Bleeding out
heme onc honkey tonk
Am I anemic or just tired from PA school??
Name that smear
other heme
100
What is indicated if a PT/PTT does NOT normalize after a mixing study?
Mixing study determines if change in PT/PTT is due to factor deficiency
If PT/PTT normalizes then change is due to a factor deficiency
But if it does NOT normalize then there is a factor inhibitor- antibodies that are neutralizing clotting factors (most commonly anticoag meds!)
100
Name the "B" symptoms.
Fever + night sweats + weight loss
Presence of these symptoms can support further work up of a possible leukemia or lymphoma diagnosis
100
Koilonychia is most consistent with a deficiency in which of the following?
Spoon shaped, concave nails from chronic iron deficiency
Other sxs of iron deficiency: fatigue, weakness, headaches, tinnitus, pica
PE findings: pale mucosa, loss of tongue papillae, angular cheilitis, esophageal webs
100

G6PD deficiency
Bite cells and upper left corner are heinz bodies
oxidative hemolysis- oxidative stress causes hemoglobin to denature and form heinz bodies. When the RBC pass through the spleen the macrophages bite out the heinz body and form the bite cells!
100
What medication increases fetal hemoglobin and reduces sickling of RBCs?
Hydroxyurea
200
A 27 year-old male nonsmoker is diagnosed with upper extremity venous thrombosis. What is the most likely coag abnormality found in this patient?
Factor V Leiden
Mutated factor V resistant to breakdown by activated Protein C - results in hypercoagulability.
Most common hypercoagulopathy
- Rule out in patients with multiple DVTs, TIAs with no other risk factors
200
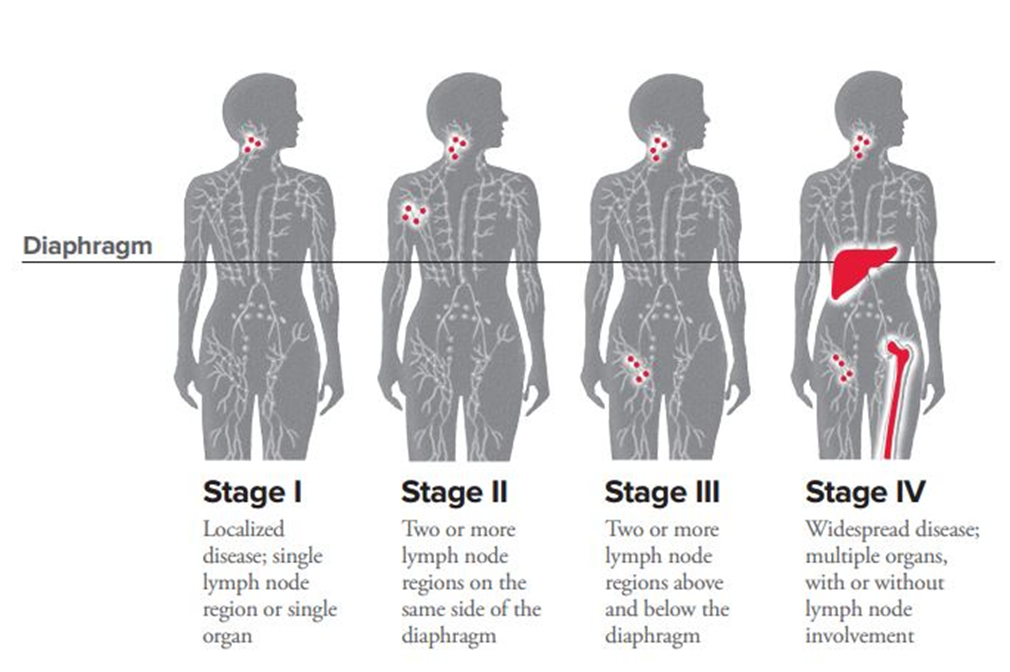
What stage of lymphoma diagnosis is a patient who is found to have right cervical lymph node and inguinal lymph node involvement?
Stage 3: two regions of lymph node involvement→ one above and one below the diaphragm
200
What is the most important recommendation in management of someone older than 60yo with new iron deficiency anemia?
Need to get a colonoscopy!!
New iron deficiency could mean a new internal bleed
specifically males >60yo common sources of bleeding is colon from polyps, cancer, hemorrhoids, etc.
200

