Dr. Craig's picks
Dr. Intaphan's picks
Drs. Moscatello's/Browder's picks
Drs. Matthews'/ Bodle's picks
100
A 68-year-old man with a history of myocardial infarction and congestive heart failure is comfortable at rest. However, when walking to his car, he develops dyspnea, fatigue, and sometimes palpitations. He must rest for several minutes before these symptoms resolve. Which of the following is his New York Heart Association classification?
A. Class I
B. Class II
C. Class III
D. Class IV
E. Class V
The answer is C. The New York Heart Association (NYHA) classification is a tool to define criteria that describe the functional ability and clinical manifestations of patients in heart failure. It is also used in patients with pulmonary hypertension. These criteria have been shown to have prognostic value with worsening survival as class increases. They are also useful to clinicians when reading studies to understand the entry and exclu- sion criteria of large clinical trials. Class I is used for patients with no limiting symptoms, class II is for patients with slight or mild limitation, class III implies no symptoms at rest but dyspnea or angina or palpitations with little exertion and patients are moderately limited, and class IV is severely limited so that even minimal activity causes symptoms. There is no NYHA Class V. Treatment guidelines also frequently base recommendations on these clinical stages. This patient has symptoms with mild exertion but is comfortable at rest; therefore he is NYHA class III.
100
A 56-year-old woman is admitted to the intensive care unit (ICU) with a thunderclap headache and a rupture of an aneurysm of the anterior cerebral artery. She is treated with endovascular coiling. On admission to the ICU, she was originally intubated and sedated. Over the course of 4 days, she is extubated but continues to demonstrate right hemiparesis and aphasia. Seven days after her presentation, she abruptly declines with alert mental status
and marked worsening of her hemiparesis. A head CT is performed urgently and does not show any progression of bleeding or widening of the ventricles. She has been on nimodipine 60 mg every 4 hours since presentation. What is the most likely diagnosis for her worsened condition?
A. Cerebral edema
B. Hydrocephalus
C. Hyponatremia
D. Rerupture of the coiled aneurysm
E. Vasospasm
The answer is E. Nontraumatic subarachnoid hemorrhage (SAH) occurs most often following rupture of a saccular, or berry, aneurysm. Autopsy and angiography studies have identified aneurysms in 2% of the adult population, affecting 4 million individuals. The yearly incidence of SAH due to aneurysmal rupture is 20,000–30,000 cases. Many patients die before reaching the hospital. If a patient survives to hospital admission, the 28-day mortality rate is 45%. More than half of individuals who survive have significant neurologic injury with lingering manifestations. The patient with SAH should be admitted to a critical care unit with expertise in managing SAH. Initial treatment of SAH includes early aneurysmal repair while managing intracranial hypertension. Repair of the aneurysm may be accomplished via neurosurgical clipping or endovascular coiling of the aneurysm. Generally coiling has shown improved functional outcomes in those undergoing endovascular procedures. Medical management is complex. Intracranial hypertension is common and frequently requires management with ventriculostomy. Medical management of elevated intracranial pressure is also often required. If a patient survives the initial period following SAH, the patient is vulnerable to several causes of delayed neurologic deficits that typically present within 1–2 weeks after the event. Vasospasm refers to narrowing of the arteries at the base of the brain following SAH and is the most common cause of delayed morbidity and mortality in SAH. Signs of ischemic injury and change in neurologic examination herald the development of vasospasm. Nimodipine is typically prescribed at a dose of 60 mg every 4 hours on admission to the intensive care unit to attempt to prevent vasospasm. Vasospasm can be detected by x-ray angiography or transcranial Doppler ultrasound. Surveillance for vasospasm is often performed via transcranial Doppler ultrasound on a daily or every-other-day basis.
100
A 27-year-old woman is admitted to the hospital with acute-onset severe right upper quadrant pain that radiates to the back. The pain is constant and not relieved with eating or bowel movements. Her labs show marked elevation in amylase and lipase, and acute pancreatitis is diagnosed. Which of the following is the best first test to demonstrate the etiology of her pancreatitis?
A. Right upper quadrant ultrasound
B. Serum alcohol level
C. Serum triglyceride level
D. Technetium hepatobiliary iminodiacetic acid scan
E. Urine drug screen
The answer is A. The most common cause of acute pancreatitis in the United States is gallstones causing common bile duct obstruction. Although bile duct obstruction may be demonstrated on technetium hepatobiliary iminodiacetic acid scan, right upper quadrant ultrasound is preferred for ease, demonstration of gallstones in the gallbladder, and demonstration of obstructed bile duct. Alcohol is the second most common cause of acute pancreatitis, followed by complications of endoscopic retro- grade cholangiopancreatography. Hypertriglyceridemia accounts for 1–4% of cases of acute pancreatitis with triglyceride levels usually >1000 mg/dL. Other potential com- mon causes include trauma, surgery, drugs such as valproic acid, anti-HIV medications, estrogens, and sphincter of Oddi dysfunction. Additionally, a number of rare causes have been described. The most judicious first step in evaluation of acute pancreatitis is to test for gallstones and pursue more rare causes after the most common cause has been ruled out.
100
You are seeing Mr. DeWinter, a 71-year-old man, for changes in mental status and cognition. His wife reports that he has slowly been worsening over the last year or two. He has frequent visual hallucinations, sleeps heavily during the daytime but not well at night, and has delusions of persecution. He was noted to have some Parkinsonian features previously and was started on L-dopa, but quickly developed a hallucinatory delirium requiring cessation of L-dopa. He does not have orthostatic hypotension or syncope. Which of the following diseases best fits his dementia syndrome?
