True or False
CLABSI
CAUTI
Myth vs. Fact
Infection Prevention: Practice
Infection Prevention: Regulatory
100
Femoral lines have a lower risk of infection than a PICC line or PORT
FALSE
There is a higher risk of infection with femoral lines. Every effort should be made to avoid femoral access.
100
What should be done every time you access a central line lumen or port (Y-site).
Scrub the hub!

100
After an IUC is removed, intermittent straight catheterization (ISC) should only be performed for 24 hours. True or False
False. ISC can be performed as often as necessary and tolerated by the patient. Some patients may require ISC for more than 24 hours.
ISC is a safe and effective treatment to decompress the bladder and restore bladder function.
RN maintains autonomy to follow the pathway and collaborate with the interdisciplinary team to provide updates and develop individualized interventions as needed.
100
The risk of developing a Urinary Tract Infection (UTI) is greater with intermittent catheterization than with an indwelling urinary catheter
MYTH
Evidence from several studies suggest a benefit of using intermittent catheterization (IC) over indwelling catheters in selected populations:
-urinary retention and bladder distention can be avoided by performing IC at regular intervals until voiding returns
-for post-op patients, increased risk of urinary retention can be managed with IC to restore normal bladder tone
-among neurogenic bladder patients, nearly all published studies show a decreased risk of CAUTI with IC
The length of time an IUC is in place is the most important contributing factor to developing a UTI
-daily risk of bacteriuria in catheterized patients: 3-7%
-7% risk of UTI 24 hours after insertion of an IUC
-8% risk daily in first 7 days after IUC placed
100
What should be present on each access port (Y-site) and lumen to help prevent infection?
Disinfection cap or SwabSleeve SwabCap
100
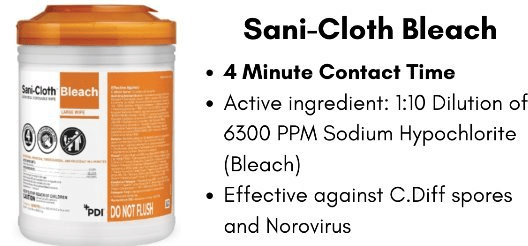
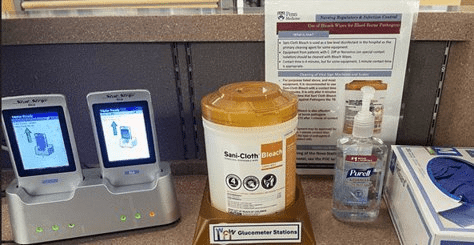
What are the contact times for the Super Sani-Cloth and Sani-Cloth Bleach wipes?
Two (2) minutes for the wipes in the purple top container and four (4) minutes for wipes in the orange top container.

200
All central lines should be removed as soon as they are no longer necessary.
True!
Document Line Necessity (Line Review) Daily in the LDA assessment! If central line is no longer necessary, talk to the team about plans for removal!
200
Your NTP pt is due to culture and has a fever of 100.5. This should be your recommendations to the provider.
RN notifies provider via phone of first neutropenic febrile event.
RN releases conditional orders (blood cultures, lactic acid, UA/UC, chest X-ray)
Provider orders antibiotics STAT.
