Tendon Injuries
Hand Fractures
Hand Anatomy
Hand Infections
Lower Extremity
100
A 25M patient presents with a sharp laceration down to bone over the volar right middle finger proximal phalanx. He is unable to flex at the DIPJ or PIPJ. What is the zone of flexor tendon injury?
Zone 2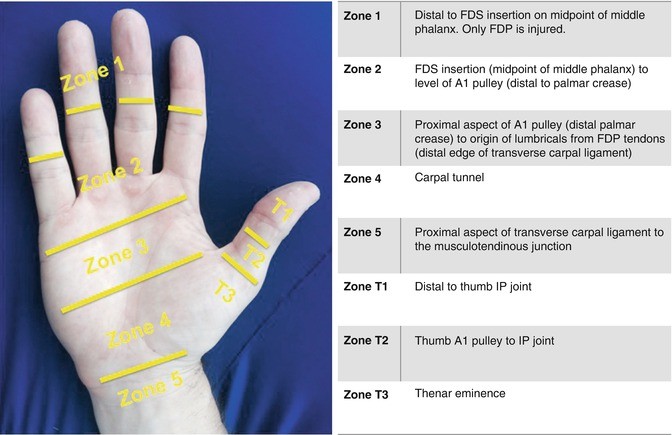
100
Most metacarpal fractures result in apex dorsal angulation. Which one of the following anatomic features is usually responsible?
A. The fracture pattern
B. The extensor tendons
C. The flexor tendons
D. The shape of the bone
E. The intrinsic muscles
E
Most metacarpal fractures display apex dorsal angulation because of the intrinsic muscles. For example, metacarpal neck fractures angulate apex dorsally because the intrinsic muscles lie volar to the axis of rotation of the MCP joint, maintaining flexion of the head. The mechanics of phalangeal fractures are more complex with basal fractures of the proximal phalanx tending to angulate apex volar due to the pull of the interossei, whereas middle phalanx fracture angulation depends on the position of the fracture relative to the flexor digitorum superficialis (FDS) insertion
100
Which one of the following is true regarding the anatomy of the flexor tendons?
A. The flexor digitorum superficialis (FDS) tendons insert into the distal phalanges.
B. The flexor digitorum profundus (FDP) tendons are attached to the lumbricals in the palm.
C. Camper’s chiasm lies at the level of the proximal interphalangeal (PIP) joint.
D. At the wrist, the index and little FDS tendons lie most superficial.
E. Flexor pollicis longus (FPL) originates from the lateral epicondyle of the humerus.
B. The flexor digitorum profundus (FDP) tendons are attached to the lumbricals in the palm.
The FDP originates from the proximal ulna and interosseous membrane and inserts into the distal phalanges to provide flexion at the distal interphalangeal (DIP) joints and contributes to proximal interphalangeal (PIP) joint flexion. It is also attached to the lumbricals in the palm, and this is important after flexor tendon division, as the proximal end of the FDP tendon will therefore not retract further proximal than the midpalm.
100
A 45-year-old builder presents with a hot, swollen, painful left middle finger 3 days after stabbing himself in the palm with a screwdriver. His middle finger is flexed and has a fusiform shape. He cannot tolerate passive digital extension or direct, gentle pressure over the volar aspect of the digit. A small bead of pus is expressed at the site of his original injury. Which one of the following is correct?
A. Kanavel’s cardinal signs of flexor sheath infection are all present.
B. This can be adequately managed with high-dose antibiotics and splinting.
C. This is likely to be polymicrobial and will require at least two antibiotic types.
D. There are no specific risk factors here for a poor outcome following flexor sheath infection.
E. Minimal access incisions alone should be adequate for surgical management.
A 
100
A 20-year-old man presents to the emergency department 6 hours after a bicycle accident with an open tibial fracture. The patient was traveling at 10 miles per hour at the time of the accident. The wound is 5 cm in length, and there is moderate contamination. The fracture is a mid-shaft tibial fracture with moderate comminution, with an associated closed fibula fracture. Which of the following Gustilo classifications is most appropriate for this injury?
