Angy Heart
Neuromuscular Madness
Coagulative Catastrophies
Diarrheal Disasters
Pop Culture
100
According to the ACC 2025 concise clinical guideline, what is the preferred treatment option for patients with pericarditis that fail to respond to NSAIDs + colchicine with inflammatory pericarditis?
Anti-IL-1 - rilonacept, anakira or goflikicept
In addition to continuing NSAID + colchicine

100
Name one FDA approved treatment for ALS
Riluzole - 3 month increased survival (1997)
Edaravone - decreased functional decline (2017)
Tofersen - for rare SOD1 mutation ALS (2023) - increases survival, functional decline (may even stabilize functional decline)
100
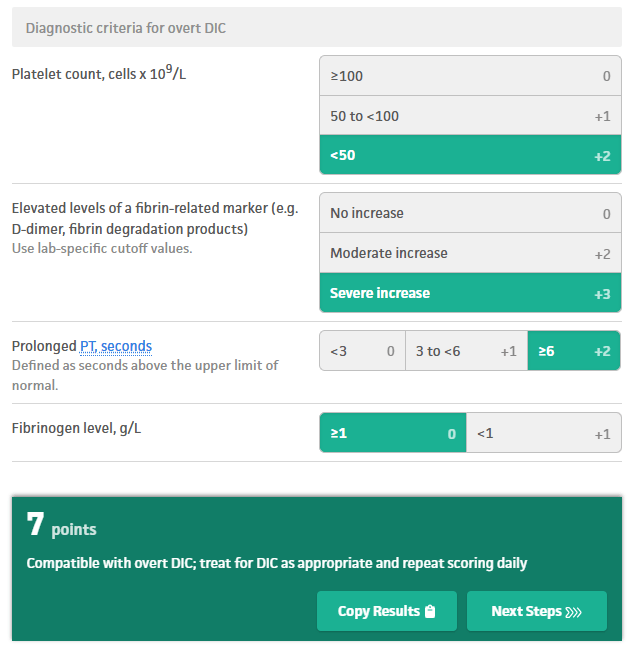
Classic lab finding in DIC (high/low):
___ plt
___ aPTT
___ PT
___ INR
___ fibrinogen
Low plt
High aPTT
High PT
High INR
Low fibrinogen
ISTH Criteria DIC score:
100
How do we define acute, persistent and chronic diarrhea?
Acute < 2 weeks
Persistent 2-4 weeks
Chronic > 4 weeks
100
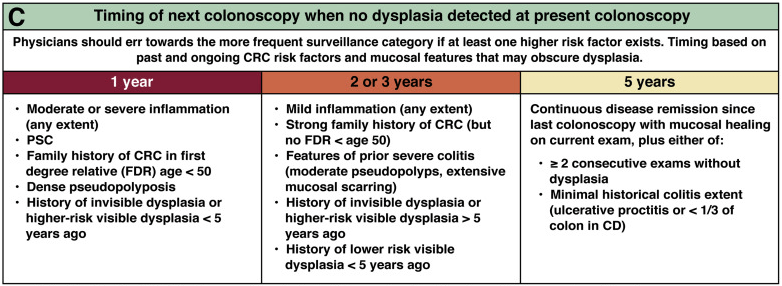
This bloke, who is no longer featured on SNL, has a chronic inflammatory disease in his gut. If he were to have a normal routine dysplasia screening colonoscopy 8-10 years after diagnosis showing mild inflammation, when should he next have a follow up colonoscopy for dysplasia screening?

Classically we are taught q2 years for everyone.
Recent guidelines risk-stratify based on important considerations include clinical/endoscopic remission, family risk, PSC
200
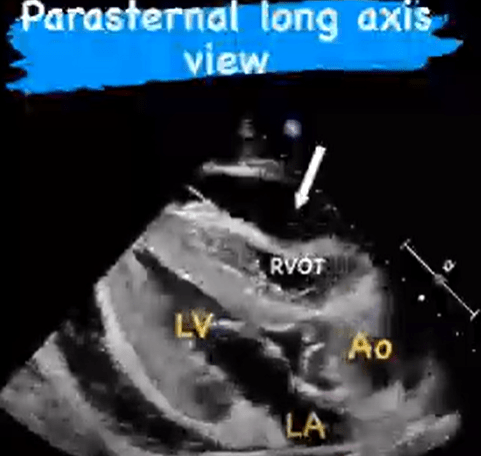
What is the most specific and concerning finding on POCUS for cardiac tamponade?