RN collects specimens and ensures antibiotics are administered within 1 hour of fever
200
True or False: If IUC removal is nurse-driven, a nurse may autonomously remove the IUC without a provider order
TRUE
Provider Order Required for all IUCs
-At initiation, the provider enters the indication for IUC placement AND a removal plan
-The removal plan is ordered as either Provider Driven or RN driven
-Patient eligibility for the post-IUC removal PennPathway is included in the initial order
Nurse Driven Removal Plan
-The RN assesses the need for IUC continuation or removal
-When the IUC is no longer indicated based on the patient's condition, the RN may autonomously remove it
-RN does not need to obtain an IUC removal order
-If patient eligible, RN follows Post-IUC Removal Management PennPathway
200
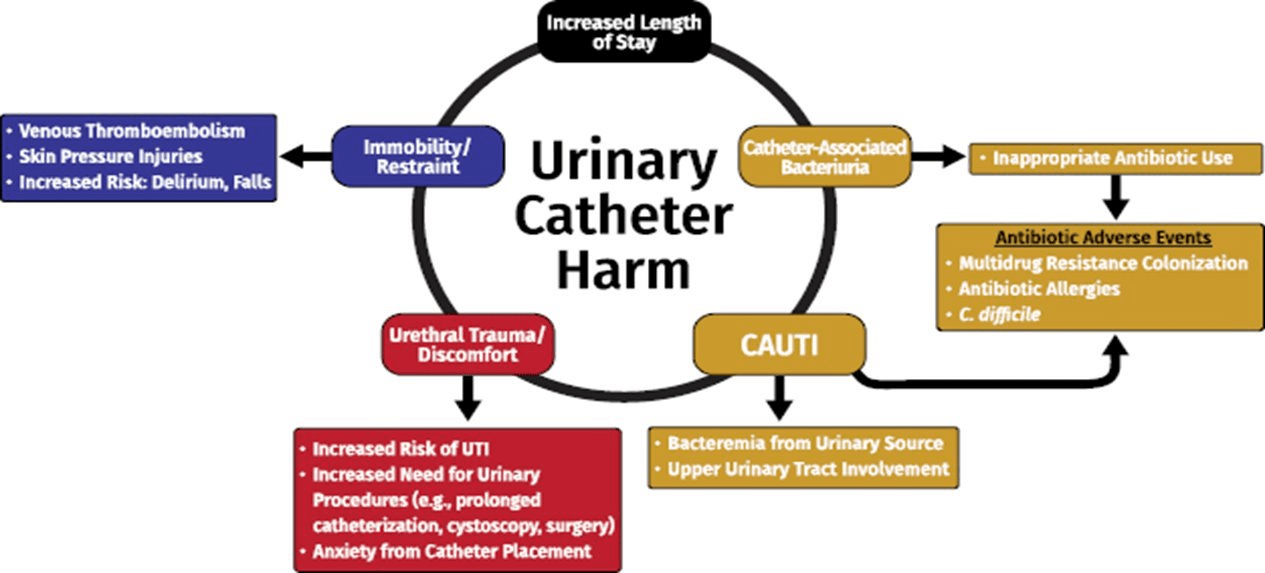
The only harm associated with an indwelling urinary catheter is a CAUTI
MYTH
Costs of a UTI
-infection increases the length of stay by 3-5 days
-treating hospital-acquired CAUTI costs $4,694-$29,743
Treatment With Antibiotics Increases the Risk of:
-development of C. difficile
-colonization with resistant organisms
Non-Infectious Risks Associated with IUC
-57% of patients developed non-infectious complications after IUC placement
-non-infectious risks include: sense of urgency/bladder spasms (24%), leaking urine (20%), pain with urination (17%), skin issues (during placement or securement) (6%)
200
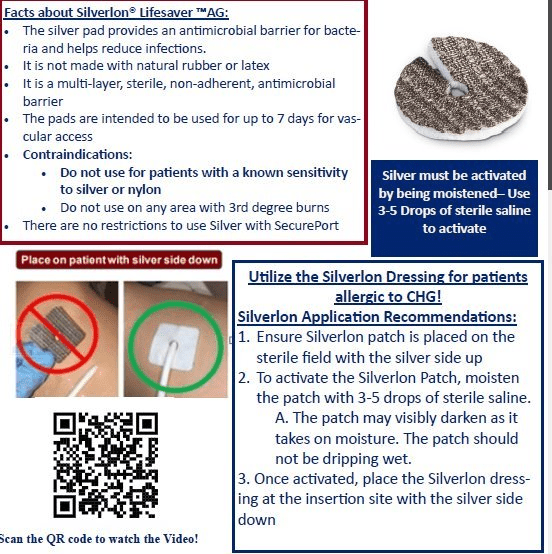
What type of dressing do you put on a CL site for a patient allergic to CHG?