A ) I
B ) II
C ) IIIA
D ) IIIB
E ) IIIC
The correct response is Option B.
200
A patient sustains an injury to the FPL tendon located over the thenar eminence. Within which zone of injury is this located?
Zone T3: Over thenar eminence
The thumb has five flexor zones, but these are different to the flexor zones for the other digits
200
You are referred a child with a phalangeal fracture passing through both the epiphysis and physis. According to the Salter-Harris classification system, what type of fracture does this represent?
This fracture represents a Salter-Harris type III injury.
The Salter-Harris classification applies to fractures that occur at the growth plate (physis) in developing limbs. The classification system is well known and is often tested in examination settings. The most common fracture pattern is a type II injury which involves the metaphysis and physis. These fractures can result in abnormal growth if the epiphyseal plates are permanently damaged ( Fig. 76.1 )
200
Which one of the following is correct regarding the intrinsic muscles of the hand?
A. There are eight interossei, all innervated by the ulnar nerve.
B. The sole function of the interossei is adduction and abduction of the digits.
C. The lumbricals originate from the flexor digitorum profundus (FDP) tendons and are all innervated by the ulnar nerve.
D. The lumbricals facilitate extension at the interphalangeal (IP) joints and are weak metacarpophalangeal (MCP) joint flexors.
E. The intrinsic muscles all share a similar bipennate structure.
D. The lumbricals facilitate extension at the interphalangeal (IP) joints and are weak metacarpophalangeal (MCP) joint flexors.
The intrinsic muscles of the hand include the lumbricals and interossei. There are seven interossei (four dorsal and three palmar), all of which are innervated by the ulnar nerve. Their main purpose is abduction (dorsal) and adduction (palmar) of the digits, but they also contribute to MCP flexion and interphalangeal (IP) joint extension. The lumbricals do originate from the FDP tendons and insert on the extensor hood but have dual innervation with the ulnar two receiving innervation from the ulnar nerve and the radial two receiving innervation from the median nerve. The palmar interossei are unipennate, while the dorsal interossei are bipennate.
200
A patient with a painful swollen fingertip is diagnosed with acute paronychia. Which one of the following is true?
A. This is a common infection originating in the pulp space.
B. Incision and drainage is the first-line treatment.
C. Management always requires removal of the nail plate.
D. Eponychial marsupialization is often required.
E. Staphylococcus aureus is the most likely pathogen.
E
Paronychia is an infection of the soft tissues surrounding the nail and can be acute or chronic. Acute paronychia is generally caused by a bacterial infection with Staphylococcus aureus and is associated with nail biting and minor trauma. First-line treatment is oral antibiotics, hand baths, and rest/elevation of the affected digit. In cases unresponsive to conservative management, it is necessary to drain the abscess and/or remove the nail plate. Chronic infections are more likely to be fungal and may require marsupialization or nail ablation in cases resistant to medical management. Pulp space infections are called felons. They can coexist with paronychia but are different entities. They are treated with incision and drainage plus antibiotics.
200
A 36-year-old man is evaluated for coverage of a 4 × 3-cm middle-third lower extremity soft-tissue defect with an exposed fracture of the mid tibia. Reconstruction with a proximally based medial hemisoleus muscle flap is planned. Which of the following arteries provides the major contribution to the blood supply
of this flap?
A ) Anterior tibial
B ) Dorsalis pedis
C ) Medial sural
D ) Peroneal
E ) Posterior tibial
The correct response is Option E. The soleus muscle is a bipennate muscle that is located in the superficial posterior compartment of the lower extremity, deep to the gastrocnemius muscle. The soleus muscle has a medial head that originates from the posterior aspect of the tibia and a lateral head that originates from the posterior surface of the fibula. The soleus functions in plantar flexion of the foot in conjunction with the gastrocnemius as they unite to form the Achilles tendon. Branches from the popliteal artery contribute to the blood supply of the proximal soleus muscle. The soleus muscle flap is a reliable local flap for coverage of moderate-sized soft tissue defects of the middle-third of the lower extremity. It is customarily elevated as a muscle-only flap and covered with a split-thickness skin graft. Branches from the posterior tibial artery contribute to the blood supply of the medial hemisoleus muscle flap, which is more reliable when based proximally.
