Red Blood Cell Disorders
Platelet Disorders
Hematologic Malignancies
Coagulation and Transfusion
Oncology Emergencies
100
44 year old woman presents with fatigue. She eats a balanced diet and takes no medications. She has regular menstrual periods. No melena stools
HR 90, BP 135/76 no hepatosplenomegaly or Lower ext edema.WBC 8.5k, MCV 70, Hgb 7, plt 550K, Iron 25, Ferritin 8, TIBC 500
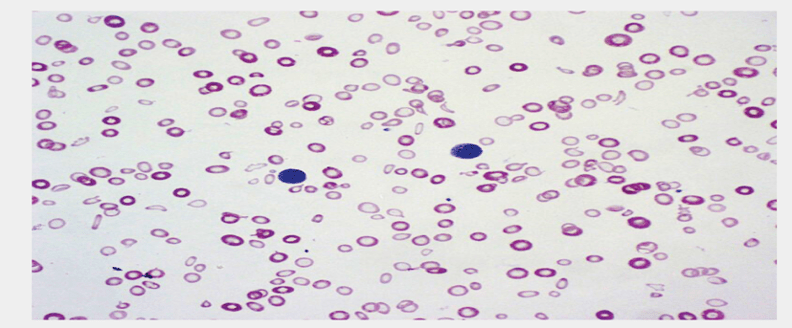
Most likely diagnosis?
Iron deficiency anemia
- hypochromic, microcytic red cells on peripheral blood smear.
- low iron level coupled with high iron-binding capacity for a low iron saturation, low ferritin level, low mean corpuscular volume
- high platelet count.
100
A 28-year-old woman at 20 weeks gestation is found to have a platelet count of 110K. She has no bleeding symptoms and no prior history of thrombocytopenia.
What is the most likely diagnosis?
Gestational thrombocytopenia
- Mild thrombocytopenia (>100K), asymptomatic
Resolves postpartum
100
A 35-year-old woman has leukocytosis and is found to have a t(9;22) translocation.
What fusion protein is produced, and what is the most appropriate therapy?
BCR-ABL fusion protein → TKI (Imatinib)
Diagnosis: CML
- Philadelphia chromosome
- Low LAP score distinguishes from leukemoid reaction
100
Primary goal of PRBC transfusion?
Increase oxygen-carrying capacity
1 unit PRBC → ↑ Hgb by ~1 g/dL
Not for volume expansion
Platelets and FFP have different indications
100
A patient receiving chemotherapy develops hyperkalemia, hyperphosphatemia, hypocalcemia, and acute kidney injury 24 hours after treatment.
What is the most likely diagnosis?
Tumor lysis syndrome
- Rapid tumor breakdown releases intracellular contents.
- Can cause fatal arrhythmias.
- Treat with aggressive IV fluids
200
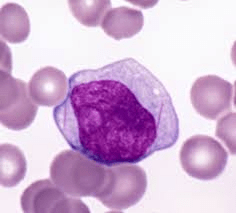
A 41 year old patient with a history of Roux-en-Y gastric bypass complains of weakness and impaired vibratory/proprioceptive sense
Provide the most likely condition that could produce the smear shown: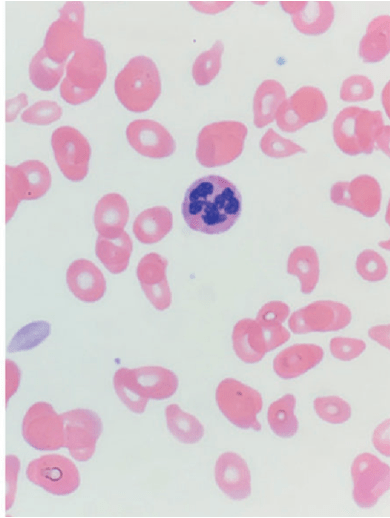
Vitamin B12 deficiency with SCID
- Develops because of inadequate binding by intrinsic factor after gastric bypass.
- Iron deficiency develops as food bypasses iron absorption sites in the duodenum.