Silverlon patch and IV3000
200
The directions for how to clean an instrument. (Hint: a frequent question from regulatory surveyors)
What is an IFU or Instruction for Use?
IFUs can be found in the UPHS Intranet home page under One Source

300
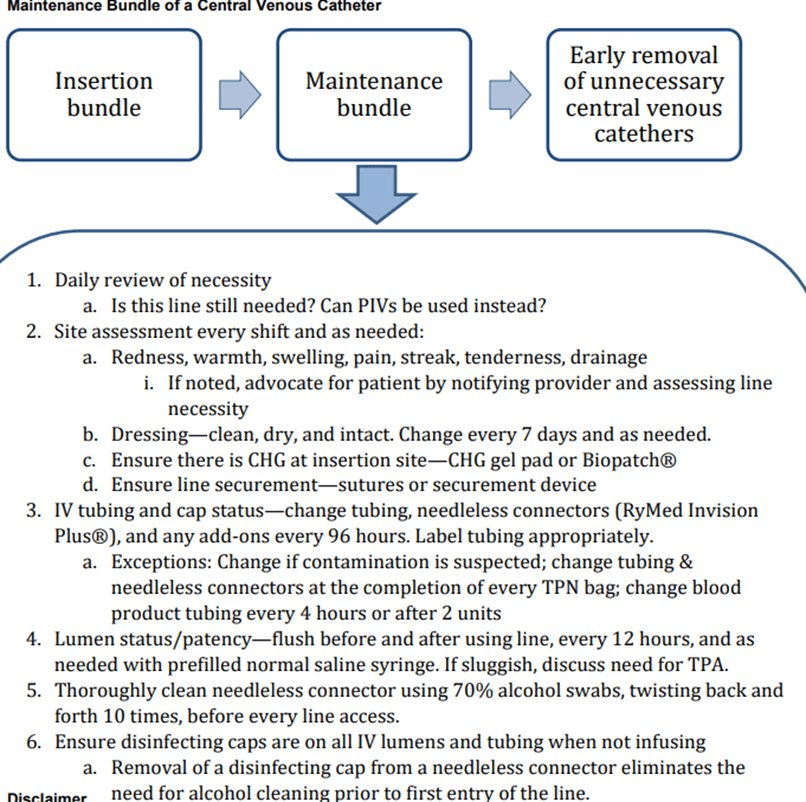
There is a Hospital Policy that includes EBP practices to prevent CLABSIs.
TRUE
The Central Line policy includes a maintenance bundle which discusses EBP to prevent CLABSIs
300
You notice new changes at your patients PICC site. The site is now red and the patient is reporting new tenderness. You should...
Alert the provider and utilize the CL hotline for an individualized plan for the infection control. 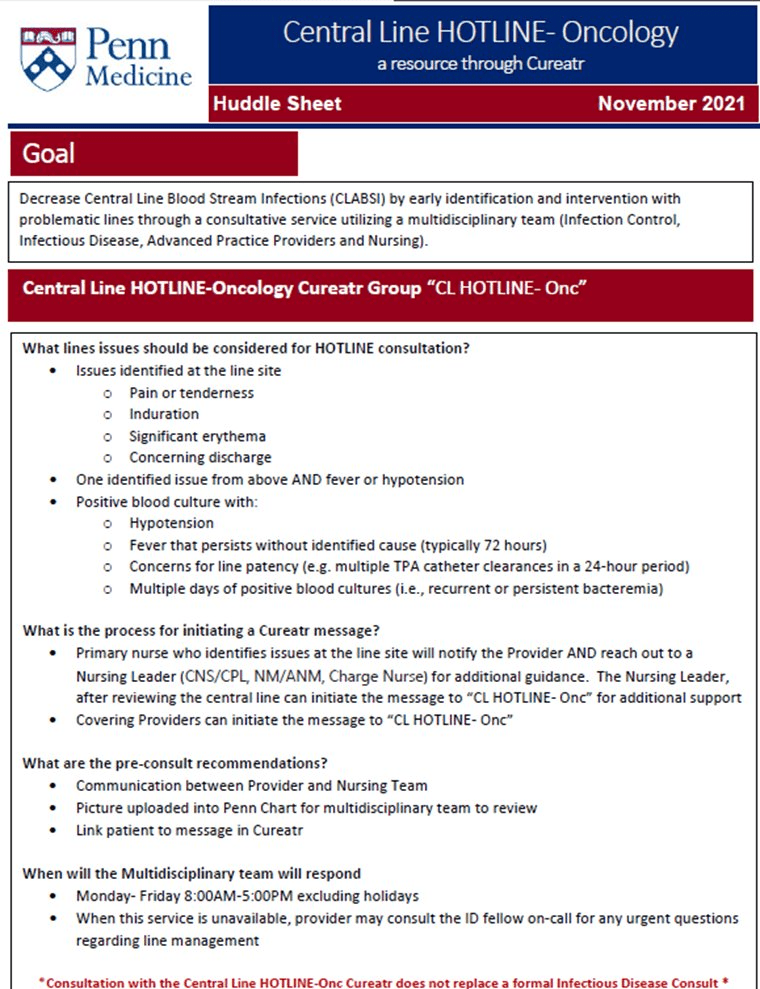
300
What must a nurse document every shift when a patient has an IUC?
-Necessity of IUC
-Maintain a closed IUC seal
-Drainage system maintained below bladder
-Securement device/dressing in place