Diastolic right ventricular free wall collapse.
200
Assuming good patient technique, A NIF value worse than ___ is concerning for impending respiratory failure
-30
Oftentimes limited by poor technique, so always ask RT if they think seal/effort was good.
200
How does the American Society of Hematology recommend that patients with stable CVD on aspirin started on therapeutic anticoagulation for a new DVT/PE be managed?
Hold asp for duration of anticoagulation.
For patients with DVT/PE with stable cardiovascular disease, the ASH guidelines suggest suspending aspirin therapy when initiating anticoagulation. The combination of anticoagulation plus aspirin increases the risk of bleeding without clear evidence of benefit for patients with stable cardiovascular disease.
200
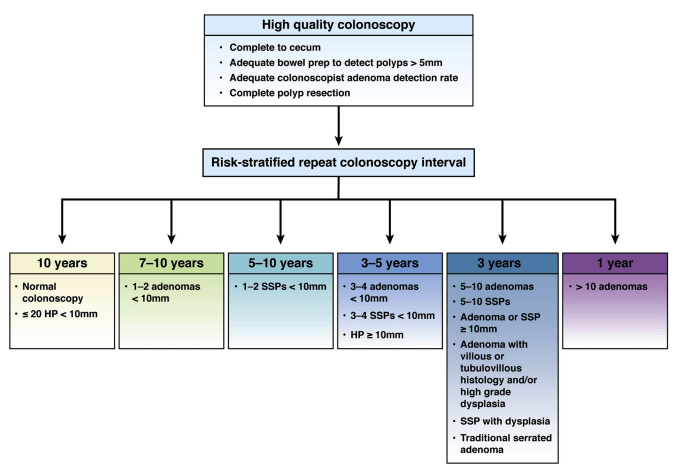
A 55 y/o female undergoes a screening colonoscopy, which shows three polyps (3mm, 5mm, and 6mm in size); all three polyps were excised and pathology showed them to be hyperplastic. When should this patient next undergo colonoscopy?
10 years: hyperplastic polyps are non-neoplastic and do not warrant earlier follow-up if < 10mm. If they are > 10mm, they should be treated similarly to sessile serrated polyps and patients may need earlier follow-up.
200
This artist, with hit song "Just Give Me a Reason", struggles with this common chronic, debilitating respiratory disease for which pulmonary guidelines have recommended changing first line treatment from this inhaled medication PRN to ______. 
P!nk
Asthma
ICS-LABA (preferred) or low dose ICS daily + PRN SABA
SABA only treatment is a/w increased exacerbations, lower lung function and asthma-related death
300
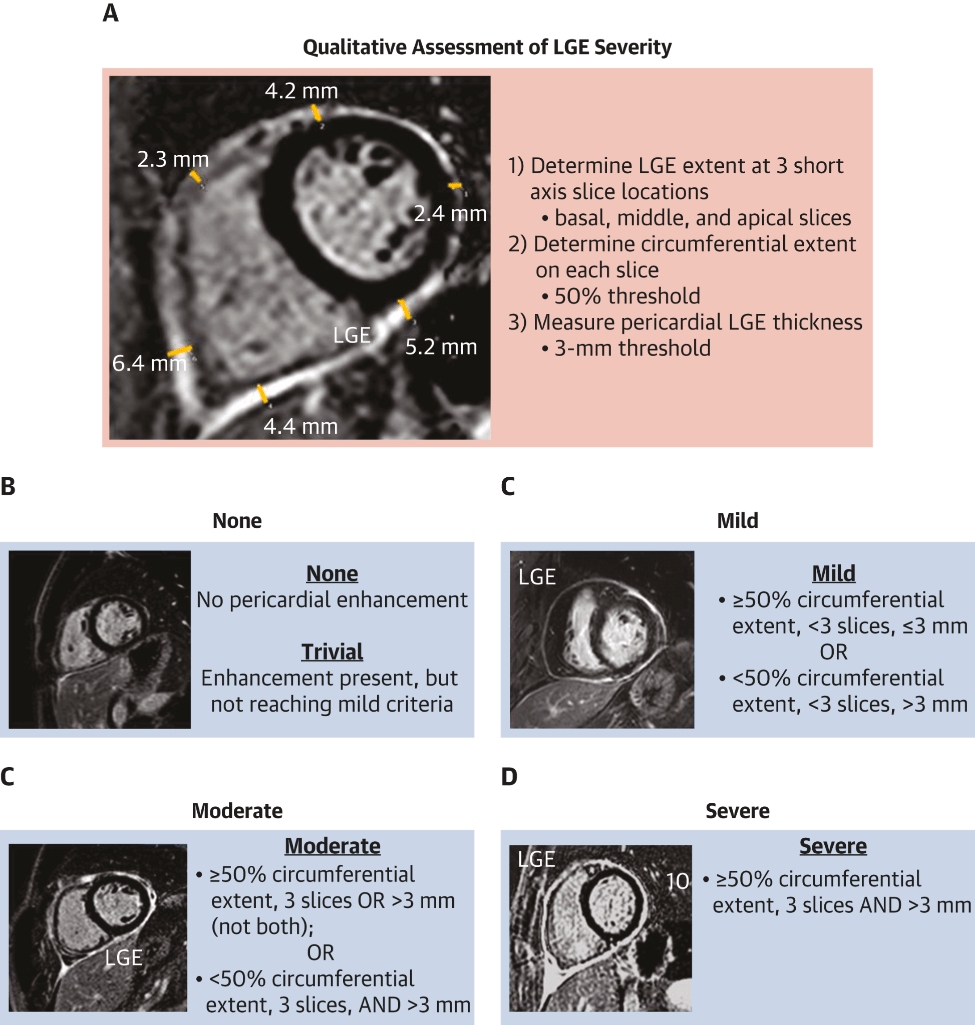