A. Alzheimer’s disease
B. Delirium
C. Dementia with Lewy bodies
D. Multiple systems atrophy with parkinsonism
E. Normal aging
The answer is C. The dementia with Lewy bodies (DLB) syndrome is characterized by visual hallucinations, parkinsonism, fluctuating alertness, neuroleptic sensitivity, rapid eye movement sleep behavior disorder (RBD), and often hyposmia and excessive daytime sleepiness. Delusions related to persecution, invasion, and person or place identity (reduplicative paramnesia) are common. When orthostatic hypotension is present, DLB must be distinguished from multiple system atrophy with parkinsonism (MSA-P). Recurrent, disabling syncope early in the course, accompanied by laryngeal spasms and anterocollis, suggest MSA-P. In DLB, orthostasis can appear early but rarely becomes disabling until well into the course, when neuropsychiatric symptoms and cognitive dysfunction are well established. Patients with DLB and Parkinson disease dementia are highly sensitive to metabolic perturbations, and in some patients the first manifestation of illness is a delirium, often precipitated by an infection, new medicine, or other systemic disturbance. A hallucinatory delirium induced by L-dopa, prescribed for parkinsonian symptoms attributed to Parkinson disease, may likewise provide the initial clue to a DLB diagnosis. Due to the frequent comorbidity with Alzheimer’s disease and the cholinergic deficit in DLB, cholinesterase inhibitors often provide significant benefit, reducing hallucinosis, stabilizing delusional symptoms, and even helping with RBD in some patients. Exercise programs maximize motor function and protect against fall-related injury. Antidepressants are often necessary. Atypical antipsychotics may be required for psychosis but can worsen extrapyramidal syndromes, even at low doses, and should be used cautiously, given the side effects, including an increased risk of death.
200
Which of the following physical examination findings are associated with severe aortic stenosis?
A. A delayed and weak carotid pulse
B. Augmentation of the murmur with Valsalva
C. Bounding femoral pulsation
D. Holosystolic murmur at the apex radiating to the axilla
E. Pan-cycle murmur at the apex
The answer is A. A delayed and weak carotid pulse is typical in cases of severe aortic stenosis. The carotid arterial pulse rises slowly to a delayed peak (pulsus parvus et tardus). In the late stages, when stroke volume declines the systolic pressure may fall and the pulse pressure will narrow. Augmentation of the murmur with Valsalva (left ventricular preload reduction) occurs in hypertrophic cardiomyopathy with out- flow tract obstruction. Bounding femoral pulse is commonly felt in aortic regurgitation. Option D describes the murmur of mitral regurgitation, whereas option E might be a heart with a ventricular aneurysm or ventricular septal defect.
200
A 56-year-old woman is admitted to the intensive care unit with a 4-day history of increasing shortness of breath and cough with copious sputum production. She has known severe chronic obstructive pulmonary disease with an FEV1 of 42% predicted. On presentation, she has a room air blood gas with a pH of 7.26, PaCO2 of 78 mmHg, and PaO2 of 50 mmHg. She is in obvious respiratory distress with use of accessory muscles and retractions. Breath sounds are quiet with diffuse expiratory wheezing and rhonchi. No infiltrates are present on chest radiograph. Which of the following therapies has been demonstrated to have the greatest reduction in mortality rate for this patient?
A. Administration of inhaled bronchodilators
B. Administration of IV glucocorticoids
C. Early administration of broad-spectrum antibiotics with coverage of Pseudomonas eruginosa
D. Early intubation with mechanical ventilation
E. Use of noninvasive positive-pressure ventilation
The answer is E. Acute exacerbations of chronic obstructive pulmonary disease (COPD) are marked by an increase in dyspnea, an increase in sputum, and a change in sputum color. Acute exacerbations of COPD account for substantial healthcare expenditures annually in the United States, with significant morbidity and mortality associated with these exacerbations. Prompt treatment can improve symptoms and decrease hospitalizations and mortality in this setting. In patients presenting with hypercarbic respiratory failure in the setting of an acute exacerbation, the treatment that has demonstrated the strongest reduction in mortality, when compared with traditional mechanical ventilation, is noninvasive positive-pressure ventilation (NIPPV). NIPPV also decreases the need for endotracheal intubation, complications, and length of stay in the hospital. Antibiotics, bronchodilators, and glucocorticoids are all cornerstones of therapy in the treatment of acute exacerbations in COPD but have not been demonstrated in clinical trials to have similar mortality benefits in the situation of acute hypercarbic respiratory failure. Specifically, no benefit is demonstrated for IV versus oral corticosteroids. Likewise, the choice of antibiotic should be made based on local susceptibility patterns, and the need for broad-spectrum antibiotics that cover for Pseudomonas spp. is not typically indicated. Recent studies have demonstrated that high-flow nasal oxygen may be an effective alternative to NIPPV, with improved outcomes (need for mechanical ventilation) and improved patient comfort.
200
A 33-year-old previously healthy woman presents to the emergency department with malaise, confusion, and fever of 37.8°C (100.1°F). She had no preceding diarrheal illness. CT of the head is unremarkable. She is found to have platelets of 13,000/cu, hemoglobin of 9.0 g/dL, and creatinine of 2.3 mg/dL. Urinalysis shows pH 5.0, protein 1+, and 11 red blood cells/high-powered field. Which of the following laboratory findings would be expected with her diagnosis?