200
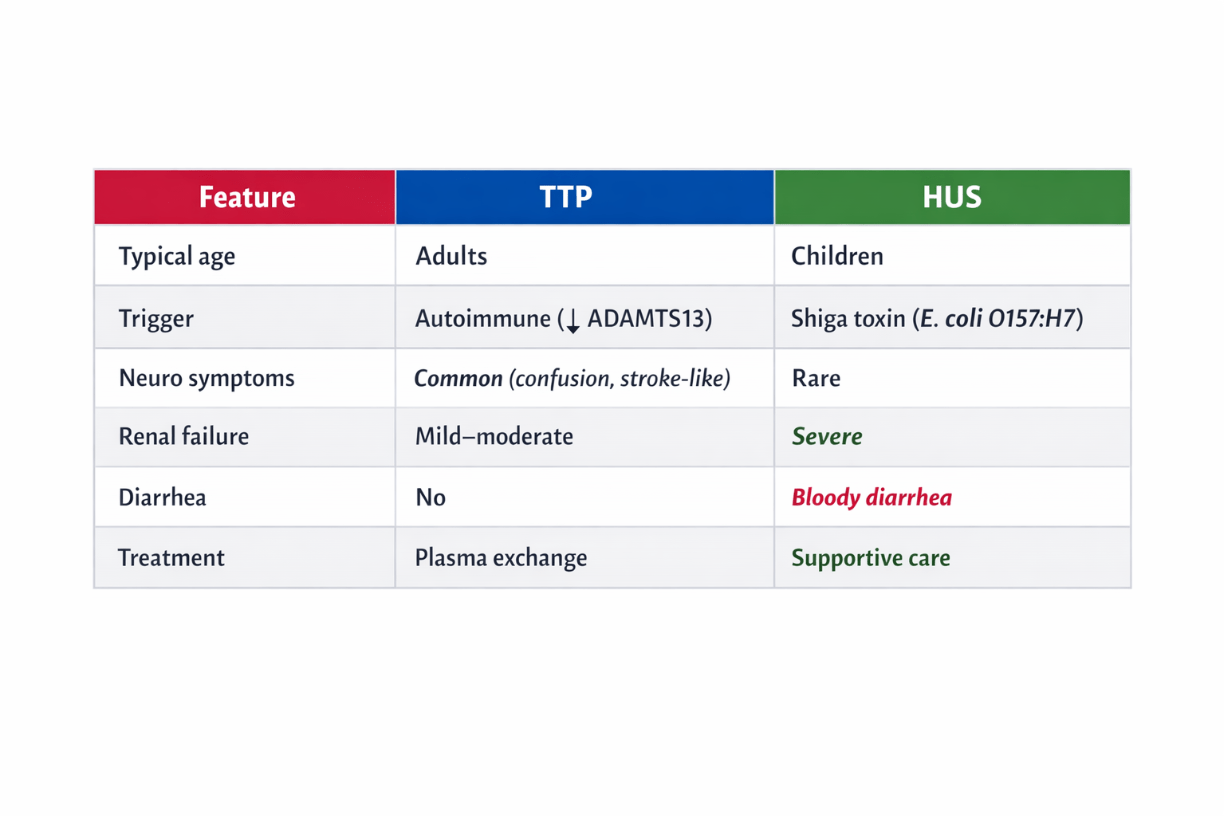
A young woman presents with abdominal pain and bloody diarrhea.
Labs show:
Hgb 10.5
Platelets 123K
Creatinine 1.9
LDH elevated
What is the most likely diagnosis?
Hemolytic Uremic Syndrome
AKI + hemolysis + thrombocytopenia
Supportive care (avoid antibiotics in E. coli O157:H7)
200
A 11-year old boy presents with pain and a maxillary/mandibular mass of the jaw. Biopsy reveals
"starry-sky appearance". Diagnosis?
Burkitt lymphoma (t(8;14))
- MYC translocation
- Very high Ki-67
- Associated with EBV
200
Mechanism of tPA?
Converts plasminogen → plasmin
Plasmin degrades fibrin
Used in STEMI and stroke
Risk of intracranial hemorrhage
Medications that inactivate factor Xa - Apixaban and Rivaroxaban
200
A patient with newly diagnosed leukemia develops elevated uric acid after starting chemotherapy.
What medication should be given to prevent renal failure?
Rasburicase
- Converts uric acid → allantoin (more soluble).
- Prevents uric acid nephropathy.
- Contraindicated in G6PD deficiency.