What finding on cardiac MR is primarily used to establish a diagnosis of pericarditis and grade it's severity?
Late gadolinium enhancement/edema - on phase-sensitivity inversion recovery sequence (ideally fat-suppressed), indicating neovascularization or inflammation
300
A 44F patient reports diplopia, ptosis, and dysphagia that occurs towards the end of the day/before bed. Denies waking up with symptoms. She undergoes evaluation and found to have positive ACh-R antibodies. In addition to electrodiagnostic confirmation, what additional evaluation should they undergo (2)?
Myasthenia Gravis
Chest CT → Thymoma
TFTs → Autoimmune thyroid disease
300
What laboratory testing can help differentiate DIC from liver-induced coagulopathy, and what result might be expected?
Factor VIII levels, which are produced by endothelial cells and independent of liver function.
DIC: consumption of all factors - usually low
Liver-induced coagulopathy: endothelial cells increase production to offset coagulopathy - usually high
300
A 25-year-old woman is evaluated for frequent watery, non-bloody diarrhea, arthralgia, and headaches. Diarrhea, arthralgia, and headaches resolved after the patient started a gluten-free diet 1 year ago. Symptoms occasionally return if she accidentally consumes gluten.
Vital signs and other physical examination findings are normal. Laboratory studies show a normal tissue transglutaminase IgA and total IgA levels. Results of testing for haplotypes HLA-DQ2 and HLA-DQ8 are positive for HLA-DQ2.
What do?
Test for c diff
Repeat HLA test after resumption of gluten containing diet
Repeat tissue transglutaminase IgA measurement after resumption of gluten-containing diet
Upper endoscopy and biopsy
Tissue transglutaminase IgA test after resumption of a gluten-containing diet.