-Drainage system emptied regularly
-Clean gloves worn when staff or patient touch catheter or bag
-Unobstructed urine flow
-Perform peri-care daily and as needed 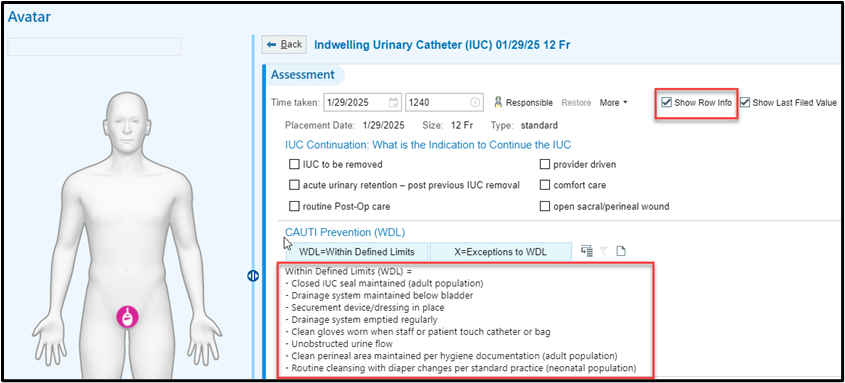
300
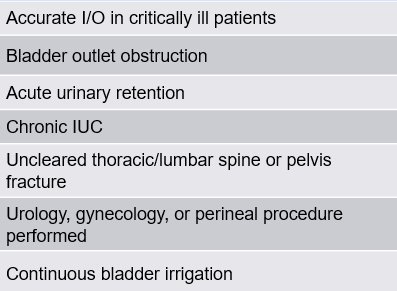
An IUC is the best option for accurate I's and O's.
MYTH
Accurate I's and O's can be measured through other effective ways:
-external urinary catheters (female and male purewick, condom catheter)
-daily weights
300
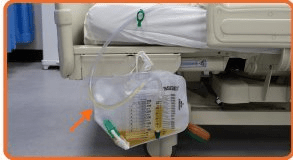
What is the term for a portion of tubing in a urinary drainage system that is positioned in a way that causes urine to accumulate in the tubing, or limit flow from the bladder?
A dependent loop
To maintain unobstructed urine flow, arrange the tubing to ensure proper flow into the drainage bag. Utilize the green sheeting clips to secure the tubing to the sheet
300
What is the only point of care instrument that must be cleaned with bleach?