300
18F sustains a 1-cm laceration over the radial aspect of the wrist. Clinical examination reveals no significant neurovascular or functional deficit, except she is unable to flex the little finger PIP joint independently. What is the next step in management?
A. Exploration under local anesthesia
B. Exploration under general anesthesia
C. Ultrasound investigation of the wrist
D. Clinical examination of the contralateral hand
E. Hand therapy referral
D. Clinical examination of the contralateral hand
The patient in this scenario is at risk of flexor carpi radialis and radial artery injury given the anatomic site involved, but clinically these structures do not appear to be injured. The chances of her sustaining an isolated FDS little finger injury are slim given the site of injury. It is far more likely that she has a congenital absence of the FDS; this occurs in approximately 20% of the population. It is important therefore to first assess the contralateral limb, since the condition may well be bilateral.
300
A 67-year-old woman underwent cast immobilization for treatment of a minimally displaced left distal radius fracture 5 weeks ago. Two weeks after cast removal, she is unable to extend her thumb. On examination, she is unable to perform retropulsion of the thumb with her palm placed flat on the examination table. Which of the following is the most appropriate next step in management?
A ) Electrodiagnostic studies
B ) Immobilization
C ) Primary tendon repair
D ) Tendon transfer
E ) X-ray study
The correct response is Option D. This patient is presenting with a rupture of the extensor pollicis longus (EPL) tendon, which occurs in as much as 5% of patients with mildly displaced distal radius fractures about 7 weeks after the initial injury. This is thought to be due to attritional rupture secondary to decreased vascularity. The treatment for this problem is a tendon transfer of the extensor indicis proprius to the EPL. Although some surgeons use a tendon graft, a primary repair is not feasible due to fraying of the EPL. Occupational therapy, immobilization, and further diagnostic studies (including electrodiagnostics and x-ray study) are not appropriate.
300
Which carpal bone is the least commonly fractured, as a result of the protection of the surrounding bony anatomy and strong carpal ligaments?
The trapezoid is the least commonly fractured carpal bone, as it is well protected by the surrounding osseous anatomy and the strong carpal ligaments surrounding tissues.
300
A diabetic patient presents with a rapidly progressing soft-tissue infection of the forearm. There is obvious crepitus within the soft tissues and overlying cellulitis with swelling. A diagnosis of gas gangrene is suspected. Which one of the following organisms is most likely to be involved?
A. Clostridium perfringens
B. S. aureus
C. Streptococcus spp.
D. Eikenella corrodens
E. Bacteroides fragilis
A. Clostridium perfringens
300
A 25-year-old man presents with a comminuted tibia plateau fracture sustained during a self-inflicted gunshot wound. During open reduction and internal fixation of the fracture, a 5-cm gap in the common peroneal nerve is noted. Tendon transfer, nerve repair with grafting, and nerve transfer are planned. Which of the following fascicular nerve transfers is most likely to aid in ankle dorsiflexion?
A ) Flexor digitorum longus to soleus
B ) Flexor digitorum longus to tibialis posterior
C ) Flexor hallucis longus to tibialis anterior
D ) Peroneal longus to extensor digitorum longus
E ) Soleus to extensor digitorum brevis
The correct response is Option C.
400
A 20-year-old rugby player is seen 1 day after sustaining a closed injury while grabbing the shirt of an opponent during a game. He is unable to flex the distal interphalangeal (DIP) joint of his right ring finger but is able to flex the PIP joint. A radiograph confirms the presence of a bony fragment at the level of the PIP joint. Which one of the following best describes this injury?
A. Leddy type I
B. Leddy type II
C. Leddy type III
D. Leddy type IV
E. Leddy type V
B. Leddy type II

400
Which one of the following carpal bones may be fractured during a wrist hyperextension injury through the “anvil mechanism.”