A positive result on a serologic test for celiac disease requires upper endoscopy with biopsies from the duodenum to confirm the disease. If biopsy results suggesting celiac disease are obtained before serologic testing, confirmatory serologic testing should be performed. Findings on upper endoscopy and biopsy may be normal in a patient with celiac disease who has adhered to a gluten-free diet for the past year. Therefore, the most appropriate management is resumption of a gluten-containing diet and follow-up serologic testing.
HLA-DQ2/DQ8 present in 40% of gen population, but present in 98-99% of those w/ celiac
300
This celebrity, who has a lifelong inflammatory skin disorder often associated with arthritis, should have a risk-benefit discussion with her rheumatologist or dermatologist about systemic therapies in these situations (4).
Kim Kardashian
Psoriasis
1 Severe psoriasis = >10% BSA
2 Concomitant psoriatic
3 Failure of topical meds
4 Scalp or groin involvement
Others can include rapid progression, QOL impact
400
Which patients should be hospitalized for acute pericarditis per new ACC statement (5)?
High fevers (>38°C)
Subacute course
Presence of large pericardial effusion with echocardiography features of tamponade physiology
Failure to respond to outpt nonsteroidal anti-inflammatory drugs (NSAIDs)
Concomitant myocarditis
Can consider immunosuppression, oral anticoagulation, and trauma
400
Name 3 meds known to worsen myasthenia
antibiotics including fluroquinolones + macrolides + aminoglycosides
AEDs; antipsychotics, BBs, CCBs, Mg, iodinated contrast rarely
400
How is catastrophic APLS (3 or more organ thrombosis in less than 1 week) treated?
Therapeutic anticoagulation (typically IV heparin), IV methypred 0.25-1g, and IVIG or therapeutic plasma exchange or both if available
For refractory cases, rituximab or eculizumab can be considered
50% mortality
400
A 40yo female with a history of ileo-colonic Crohn’s disease presents with gas and feculent vaginal discharge for the past 2 weeks. MRI reveals a fistulous tract from the rectum through the vaginal wall with surrounding edema. What is the next appropriate step in management?
TNF-a inhibitors first line for fistulizing disease
Infliximab (Remicade), adalimumab (Humira) as alt first line/second line. May have adjunctive immunomodulator/antibiotic/surgical procedure.
Certolizumab less evidence for fistula remission
Ustekinumab (Stelara, anti IL12-23) + Vedolizumab (Entyvio, anti-a4B7) w/ some evidence for second line
400
This iconoclastic singer struggles from a chronic debilitating MSK condition characterized by point tenderness, for which FDA-approved pharmacotherapy includes ______(up to 3).

Lady Gaga
Fibromyalgia
Duloxetine, milnacipran (good w/ comorbid depression), and pregabalin (pain, anxiolytic)
Amytriptiline (sleep, fatigue) and Flexeril not technically FDA-approved, but can be good for alt dx.
500
How can you establish a definite diagnosis of myocarditis? How about a probable diagnosis?