Why not allopurinol?
300
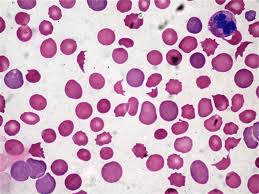
8 yr old male complained of abdominal pain and dark urine. He was recently treated with Bactrim for a UTI. His peripheral smear is as follows:
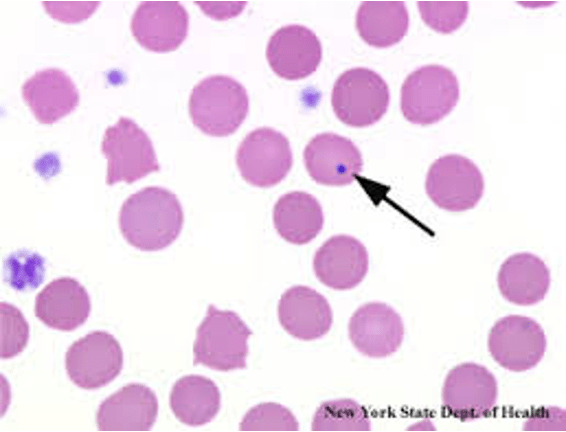
What triggers should he avoid?
Sulfa drugs, isoniazid, dapsone, quinines, nitrofurantoin, ibuprofen, aspirin and fava beans.
G6PD deficiency → ↓ NADPH → ↓ glutathione
→ RBCs cannot handle oxidative stress
→ Heinz bodies → splenic removal → bite cells → hemolysis
- Treatment is to avoid triggers.
300
A woman with well-controlled HIV presents with gingival bleeding and petechiae.
Labs:
Platelets 12K
Hgb normal
WBC normal
What is the most likely diagnosis AND first-line treatment?
Immune thrombocytopenia (ITP)
- HIV triggers autoantibodies against platelet glycoproteins (often GpIIb/IIIa)
- ART alone often improves platelet count.
- If persistent/severe thrombocytopenia
Glucocorticoids or IVIG
300
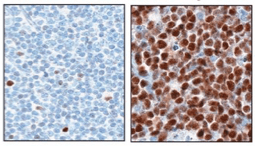
A patient with B symptoms and diffuse lymphadenopathy has CD20-positive large B cells.
What is the most likely diagnosis?
Diffuse large B-cell lymphoma
- Most common aggressive NHL
- Elevated LDH common
- Treat with R-CHOP
300
A hospitalized patient with active inflammatory bowel disease is awaiting repeat colonoscopy. What is the most appropriate medication to administer?
Give DVT prophylaxis
IBD causes a hypercoagulable state
Risk highest during flare and hospitalization
Give pharmacologic DVT prophylaxis unless active bleeding. LMWH preferred
300
A cancer patient presents with acute back pain, progressive lower extremity weakness, and urinary retention.
What is the most appropriate immediate next step?
Emergent MRI of the spine
- Suspect malignant epidural spinal cord compression.
- Start high-dose steroids immediately.
- Neurosurgery and radiation oncology consult urgently.
400
A 32 year old man is evaluated for shortness of breath for 2 weeks. He has a history of SLE and his only medication is hydroxychloroquine. He is tachycardic on exam and his pulse ox is 99% on RA.
Hgb 10, WBC 4.2k, Platelet 125k, Reticulocyte count 15%, LDH 475
What is the most appropriate diagnostic test in this case?
Direct antiglobulin test (Direct Coombs test)
- SLE: Warm autoimmune hemolytic anemia (AIHA)
- DAT detects:
IgG and/or C3 bound to RBCs
Confirms autoimmune hemolysis
- Suspect hemolytic anemia if you see anemia, elevated reticulocytes, elevated LDH, low haptogobin, indirect hyperbilirubinemia
400
A patient presents with fever, confusion, anemia, thrombocytopenia, and schistocytes on smear.
What is the immediate treatment?
Plasma Exchange
Diagnosis: TTP (Thrombotic Thrombocytopenic Purpura)
Schistocytes + neurologic symptoms
Immediate plasma exchange — do NOT wait for ADAMTS13
400
A 67-year-old asymptomatic man is found to have a monoclonal protein level of 2.2 g/dL on serum protein electrophoresis. He has normal calcium, creatinine, and hemoglobin levels, and no bone pain.