A. Triquetrum
B. Hamate
C. Trapezium
D. Capitate
E. Lunate
D capitate
The capitate is at risk of transverse body fracture during forced hyperextension when it is forced against the distal radius through the anvil mechanism ( Fig. 73.1 ). This can result in 180-degree rotation of the proximal fragment which cannot heal without formal reduction and stabilization. Patients remain at risk of avascular necrosis of the proximal fragment. 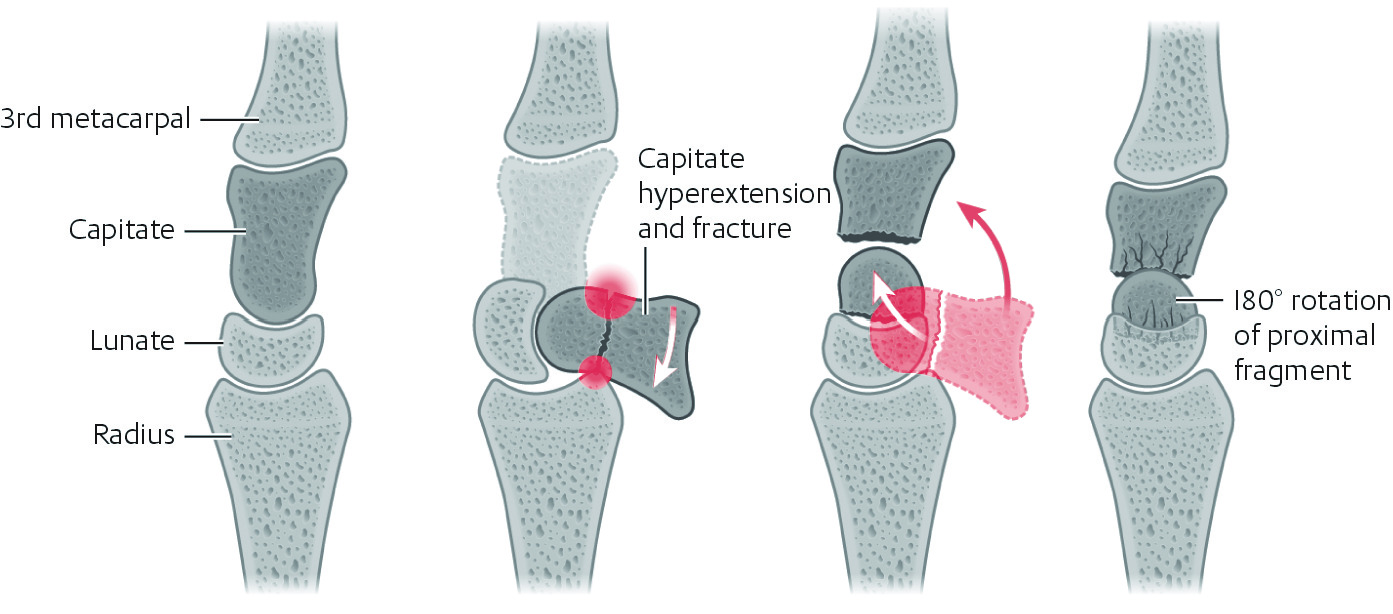
400
A 56-year-old woman presents for examination after undergoing completion
amputation through the distal interphalangeal joint of the right middle finger 6
months ago. When she makes a composite fist, the middle finger paradoxically
extends at the proximal interphalangeal joint. Which of the following anatomical
structures is most likely responsible for this finding?
A ) Central slip
B ) Flexor digitorum profundus
C ) Flexor digitorum superficialis
D ) Lumbrical
E ) Triangular ligament
The correct response is Option D. The finding described is called the lumbrical plus deformity, which is paradoxical extension of the interphalangeal (IP) joint or joints with active flexion of the digits. The lumbrical muscle originates from the flexor digitorum profundus (FDP) tendon and acts through the lateral bands to extend the IP joints and flex the metacarpophalangeal (MCP) joints. When the proximal end of the FDP tendon retracts, the lumbrical muscle retracts with it, resulting in increased force of MP flexion and IP extension on the affected finger. Since the FDP has a common muscle belly, when a composite fist is made, the unaffected fingers flex and the injured finger extends. In this patient, the injured finger does not flex because the FDP is no longer attached following amputation through the distal IP joint.
