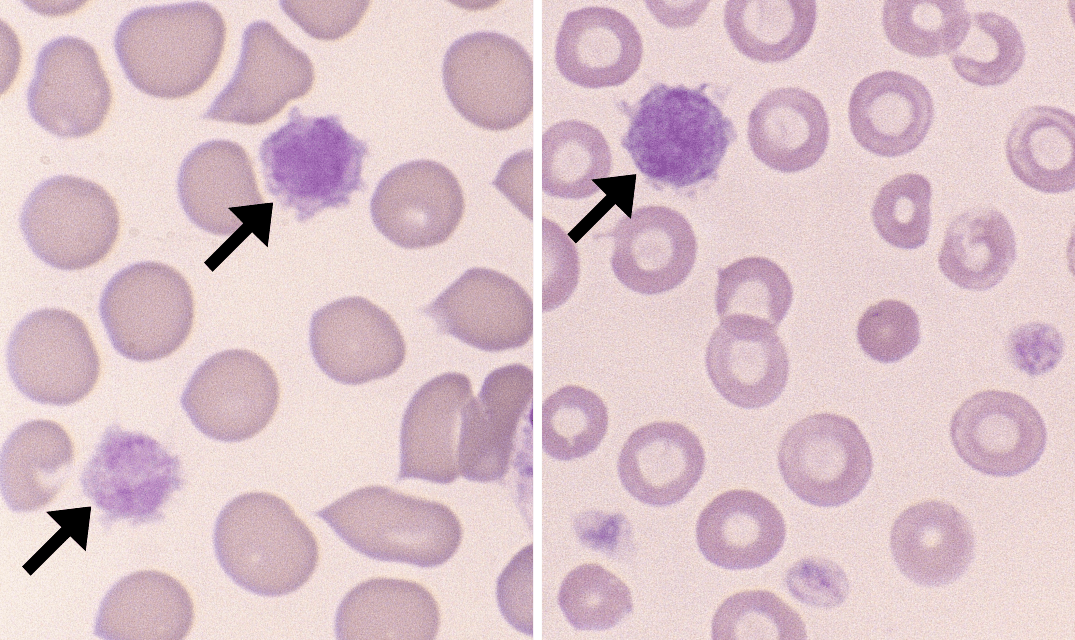
- Megathrombocytes: A direct term for large platelets.
or
- Giant Platelets: Another common term for these large blood cells.