A. ADAMSTS13 <10%
B. Anti-glomerular basement membrane antibodies
C. Decreased lactate dehydrogenase
D. Positive direct Coombs test
E. Spherocytes on peripheral blood smear
The answer is A. Thrombotic thrombocytopenic purpura (TTP) and hemolytic- uremic syndrome (HUS) represent a spectrum of thrombotic microangiopathies. TTP and HUS share the general features of idiopathic thrombocytopenic purpura, microan- giopathic hemolytic anemia, fever, renal failure, and neurologic disturbances. Schistocytes, not spherocytes, are typical on peripheral smear. When patients, particularly children, have more evidence of renal injury, their condition tends to be called HUS. In adults with neurologic disease, it is considered to be TTP. In adults there is often a mixture of both, which is why they are often referred to as having TTP/HUS. In familial cases of adult TTP/HUS, there is a genetic deficiency of the ADAMTS13 metalloprotease that cleaves large multim- ers of von Willebrand factor. When ADAMTS13 is absent, these large multimers cause platelet clumping and intravascular hemolysis. In the setting of intravascular hemolysis an elevated lactate hydrogenase is usually seen as well as schistocytes on peripheral blood smear. An antibody to ADAMTS13 is found in many sporadic cases of adult TTP/HUS, but not all; many patients also have antibodies to the thrombospondin receptor on selected endothelial cells in small vessels or increased levels of plasminogen-activator inhibitor 1. Patients can be tested for ADAMTS13 activity and, if low, the presence of antibodies to ADAMTS13 distinguishes the deficiency from the immune-mediated disease. Antibodies to red blood cells (positive direct coombs test) are not typically seen in TTP. Anti-glomerular basement membrane antibodies are seen in Goodpasture syndrome, which presents with acute glomerulonephritis and alveolar hemorrhage.
200
Which of the following molecules directly activates osteoclast progenitors leading to increased bone resorption and is a target of an osteoporosis treatment drug?
A. Fibroblast growth factor 2
B. Insulin-like growth factor-1
C. Parathyroid hormone
D. RANK ligand
The answer D. Resorption of bone is carried out mainly by osteoclasts, multinucleated cells that are formed by fusion of cells derived from the common precursor of macrophages and osteoclasts. Thus, these cells derive from the hematopoietic lineage, quite different from the mesenchymal cells that become osteoblasts. Multiple factors that regulate osteoclast development have been identified. RANK ligand, a member of the tumor necrosis factor family, is expressed on the surface of osteocytes, osteoblasts, and stromal fibroblasts. In a process involving cell-cell interactions, RANK ligand binds to the RANK receptor on osteoclast progenitors, stimulating osteoclast differentiation and activation. Denosumab is a monoclonal antibody targeting RANK ligand. Osteoblasts synthesize and secrete the organic matrix and regulate its mineralization. They are derived from cells of mesenchymal origin. Osteocytes regulate osteoblasts partly by secreting a potent inhibitor of Wnt signaling called sclerostin. Numerous other growth-regulatory factors affect osteoblast function, including the three closely related transforming growth factor βs, fibroblast growth factors 2 and 18, platelet-derived growth factor, and insulin-like growth factors 1 and 2.
300
You are seeing Mr. Johnson who is a 24-year-old previously healthy marathon runner. He is in for his employer-required physical examination. Which of the following rhythms is demonstrated in the given figure?

A. First-degree heart block
B. Mobitz type I, second-degree heart block
C. Mobitz type II, second-degree heart block
D. Normal sinus rhythm
E. Type III heart block
The answer is B. This is Mobitz type I second-degree heart block, or Wenckebach heart block. The periodic failure of conduction in Mobitz type I block is characterized by a progressively lengthening PR interval, shortening of the RR inter- val, and a pause that is less than two times the immediately preceding RR interval on the electrocardiogram (ECG). The ECG complex after the pause exhibits a shorter PR interval than that immediately preceding the pause. This ECG pattern most often arises because of decremental conduction of electrical impulses in the atrioventricular node. This rhythm is usually benign and may be seen in very fit athletes due to high vagal tone.
300
Ms. Puhl, a 32-year-old woman with a long-standing history of asthma, comes to the emergency department complaining of shortness of breath typical of her asthma exacerbations after visiting a friend who had seven cats in the house. On examination, she has diffuse bilateral polyphonic wheezes and is using accessory muscles to breathe. Her initial arterial blood gas on room air shows a pH of 7.34, PaCO2 of 32 mmHg, and PaO2 of 48 mmHg. After placing her on 40% oxygen by face mask, a repeat PaO2 is 200 mmHg and PaCO2 is 32 mmHg. The most likely cause of her initial hypoxemia was:
A. Alveolar hypoventilation
B. Diffusion defect
C. Increased dead space
D. Shunt
E. Ventilation-perfusion mismatch
The answer is E. This patient with asthma presents with hypoxemia and a reduced PaCO2. A low PaCO2 rules out hypoventilation as the cause of her initial hypoxia. Increased dead space alone would not affect oxygenation and would be expected to result in an increased PaCO2 if alveolar ventilation was not increased to compensate. After being placed on oxygen, the PaO2 increases notably, which argues against shunt physiology since a shunt does not substantially correct with supplemental oxygen. Asthma is characterized by airways hyper-reactivity that leads to areas of ventilation-perfusion mismatch. Hypoxemia results from areas of low ventilation with normal to high perfusion. This can be eas- ily corrected with supplemental oxygen. Asthma does not reduce the surface area for gas exchange in the lung. In fact, during periods of hyperinflation as might occur in asthma, the diffusing capacity may be increased.