400
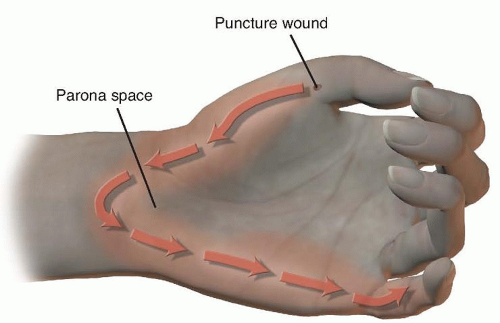
A 59-year-old man with type 2 diabetes mellitus comes to the office because he has had swelling, pain, and decreased function of the right small finger after he injured it slightly 2 weeks ago. The patient reports similar symptoms of the right thumb, although it sustained no inciting injury. Examination of both digits shows signs and symptoms of pyogenic flexor tenosynovitis. In addition to washing out the respective tendon sheaths, exploration of which of the following additional sites is necessary?
A) First web space
B) Flexor carpi radialis tendon sheath
C) Hypothenar compartment
D) Ring finger flexor tendon sheath
E) Space of Parona
The correct response is Option E.
Infectious flexor tenosynovitis can spread from the tendon sheath of the fifth digit to the flexor tendon sheath of the thumb by way of the space of Parona: the potential space in the volar wrist, deep to the flexor tendons but superficial to the pronator quadratus muscle. In this area, the proximal extent of the tendon sheaths of both the small finger and the thumb are in close proximity. This has been termed the “horseshoe abscess” of the upper extremity.

400
A 26-year-old man presents with silicone rods in the flexor tendon sheaths of
middle and ring fingers. Medical history includes saw injury resulting in flexor
tendon debridement. Second stage flexor tendon reconstruction using an
expendable donor tendon graft from the lower leg is planned. Which of the following
is the most appropriate description of the location for this tendon at the ankle?
A ) Anterior to the lateral malleolus
B ) Anterior to the medial malleolus
C ) In the anterior compartment
D ) In the lateral compartment
E ) Lateral to the Achilles tendon
F ) Medial to the Achilles tendon
The correct response is Option F. The most appropriate description of the location of the tendon at the ankle is medial to the Achilles tendon. The plantaris tendon can present an expendable donor tendon from the lower leg for tendon grafting. The plantaris is a small, thin rudimentary muscle with a long tendon. It acts in plantar flexion at the ankle and flexion at the knee, and harvesting does not leave any donor site deficits.
500
What is the most frequently ruptured flexor tendon after primary repair?
FPL
The most commonly re-ruptured flexor tendon is the FPL, but ring and little finger FDP tendons also have high rates of re-rupture. The overall rate of re-rupture after primary flexor tendon repair is around 5% and 10% for FPL. Volar plates placed distal to the watershed line can impinge on the FPL tendon. Higher power than other flexor tendons
500
A 25-year-old man presents to the office because of pain and swelling at the base of his dominant right thumb 3 days after a fall from his bicycle. X-ray study shows a Bennett fracture. The patient is scheduled for surgery. In addition to longitudinal traction and volarly directed pressure applied to the dorsal radial metacarpal base, which of the following best describes the appropriate reduction maneuver for this injury?