The glucometer.
-Glucometers should always be cleaned with Sani-Cloth Bleach wipes.
-New docking stations include bleach wipes to ensure the equipment is disinfected properly.
400
My patient has malodorous urine with sediment. These are not indications to send a Urine Culture.
TRUE
400
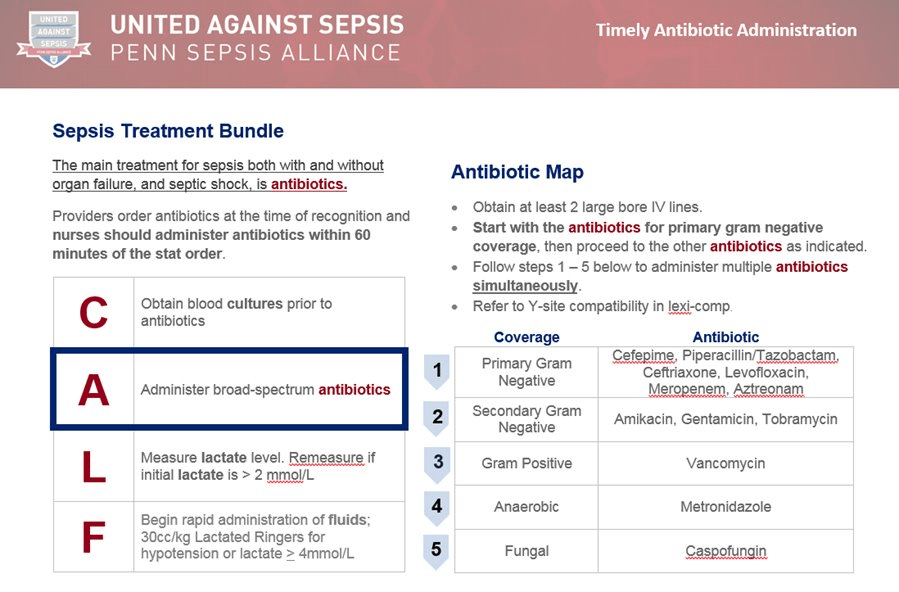
Your patient is ordered IV cefepime and IV vancomycin for their first NTP fever. You have limited access, which medication should be administered first?
IV cefepime
400
What are the IUC indications of Nurse Driven Removal?
-Open Sacral/Perineal Wounds (Stage III/IV)
-Comfort Care
-Routine Post-op Care
-Acute Urinary Retention - Post Previous IUC Removal
400
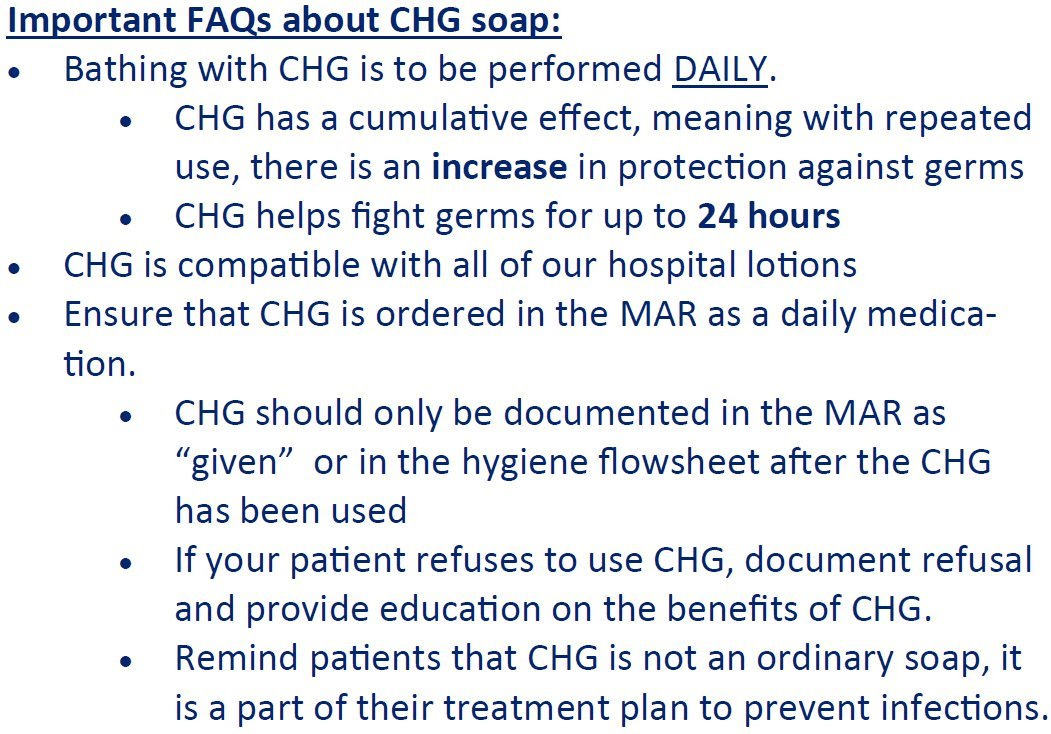
Hibiclens, aka chlorhexidene gluconate (CHG), is most effective if used by patients every day.
FACT
400
Your patient is ordered blood cultures for a NTP fever. You are unable to obtain peripheral cultures, and you just received the IV abx. What are your next steps?
Administer the IV antibiotics! Do not delay the administration of IV antibiotics.
400
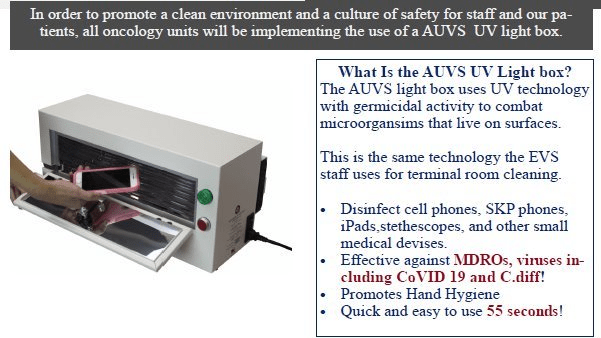
What instrument looks like a toaster oven and can be used to clean your phones and small items?