300
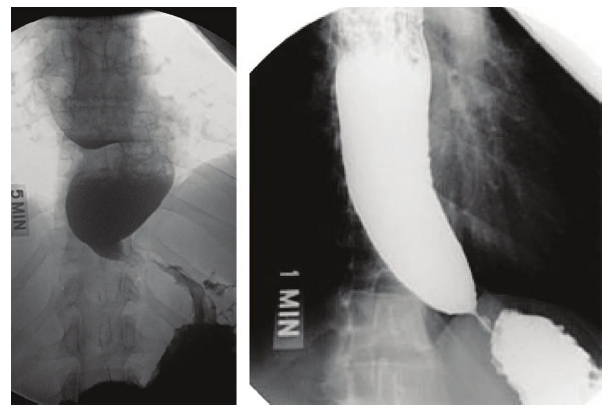
A 43-year-old man presents with 6 months of worsening dysphagia and postprandial regurgitation. He reports difficulty and pain with swallowing both liquids and solids; he has no difficulty with the initial components of swallowing but reports pain in the mid-chest region. He frequently regurgitates undigested food 20–60 minutes after eating or drinking. In the past 2 months, he has lost 15 lb. He also has had one episode of presumed pneumonia 4 months ago notable for a right lower lobe infiltrate. He has no significant past medical history, takes no medications, and does not smoke cigarettes. He works as a service representative at a major electronics store and has never left the United States. Other than signs of recent weight loss, his physical examination is unremarkable. A barium swallow is performed and shown in the figure. Which of the following is the most likely cause of his disease?
A. Autoimmune reaction to latent herpes virus
B. Diffuse spasm on smooth muscle
C. Infection by Trypanosoma cruzi
D. Malignant growth of columnar epithelial cells
E. Malignant growth squamous epithelial cells
The answer is A. The barium swallow image demonstrates achalasia with esophageal dilation narrowing at the gastroesophageal junction and an air-fluid level in the mid-esophagus. Achalasia is a rare disease caused by loss of ganglion cells within the esophageal myenteric plexus with a population incidence of about 1:100,000; it usually presents between age 25 and 60. With long-standing disease, aganglionosis is noted. The disease involves both excitatory (cholinergic) and inhibitory (nitric oxide) ganglionic neurons. This leads to impaired deglutitive lower esophageal sphincter (LES) relaxation and absent peristalsis. Increasing evidence suggests that the ultimate cause of ganglion cell degeneration in achalasia is an autoimmune process attributable to a latent infection with human herpes simplex virus 1 combined with genetic susceptibility. Long-standing achalasia is characterized by progressive dilatation and sigmoid deformity of the esophagus with hypertrophy of the LES. Clinical manifestations may include dys- phagia, regurgitation, chest pain, and weight loss. Most patients report solid and liquid food dysphagia. Regurgitation occurs when food, fluid, and secretions are retained in the dilated esophagus. Patients with advanced achalasia are at risk for bronchitis, pneumo- nia, or lung abscess from chronic regurgitation and aspiration. The differential diagnosis of achalasia includes diffuse esophageal spasm, Chagas disease, and pseudo-achalasia. Chagas disease is endemic in areas of central Brazil, Venezuela, and northern Argen- tina and spread by the bite of the reduviid (kissing) bug that transmits the protozoan Trypanosoma cruzi. The chronic phase of the disease develops years after infection and results from destruction of autonomic ganglion cells throughout the body, including the heart, gut, urinary tract, and respiratory tract. Tumor infiltration, most commonly seen with carcinoma in the gastric fundus or distal esophagus, can mimic idiopathic achalasia. The resulting pseudo-achalasia accounts for up to 5% of suspected cases and is more likely with advanced age, abrupt onset of symptoms (<1 year), and weight loss. Hence, endoscopy is a necessary part of the evaluation of achalasia. When the clinical suspicion for pseudo-achalasia is high and endoscopy nondiagnostic, CT scanning or endoscopic ultrasound may be of value. There is no known way of preventing or reversing achalasia. Therapy is directed at reducing LES pressure so that gravity and esophageal pressurization promote esophageal emptying. Peristalsis rarely, if ever, recovers. Botulinum toxin, injected into the LES under endoscopic guidance, inhibits acetylcholine release from nerve endings and improves dysphagia in about 66% of cases for at least 6 months. The only durable therapies for achalasia are pneumatic dilatation and Heller myotomy.
300
A 40-year-old woman with systemic lupus erythematosus (SLE) presents to the clinic with proximal and distal leg weakness and sensory loss in her feet that has been present for several months. She has not had pain or burning in her feet, just decreased sensation. She has been treated with hydroxychloroquine and mycophenolate mofetil for 10 years for her SLE. She does not take other medications. Electromyography demonstrates myopathic muscle action potentials in the proximal muscles and reduced recruitment in more distal muscles. Nerve conduction study shows a reduction in amplitude. Lumbar puncture does not show elevated protein or white blood cells. Which of the following is the most likely cause of her neurologic symptoms?