Iron deficiency anemia
hypochromic- central pallor should only be 1/3 of RBC
microcytic- RBC normally about the size of a lymphocyte nucleus
RDW- lots of variation in sizes of RBC
200
What disease is suggested by an increased hemoglobin concentration, leukocytosis, and thrombocytosis?
Polycythemia vera
increases in all three cell lines- RBC, platelets, BM/ WBC
Most commonly from JAK2 mutation
Treatment is phlebotomy, hydroxyurea, aspirin
Risk of hyperviscous blood--> clots
300
A 26 year-old female required 12 units of packed red blood cells during a trauma resuscitation and surgical repair of liver and splenic lacerations. The patient is now 6 hours postoperative and has blood oozing from the suture line and IV sites. There is bloody urine in the Foley bag. Laboratory evaluation demonstrates a platelet count of 10,000/microliter, prolonged prothrombin level, and the presence of fibrin split products.What is the most likely diagnosis?
Disseminated intravascular coagulation (DIC)
Actually a widespread hypercoagulable state but as all your coag factors and platelets are used up then you have widespread hemorrhages
Bleeding from everywhere!! Foley, sutures, IV sites, may be vomiting blood
emergent platelet and FFP transfusions
300
Translocation between chromosome 9 and 22 and positive BCR-ABL oncogene indicates what? What is the translocation called?
Philadelphia chromosome t(9;22)
Indicates chronic myeloid leukemia when found in bone marrow.
Most adults will be asymptomatic until "blast crisis" (>20% blasts in BM) --> presents like AML
CML treatment= Gleevec
300
What additional test can help differentiate folate and B12 deficiency?
*Only needed if specific serum folate and B12 levels are borderline
Methylmalonic acid (MMA) and homocysteine
Homocysteine is elevated in both b12 and folate
MMA is elevated in B12 deficiency
300
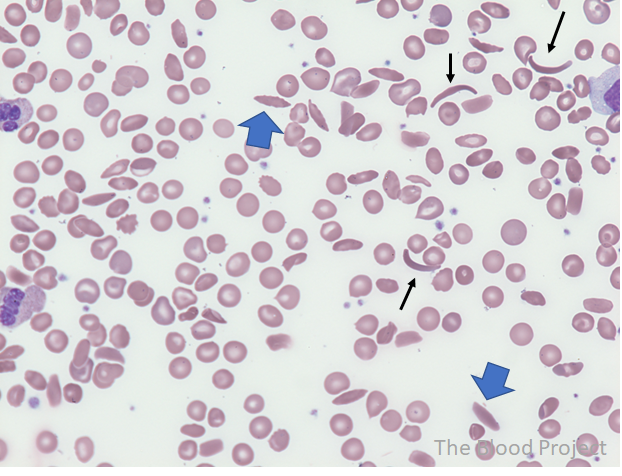
Sickle cell!
300
A 1 year old presents with his mother for the first time since moving to the US from Greece. Right away you notice the patient has frontal bossing, chipmunk cheeks. What test would confirm the expected diagnosis?
Hemoglobin electrophoresis to confirm beta thalassemia
Will show 95% HbF, HbA2 10%, NO HbA
CBC will show severe microcytic anemia
- Mediterranean descent
400
a 10 week old infant presents to the ER after a seizure. The baby is lethargic and not responding to appropriate verbal or physical stimuli. The mother received all appropriate prenatal care and has been exclusively breastfeeding the patient. The baby was born at home and has not yet seen a medical provider for care. Physical examination shows shallow respirations and a petechial rash on the oral mucosa. Laboratory studies, platelet count and fibrinogen level are within normal limits, and international normalized ratio is 4. CT scan of the head shows intracranial hemorrhage. What best explains the patient's findings? And what did the patient likely not receive after birth?
Vitamin K deficiency
Vitamin K injection at birth likely not given
Most commonly presents in breastfed infants 2-12 weeks old who did not receive vitamin K injection. Presents with intracranial bleeding and has a high mortality rate.
400
A 4 year old presents with fever, bone pain, abdominal pain, easy bruising, and a recurrent URI. CBC shows neutropenia, decreased hemoglobin, decreased platelets. Peripheral smear shows some blasts cells. What is the most likely diagnosis? What is the next steps to confirm the diagnosis?
Child should make you think Acute lymphoblastic leukemia
*ALL children get ALL:/
need BM biopsy which will show >20% lymphoblasts to confirm
Good prognosis when treated with chemo. The younger the dx the better prognosis with ALL
400
a 62-year-old male with a history of chronic kidney disease complains of weight loss, fatigue, and weakness. Iron studies reveal decreased serum iron, increased ferritin, and decreased TIBC. Peripheral blood smear shows normochromic RBCs. What is the most likely diagnosis?
Anemia of chronic disease- can coexist with iron deficiency
Common causes include:
#1 CKD then other connective tissue disorders including RA, Lupus, HIV, cirrhosis
400