The Advanced UltraViolet (AUV) disinfection light box.
500
I have a question about my COVID-19 patient's isolation precautions. I can send a Secure Chat to the infection prevention team to clarify any concerns I have.
TRUE
500
What product helps with oozing/bleeding at the CVC site?
Stat Seal

500
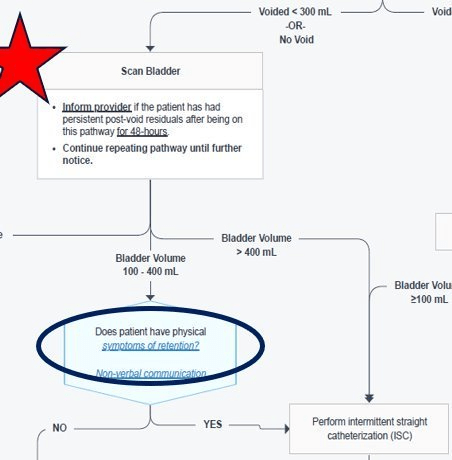
Six hours have passed since your patient's IUC has been removed and the patient has not voided spontaneously. Bladder scans show a volume of 475 mL of urine and patient is complaining of "fullness". You should ____________.
Perform straight catheterization
Bladder Management: Post-indwelling Urinary Catheter (IUC) Removal Management
500
Tubing and the needleless connectors on central line lumens must be changed every 96 hours without exception.
MYTH
500
True or False: Floor RNs have no responsibility for a Hemodialysis catheter
FALSE.
HD Line Care, including dressing changes, is the responsibility of the bedside nurse. Only Dialysis competent nurses may flush or access HD catheter.
500
What equipment is dedicated to the room of a patient with C. difficile?
A Dynamap and disposable stethoscope