A ) Abduction and pronation of the thumb
B ) Abduction and supination of the thumb
C ) Adduction and flexion of the thumb
D ) Adduction and pronation of the thumb
E ) Adduction and supination of the thumb
A
Bennett fracture is an intra-articular fracture-dislocation of the carpometacarpal joint of the thumb that occurs following an axially loading force through a partially flexed metacarpal. A variable-sized volar ulnar fragment of the metacarpal base articular surface remains in position by attachment of the anterior oblique ligament to the trapezium. The larger fragment consisting of the remaining metacarpal base subluxates proximally, radially, and dorsally due to deforming forces from the abductor pollicis longus and the thumb extensors. Deforming forces from the adductor pollicis also cause metacarpal adduction and supination. To counteract the deforming forces of this unstable fracture-dislocation, reduction is attempted by applying axial traction to the extended thumb, palmar abduction, and pronation, while exerting pressure over the metacarpal base in preparation for insertion of Kirschner wires. 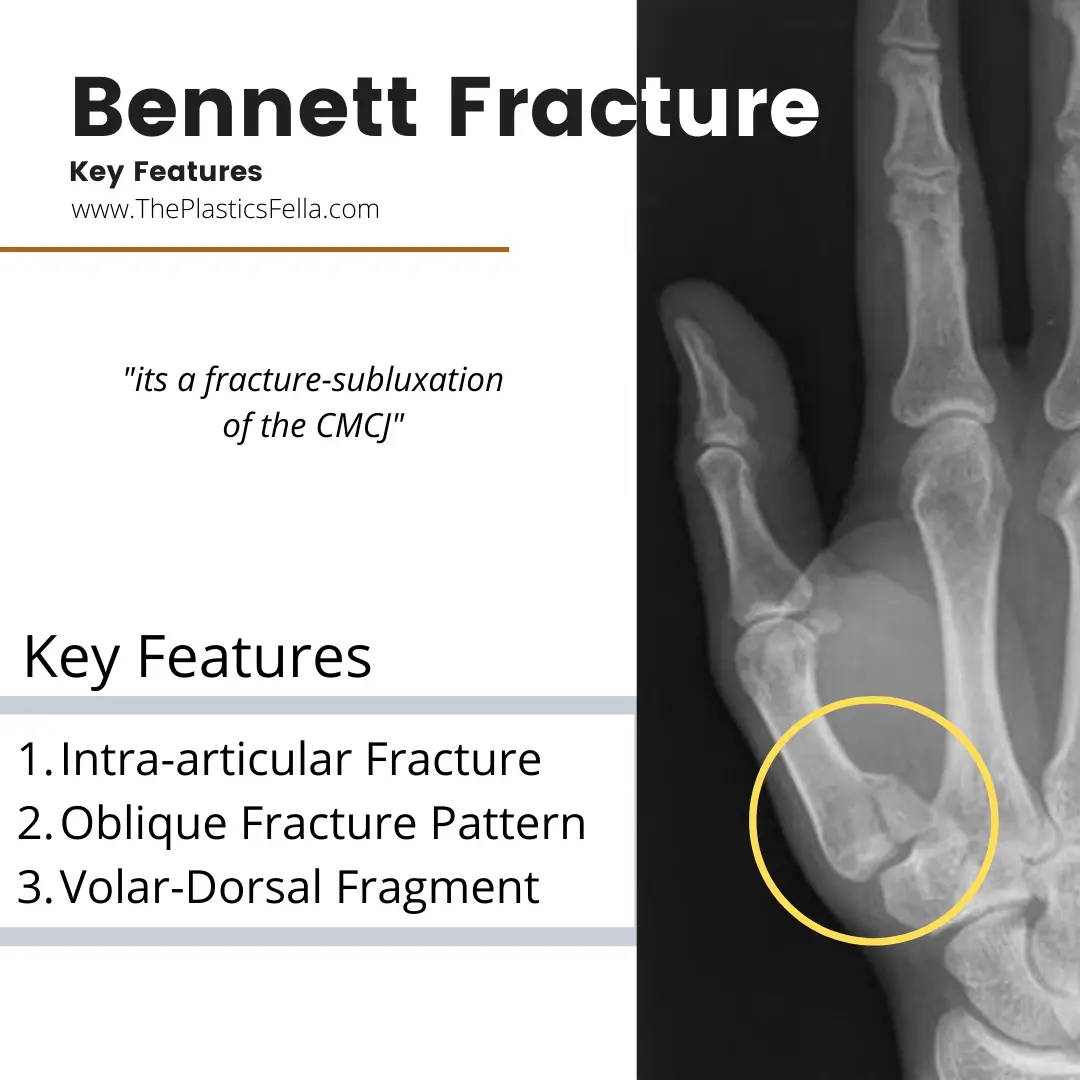
500
Which of the following is the most important ligament to prevent radial subluxation of the first metacarpal at the carpometacarpal joint?