A. Chronic inflammatory demyelinating polyneuropathy
B. Guillain-Barré syndrome
C. Hydroxychloroquine toxicity
D. Multiple sclerosis
E. Small fiber neuropathy from SLE
The answer is C. Hydroxychloroquine can cause a toxic myopathy characterized by slowly progressive, painless, proximal weakness and atrophy, which is worse in the legs than in the arms. In addition, neuropathy can also develop with or without the myopathy leading to sensory loss and distal weakness. The “neuromyopathy” usually appears in patients taking 500 mg daily for a year or more but has been reported with doses as low as 200 mg/d. Serum creatine kinase levels are usually elevated due to the superimposed myopathy. Nerve conduction studies (NCSs) reveal mild slowing of motor and sensory nerve conduction velocities with a mild to moderate reduction in the amplitudes, although NCSs may be normal in patients with only myopathy. Electromyography demonstrates myopathic muscle action potentials (MUAPs), increased insertional activity in the form of positive sharp waves, fibrillation potentials, and occasionally myotonic potentials, particularly in the proximal muscles. Neurogenic MUAPs and reduced recruitment are found in more distal muscles. In this patient clinical and NCS findings consistent with hydroxychloroquine myopathy and neuropathy. Between 2 and 27% of individuals with systemic lupus erythematosus develop peripheral neuropathy. Affected patients typically present with a slowly progressive sensory loss beginning in the feet. Some patients develop burning pain and paresthesia with normal reflexes, and NCSs suggest a pure small-fiber neuropathy. Less common are multiple mononeuropathies presumably secondary to necrotizing vasculitis. Rarely, a generalized sensorimotor polyneuropathy meeting clinical, laboratory, electrophysiologic, and histologic criteria for either Guillain-Barré syndrome (GBS) or chronic inflammatory demyelinating polyneuropathy (CIDP)may occur. A patient with GBS or CIDP would be expected to have an abnormal lumbar puncture. Similarly, the normal lumbar puncture and clinical presentation is not consistentwith multiple sclerosis.
400
Mr. Jones is a 21-year-old man who presents to the emergency room with several days of worsening shortness of breath and lethargy after 1 week after a viral upper respiratory tract infection. His family brought him in after he lacked the energy to rise from the couch unassisted. His blood pressure is 88/72, heart rate is 115 beats/min, and room air oxygen saturation is 90%. Physical examination reveals pulmonary crackles, elevated jugular venous pressure, an audible S3 gallop, and cool extremities. He is lethargic and slow to respond to questions. Laboratory analysis reveals a creatinine of 2.3 mg/dL, elevated B-type natriuretic peptide level, and mildly elevated lactate. Bedside echocardiography reveals a left ventricular ejection fraction of 15% with global hypokinesis. You start dobutamine at 5 μg/kg per minute and prepare to insert a pulmonary artery catheter for hemodynamic monitoring. Before starting dobutamine, which of the following hemodynamic parameters is most likely increased and should decrease with therapy?
A. Cardiac output
B. Left ventricular stroke work index
C. Mixed venous oxygen saturation
D. Stroke volume
E. Systemic vascular resistance
The answer is E. The utility of invasive hemodynamic monitoring during acute decompensated heart failure has been highly scrutinized recently. Based on several observational and randomized trials, the routine use of a pulmonary artery catheter is not recommended and should be restricted to those who respond poorly to diuresis or experi- ence hypotension or signs and symptoms suggestive of a low cardiac output where thera- peutic targets are unclear. In this patient with hypotension and signs of low cardiac output, invasive monitoring will allow the clinician to rapidly, objectively assess any changes in hemodynamic status and respond appropriately. In states of “cold” (poor perfusion) and “wet” (elevated filling pressures, or hypervolemia) heart failure, the stroke volume and cardiac output are decreased. Left ventricular stroke work index (a calculated value which normalizes left ventricular work for the patient’s body surface area and afterload) is also diminished. Mixed venous oxygen saturation is greatly diminished as well, as the Fick equation dictates that cardiac output is proportional to the venous oxygen saturation if oxygen consumption and arterial oxygen saturation are normal. Systemic vascular resistance equals the (mean systemic arterial pressure – mean right atrial pressure) divided by cardiac output. As cardiac output drops, the systemic vasculature will increase its resist- ance to attempt to maintain blood pressure and end-organ perfusion pressure. However, this initially compensatory action becomes deleterious as an inefficient left ventricle must work against an ever-increasing afterload. The most effective inotropic agents in acute decompensated heart failure (milrinone and dobutamine) also have vasodilatory properties to combat this harmful systemic vascular resistance increase.
400
A 34-year-old woman seeks evaluation for a complaint of cough and dyspnea on exertion that has gradually worsened over 3 months. The patient has no past history of pulmonary complaints and has never had asthma. She started working in a pet store approximately 6 months ago. Her duties there include cleaning the reptile and bird cages. She reports occasional low-grade fevers but has had no wheezing. The cough is dry and non-productive. Before 3 months ago, the patient had no limitation of exercise tolerance, but now she reports that she gets dyspneic climbing two flights of stairs. On physical examination, the patient appears well. She has an oxygen saturation of 95% on room air at rest but desaturates to 89% with ambulation. Temperature is 37.7°C (99.8°F). The pulmonary examination is unremarkable. No clubbing or cyanosis is present. The patient has a normal chest radiogram. A high-resolution chest CT shows diffuse ground-glass infiltrates in the lower lobes with the presence of centrilobular nodules. A transbronchial biopsy shows an interstitial alveolar infiltrate of plasma cells, lymphocytes, and occasional eosinophils. There are also several loose noncaseating granulomas. All cultures are negative for bacterial, viral, and fungal pathogens. What treatment do you recommend for the patient?