Definite - Cardiac MRI or endomyocardial biopsy
Probable -
elevated trop
LV +/- RV dysfunction (abnmormal strain, wall motion or reduced EF)
ST-T changes - nonspecific, but still count
500
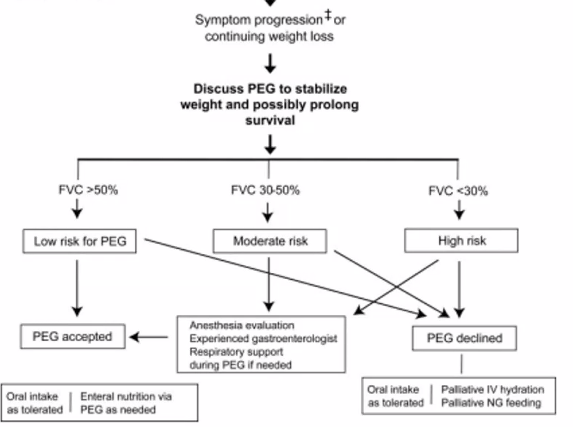
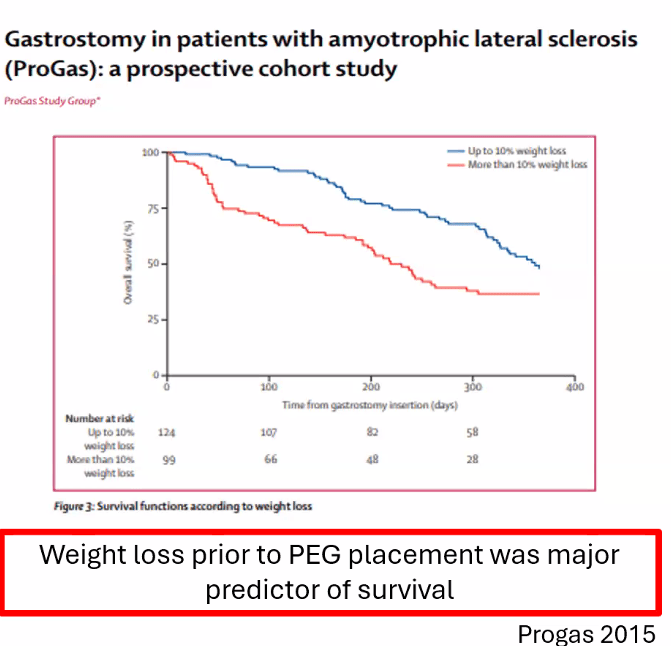
Which patients with ALS are likely to have a survival benefit of gastrostomy tube placement?
FVC> 50%, ideally before significant weight loss (>10% of BW)
FVC 30-50% less likely to see survival benefit, but may have symptom improvement + weight gain
500
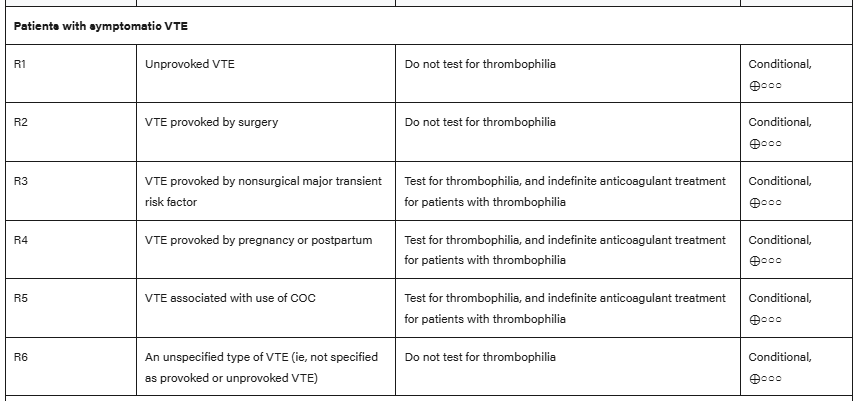
Per the American Hematologic Society Guidelines, which patient populations should not undergo testing for thrombophilia conditions after a new diagnosis of venous thromboembolism at a usual site (2)?
Unprovoked DVT - warrants indefinite anticoagulation, regardless of etiology. Exception is high suspicion of APLS, because it can change management
VTE provoked by surgery or other clear predisposing medical syndrome.
Testing indicated for: VTE provoked by nonsurgical major transient risk factor, cerebral/splanchnic VTE, age < 45, recurrent/multiple thrombosis, arterial thrombosis (needs APLS testing).
500
What are the Rome IV diagnostic criteria for IBS (5).
 Should also have normal CRP, IgA level + IgA TtG. Normal physical exam, basic labs and no alarm features.
Should also have normal CRP, IgA level + IgA TtG. Normal physical exam, basic labs and no alarm features.
500
What should be first line treatment for patient presenting with community aquired pneumonia, + risk factors for MRSA, and this chest CT?

Amp-Sulbactam, Macrolide (usually azithro) + Vanc/linezolid
Chest tube for empyema, abscess may also require drainage
Green arrows - abscess w/ thick walls and air filled cavity - inside lung parenchyma
Yellow arrows - Empyema w/ thin walls and fluid filled, in the pleural space seperating parietal and visceral