A ) Anterior oblique
B ) Dorsal central
C ) Posterior cruciate
D ) Transverse metacarpal
E ) Ulnar collateral
The correct response is Option A. 
This patient presents with severe osteoarthritis of the carpometacarpal (CMC) joint of the thumb. The thumb metacarpal is in adduction, and the proximal phalanx is in hyperextension. The complex range of motion of the thumb basal joint is achieved through stability from 16 ligaments. Of the choices given, only the anterior oblique ligament is in the thumb at the basal joint. It has been found to be the most important preventative measure against radial subluxation in cases of CMC arthritis in biomechanical studies. It originates on the volar tubercle of the trapezium and inserts on the thumb metacarpal volarly. In cases of severe thumb CMC arthritis, the progressive ligamentous incompetence of the anterior oblique ligament and dorsal radial ligament allow the thumb metacarpal to migrate dorsally and proximally. The dorsal radial ligament is also important for basal joint stabilization, while the other ligaments of the thumb basal joint are not as important.
500
A patient inadvertently injects an oil-based material into a digit while using a high-pressure tool. Which one of the following is correct?
A. The dominant thumb is the most likely digit to be affected.B. Urgent debridement and decompression is required.C. Water-based solvents cause similar levels of tissue damage.D. The risk of subsequent need for amputation is low.E. Soft-tissue damage can be predicted by the size of the entry wound.
High-pressure injection injuries are a surgical emergency and can cause significant tissue damage through a small entry wound. Material is inadvertently injected into the digit at high pressure (often as high as 7000 psi). The most commonly involved digit is the nondominant index finger as the offending tool tends to be held in the dominant hand with the nondominant hand supporting the target object. These injuries need urgent surgical management with wound extension, irrigation, and tissue debridement. Both oil-based and water-based solvents can cause significant damage, but oil-based injuries tend to be worse and generate greater irritation of the soft tissues. Risk of amputation is high (up to 50%) after an oil-based, high-pressure injury such as paint injection. The entry wound does not provide much information with regard to the zone of tissue damage, so it is easy to underestimate its severity. Debridement often fails to remove all traces of injection material satisfactorily. If the fingertip is the entry point, material can frequently be identified in the forearm where it has been forced under pressure along the tendon sheath. This is in addition to the pressure insult to the soft tissues surrounding the entry point, for example, the fat of the pulp may be completely nonviable due to both barotrauma and foreign material contamination.
500
A 34-year-old woman presents with a 1-year history of progressive ankle and dorsal foot pain and paresthesias in the first dorsal web space. Electrodiagnostic study is significant for changes in the extensor digitorum brevis muscle. Which of the following nerves is the most likely source of this patient's symptoms?
A ) Deep peroneal
B ) Saphenous
C ) Superficial peroneal
D ) Sural
E ) Tibial
 The correct response is Option A. Anterior tarsal tunnel syndrome, also known as deep peroneal nerve (DPN) entrapment, is the result of compression of the DPN at the superior border of the inferior extensor retinaculum at the ankle joint and beneath the extensor hallucis longus tendon. Entrapment can occur as a result of wearing tight-fitting shoes or boots. It is important to rule out exertional anterior compartment syndrome or common peroneal nerve entrapment as the cause of symptoms. The nerve can also experience traction injury caused by chronic ankle instability due to ankle sprains.
The correct response is Option A. Anterior tarsal tunnel syndrome, also known as deep peroneal nerve (DPN) entrapment, is the result of compression of the DPN at the superior border of the inferior extensor retinaculum at the ankle joint and beneath the extensor hallucis longus tendon. Entrapment can occur as a result of wearing tight-fitting shoes or boots. It is important to rule out exertional anterior compartment syndrome or common peroneal nerve entrapment as the cause of symptoms. The nerve can also experience traction injury caused by chronic ankle instability due to ankle sprains.