A. Amphotericin
B. Doxycycline
C. Glucocorticoids
D. Glucocorticoids plus azathioprine
E. Glucocorticoids plus removal of antigen
The answer is E. The patient has a subacute presentation of hypersensitivity pneumonitis related to exposure to bird droppings and feathers at work. Hypersensitivity pneumonitis is a delayed-type hypersensitivity reaction that has a variety of presentations. Some people develop acute onset of shortness of breath, fevers, chills, and dyspnea within 6–8 hours of antigen exposure. Others may pre- sent subacutely with worsening dyspnea on exertion and dry cough over weeks to months. Chronic hypersensitivity pneumonitis presents with more severe and persistent symptoms along with clubbing. Progressive worsening is common with the development of chronic hypoxemia, pulmonary hypertension, interstitial pulmonary fibrosis, and respiratory failure. The diagnosis relies on a variety of tests. Peripheral eosinophilia is not a feature of this disease as the disease is mediated through T-cell inflammation. Other nonspecific markers of inflammation may be elevated, including the erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, and serum immunoglobulins. Neutrophilia and lymphopenia can be seen. If a specific antigen is suspected, serum precipitins directed toward that antigen may be demonstrated. However, these tests are neither sensitive nor specific for the presence of disease. Chest radiography may be normal or show a diffuse reticulonodular infiltrate. Chest CT is the imaging modality of choice and shows ground-glass infiltrates in the lower lobes. Centrilobular infiltrates are often seen as well. In the chronic stages, patchy emphysema is the most common finding. Histopathologically, interstitial alveolar infiltrates predominate, with a variety of lymphocytes, plasma cells, and occasionally eosinophils and neutrophils seen. Loose, noncaseating granulomas are typical. Treatment requires removing the individual from exposure to the antigen. If this is not possible, the patient should wear a mask that prevents small-particle inhalation during exposure. In patients with mild disease, removal from antigen exposure alone may be sufficient to treat the disease. More severe symptoms require therapy with glucocorticoids at an equivalent prednisone dose of 1 mg/kg daily for 7–14 days. The steroids are then gradually tapered over 2–6 weeks.
400
A patient with a history of Sjögren syndrome has the following laboratory findings: plasma sodium 139 mEq/L, chloride 112 mEq/L, bicarbonate 15 mEq/L, and potassium 3.0 mEq/L. Urine studies show a pH of 6.0, sodium of 15 mEq/L, potassium of 10 mEq/L, and chloride of 12 mEq/L. What is the most likely diagnosis?
A. Chronic diarrhea
B. Type I renal tubular acidosis (RTA)
C. Type II RTA
D. Type III RTA
E. Type IV RTA
The answer is B. This patient has a normal anion gap metabolic acidosis (anion gap, 12). The calculated urine anion gap (Na + K – Cl ) is +3; thus, the acidosis is unlikely to be due to gastrointestinal bicarbonate loss. In this patient, the diagnosis is type I renal tubular acidosis (RTA), or distal RTA. This is a disorder in which the distal nephron does not lower pH normally. It is associated with a urine pH >5.5, hypokalemia, and lack of bicarbonaturia. Sjögren syndrome is one of the autoimmune diseases (along with systemic lupus erythematosus, granulomatous interstitial nephritis, IgG4-related systemic disease, and idiopathic autoimmune interstitial nephritis) that may be associated with acute interstitial nephritis and tubular dysfunction. Sjögren-associated type I RTA may be associated with calcium phosphate stones and nephrocalcinosis. Type II RTA, or proximal RTA, includes a pH <5.5, hypokalemia, a positive urine anion gap, bicarbonaturia, hypophosphatemia, and hypercalciuria. This condition results from defective resorption of bicarbonate. Type III RTA is rare and most commonly is seen in children. Type IV RTA is also referred to as hyperkalemic distal RTA. Hyporeninemic hypoaldosteronism is the most common cause of type IV RTA and is usually associated with diabetic nephropathy.
400
A 60-year-old man presents to the emergency department with numbness and weakness in his legs and feet. On examination, you find that he is numb to the knees and has marked weakness in ankle dorsiflexion and plantar flexion. Two years ago, he developed diabetes, and last year, he was admitted when found to be profoundly hypothyroid. On examination, he has hepatosplenomegaly and appears to have a dark tan despite having no sun exposure recently. Which of the following tests will likely help make his diagnosis?
A. Anti-nuclear antibody titer measurement
B. Antithymoglobulin antibody titer measurement
C. Blood cultures
D. Serum protein electrophoresis
E. Skin biopsy searching for intravascular clonal T cells
The answer is D. This patient likely has polyneuropathy, organomegaly, endo- crinopathy, M-protein, and skin changes (POEMS). Patients usually present with a pro- gressive sensorimotor polyneuropathy, diabetes mellitus (50%), primary gonadal failure (70%), and a plasma cell dyscrasia with sclerotic bony lesions. Associated findings can be hepatosplenomegaly, lymphadenopathy, and hyperpigmentation. Patients often present in the fifth and sixth decades of life and have a median survival after diagnosis of less than 3 years. The detection of an M-protein on serum electrophoresis would make POEMS the most likely diagnosis.
500
Mr. Rhodes is a 45-year-old man who presented to his primary care physician with 4 months of worsening dyspnea. Pulmonary function tests and CT chest are normal. Echocardiogram shows elevated right ventricular systolic pressure estimates by Doppler velocities and left ventricular diastolic dysfunction with normal systolic function. Based on this information he undergoes a right heart catheterization. Hemodynamics are shown below.