Folic acid deficiency anemia
macrocytic- large oval shaped RBCs
*hypersegmented neutrophils**
Note variety in RBC size = high RDW!
400
What is the classic triad observed in patients with hemochromatosis?
Cirrhosis, diabetes mellitus, bronzed hyperpigmented skin
Increased iron deposition in liver, pancreas and in skin
Now most commonly found incidentally
Treat with phlebotomy
500
A 32-year-old man with a history of easy bruising and joint swelling is being prepped for an appendectomy. During the physical examination, the patient states that he had surgery to correct a heart defect when he was 4, and during the procedure, he was bleeding uncontrollably. Since then he has been diagnosed with a bleeding disorder and must be treated prophylactically prior to any surgical procedure. He adds that his maternal grandfather and 2 of his grandfather's brothers also had the same disorder. What is the best primary perioperative treatment to prevent uncontrollable bleeding?
Hemophilia A→ recombinant factor VIII is the best primary periop treatment
For mild hemophilia A you can use desmopressin which stimulates release of vWF and FVIII but not enough that would be needed for a surgery or severe disease
hemophilia A=8 Factor VIII
- hemophilia B. b= upside down 9
500
55yo presents with fatigue, easy bruising, gingival hyperplasia and bleeding gums. CBC shows anemia, neutropenia, and thrombocytopenia. Smear shows peripheral blasts. Bone marrow biopsy shows Auer rods. What is the most likely diagnosis?
Auer rods = Acute myelogenous leukemia

unique AML sxs are bleeding gums.
500
What anemia results in all three cell lines being decreased? RBC, WBC, and platelets?
Aplastic anemia- hypocellular bone marrow
Mostly idiopathic but look for drugs that could cause-->Phenytoin, sulfa, ACE, methimazole, chemo
No reticulocytosis– aka no new RBCs
500

Normal smear → RBC are around the same size and shape, central pallor is around ⅓ of RBC width, normal neutrophils and platelets present.
500
A 29 year-old patient with idiopathic thrombocytopenia purpura (ITP) is treated with prednisone therapy. Despite therapy, platelet counts remain consistently below 20,000/microliter over the course of 6 weeks. What is the next best step? What is the risk with platelets this low?
<20K platelets risks spontaneous bleeding.
Requires more definitive treatment with splenectomy because of the severity
If steroids aren't helping but levels are not as severe could try IVIG first