What is the most likely diagnosis?
MGUS
- Does not fit CRAB criteria, No lytic bone lesions, No Rouleaux on peripheral smear, and no Bence Jones proteinuria; these are seen in Multiple Myeloma
- M protein <3 g/dL, No end-organ damage, Monitor annually
400
A 75-year-old man with atrial fibrillation on warfarin presents with a large intracranial hemorrhage after a fall.
Labs show:
INR 3.8
Platelets 190,000
Hemoglobin 13 g/dL
He is hemodynamically stable.
What is the most appropriate immediate treatment to reverse his coagulopathy?
Prothrombin complex concentrate (PCC) + IV vitamin K
- Life-threatening bleeding on warfarin requires rapid reversal of clotting factors.
- PCC replaces factors II, VII, IX, and X faster and more effectively than FFP.
- Vitamin K must also be given for sustained reversal.
400
A patient with metastatic cancer develops sudden severe headache and focal neurologic deficits. CT reveals hemorrhagic brain metastases.
Which three primary tumors are most commonly associated with hemorrhagic metastases?
Renal cell carcinoma, melanoma, and thyroid cancer
- Highly vascular tumors.
- Increased risk of intracranial bleeding.
- Sudden neuro decline in cancer patient → consider hemorrhagic mets
500
A 45 year old woman presents with episodic dark urine, fatigue, and shortness of breath. She undergoes anemia work up which reveals CD55 and CD59 negative RBCs. She is begun on medical treatment with a biologic agent. What is a concerning complication of the therapy used in her case?
Neisseria meningitidis infection (meningococcal sepsis)
Diagnosis:
Paroxysmal Nocturnal Hemoglobinuria (PNH)
Loss of GPI-anchored proteins → complement-mediated hemolysis.
Eculizumab
→ Monoclonal antibody against C5
→ Blocks terminal complement activation (C5b-9)
500
A 64-year-old man is hospitalized for pulmonary embolism and started on intravenous heparin. On hospital day 6, his platelet count drops from 260,000 to 110,000. He has no bleeding but develops new swelling and pain in his right leg. Doppler ultrasound confirms a new DVT.
What is the most likely diagnosis and the most appropriate next step in management?
Heparin-induced thrombocytopenia (HIT) → stop all heparin and start argatroban (or another non-heparin anticoagulant).
-
Platelet drop >50% occurring 5–10 days after heparin exposure strongly suggests HIT.
- HIT causes thrombosis (arterial or venous), not bleeding — new clot with falling platelets is classic.
- Immediately stop all heparin and start a direct thrombin inhibitor (argatroban or bivalirudin); do NOT give platelets.
500
A 29-year-old man presents with fatigue, spontaneous bruising, and gingival bleeding. Labs show anemia, thrombocytopenia, prolonged PT/PTT, low fibrinogen, and blasts on smear. Cytogenetics reveals t(15;17).
What is the most appropriate immediate treatment?
All-trans retinoic acid (ATRA)
- Acute promyelocytic leukemia
- Associated with DIC
- Start ATRA immediately — don’t wait
500
A 62-year-old woman develops severe postoperative bleeding 1 week after knee replacement. She has no prior bleeding history.
Labs:
Platelets normal
PT normal
aPTT prolonged
Mixing study does NOT correct
What is the most likely diagnosis and the most appropriate treatment?
Acquired factor VIII inhibitor
- Normal platelets + normal PT + prolonged aPTT
→ This isolates the problem to the intrinsic pathway (Factor VIII, IX, XI).
- Mixing study does NOT correct
→ If it were a simple factor deficiency (like hemophilia), adding normal plasma would correct it.
→ Failure to correct means there is an inhibitor — most commonly an autoantibody against Factor VIII.
- Rx: Recombinant factor VIIa (Bypass therapy)
500
A chemotherapy patient presents with fever of 100.4°F and an absolute neutrophil count (ANC) of 35. He appears stable but has no obvious source of infection.
What is the most important immediate management step?
Start empiric broad-spectrum anti-pseudomonal antibiotics immediately
- Neutropenic fever is a medical emergency.
- Do NOT wait for culture results.
- Must cover Pseudomonas (e.g., cefepime, piperacillin-tazobactam).