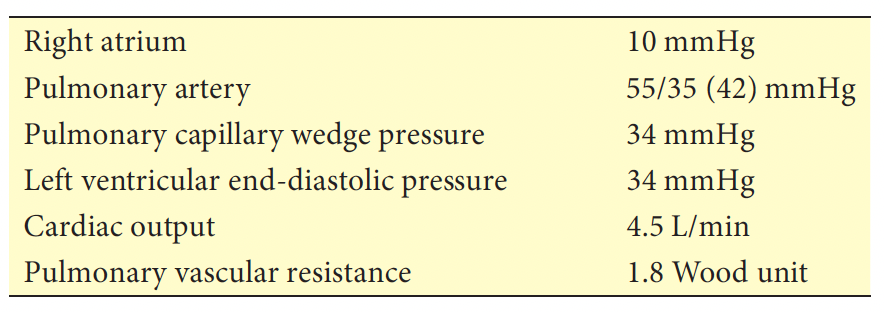
Which of the following is the most likely cause of Mr. Rhodes’ pulmonary hypertension?
A. Chronic lung disease
B. Chronic thromboembolic pulmonary hypertension
C. Heart failure with preserved ejection fraction
D. Idiopathic pulmonary arterial hypertension
The answer is C. Normal pulmonary function tests and CT scan make chronic lung disease unlikely. The elevated pulmonary capillary wedge pressure rules out idiopathic pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension, as it is normal in those disorders. The identical wedge pressure and left ventricular end-diastolic pressure render mitral stenosis unlikely, because with signifi- cant mitral stenosis there should be a gradient between the pulmonary capillary wedge pressure and end-diastolic left ventricle pressure. These results are consistent with post- capillary pulmonary hypertension (or pulmonary venous hypertension) due to left heart disease. Whatever the cause of elevated left atrial pressure (i.e., systolic or diastolic heart failure or valvular disease), the increased pulmonary venous pressure indirectly leads to a rise in pulmonary arterial pressure. The catheterization results combined with the normal left ventricular ejection fraction on echocardiogram make heart failure with preserved ejection fraction the most likely etiology of his pulmonary hypertension. The presence of pulmonary hypertension portends a poor prognosis in all forms of heart failure.
500
A 32-year-old female is admitted to the intensive care unit with respiratory failure secondary to influenza pneumonia. She is intubated and sedated. Her initial ventilator settings are volume control with a respiratory rate of 35, tidal volume (TV) of 420 mL, FiO2 of 0.60, and positive end-expiratory pressure (PEEP) of 12 cmH2O. Her blood gas after 30 minutes on those settings reveals a pH of 7.21, PCO2 of 65, and PaO2 of 65. Her plateau pressure is 22 cmH2O. Her blood pressure is 110/65, her heart rate is 105 beats/min, and her saturation is 91%. Her ideal body weight is 70 kg. What is the most appropriate next step in terms of ventilator management?
A. Increase FiO2 to 80%
B. Increase PEEP to 14 cmH2O
C. Increase respiratory rate to 40 breaths/min
D. Increase TV to 480 mL
E. Maintain current settings
The answer is E. This patient with acute respiratory distress syndrome (ARDS) is appropriately receiving low tidal volume ventilation and as a result has developed a respiratory acidosis. However, she is tolerating this acidosis from a hemodynamic standpoint so there is no reason to treat this permissive hypercapnia. Increasing the tidal volume would increase her plateau pressure and put her at greater risk of ventilator- induced lung injury. Increasing her respiratory rate to 40 would increase the possibility of air trapping with resulting auto-positive end-expiratory pressure (PEEP), and would likely lead to patient-ventilator dyssynchrony. There is no need to increase her FiO2 as her PaO2 and saturation are adequate. Increasing PEEP would possibly increase her plateau pressure and would not be indicated because she is already adequately oxygenating. The best thing to do would be to leave her ventilator settings where they are for the time being.
500
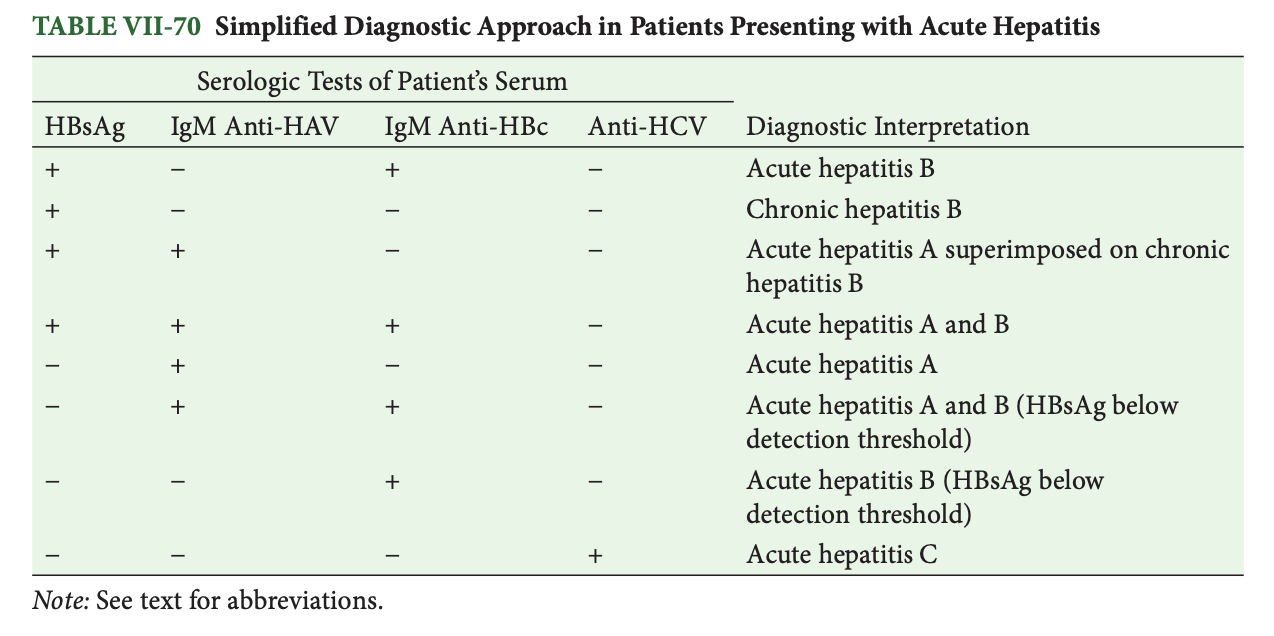
A 34-year-old man presents to the physician complaining of yellow eyes. For the past week, he has felt ill, with decreased oral intake, low-grade fevers (~100°F), fatigue, nausea, and occasional vomiting. With the onset of jaundice, he has noticed pain in his right upper quadrant. He currently uses marijuana and ecstasy and has a prior history of injection drug use with cocaine. He has no other past medical history, but he was unable to donate blood for reasons that he cannot recall 4 years previously. His social history is remarkable for working as a veterinary assistant. On sexual history, he reports five male sexual partners over the past 6 months. He does not consistently use condoms. On physical examination, he appears ill and has obvious jaundice with scleral icterus. His liver is 15 cm to percussion, palpable 6 cm below the right costal margin. The edge is smooth and tender to palpation. The spleen is not enlarged. There are no stigmata of chronic liver disease. His aspartate aminotransferase is 1232 IU/L, alanine aminotransferase is 1560 IU/L, alkaline phosphatase is 394 IU/L, total bilirubin is 13.4 mg/dL, and direct bilirubin is 12.2 mg/dL. His international normalized ratio is 2.3, and activated partial thromboplastin time is 52 seconds. Hepatitis serologies are sent and reveal the following:
Hepatitis A IgM: negative
Hepatitis A IgG: negative
Hepatitis B core IgM: positive
Hepatitis B core IgG: negative
Hepatitis B surface antigen: positive
Hepatitis B surface antibody: negative
Hepatitis B e antigen: positive
Hepatitis B e antibody: negative
Hepatitis C antibody: positive
What is the cause of the patient’s current clinical presentation?
A. Acute hepatitis A infection
B. Acute hepatitis B infection
C. Acute hepatitis C infection
D. Chronic hepatitis B infection
E. Drug-induced hepatitis
The answer is B.
500
A 39-year-old man comes to the clinic complaining of blistering skin lesions on the backs of his hands and arms that are painful. They are often precipitated by sunlight and heal with scarring. He also notices that they often occur after drinking alcohol heavily. His hands and forearms have numerous hypopigmented scars that he says are from previous episodes. The skin over the back of his hands appears thick and coarse. Otherwise his review of systems and physical examination are normal. The lesions on his hands are shown in the figure. Testing confirms your suspected diagnosis. Which of the following treatments will most likely lead to long-term improvement for this patient?

A. Avoidance of sun exposure and IV hemin for treatment of acute lesions
B. Hydroxychloroquine 200 mg twice daily
C. Phlebotomy of 450 mL of blood every 1–2 weeks
D. Prednisone 0.5 mg/kg orally daily
E. Triamcinolone 0.5% topically twice daily
The answer is C. This patient has porphyria cutanea tarda (PCT), the most common of the porphyrias. Although PCT can be inherited, it most commonly occurs sporadically and is associated with a defect in hepatic uroporphyrinogen (URO) decar- boxylase. For clinical symptoms to be present, the patient needs to have less than 20% of normal enzyme activity, and PCT occurs when an individual develops an inhibitor of URO decarboxylase in the liver. The majority of PCT patients have no mutations in URO decarboxylase. The major clinical feature of PCT is blistering skin lesions predominantly affecting the back of the hands that also may involve the forearms, face, legs, and feet. The lesions start as blisters that rupture and crust over, leaving scarring. Chronically, the areas most involved can develop thickened skin similar to systemic sclerosis. Precipitating fac- tors for development of lesions include hepatitis C, HIV, excess alcohol, elevated iron lev- els, and estrogens. Diagnosis of PCT is made by measuring porphyrin levels, which would demonstrate elevated plasma, urine, and fecal porphyrins. Liver levels of porphyrins are also high. Urinary 5-aminolevulinic acid level may be slightly elevated, but the urinary porphobilinogen level is normal. In addition to avoiding precipitating factors, treatment of PCT is primarily through phlebotomy every 1–2 weeks to achieve a low-normal ferritin level. With this approach, a complete remission can almost always be achieved, typically after only five to six phlebotomies. After remission, continued phlebotomy may not be required, but plasma porphyrin levels should continue to be followed every 6–12 months to assess for recurrence. An alternative effective treatment is the antimalarial drugs chloroquine or hydroxychloroquine. These drugs complex with the excess porphyrins and promote their excretions. Doses typically are lower in PCT because standard doses may actually worsen symptoms transiently. Recent studies have shown that hydroxychloroquine may be as safe and effective as phlebotomy, although phlebotomy remains the standard of care at this time. None of the other treatments, including hemin, are used in the treatment of PCT.