Potassium
Cardiology
Sodium
ID
Diabetes
100
Your patient's potassium is 3.0 on AM labs and you want to replace it, what options do you have, and how much should you give?
Potassium Chloride pills (big), Potassium chloride oral solution (tastes bad), potassium chloride IV (takes forever to run, extra fluid, burns)
You should give 40 - 60 mEq.
100
What is the most common cause of acute endocarditis
Staphylococcus aureus.
HACEK group of organisms: Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella.
Prosthetic valve S. epidermidis more common
100
You admit a patient for CAP, what abx regimen do you want to start?
Ceftriaxone + Azithyrmycin OR Doxy
100
What class of medications can cause Euglycemic DKA?
SGLT-2
200
What is the goal glucose level in hospitalized non-ICU patients?
140 - 180
200
Name that rhythm... and treatment!
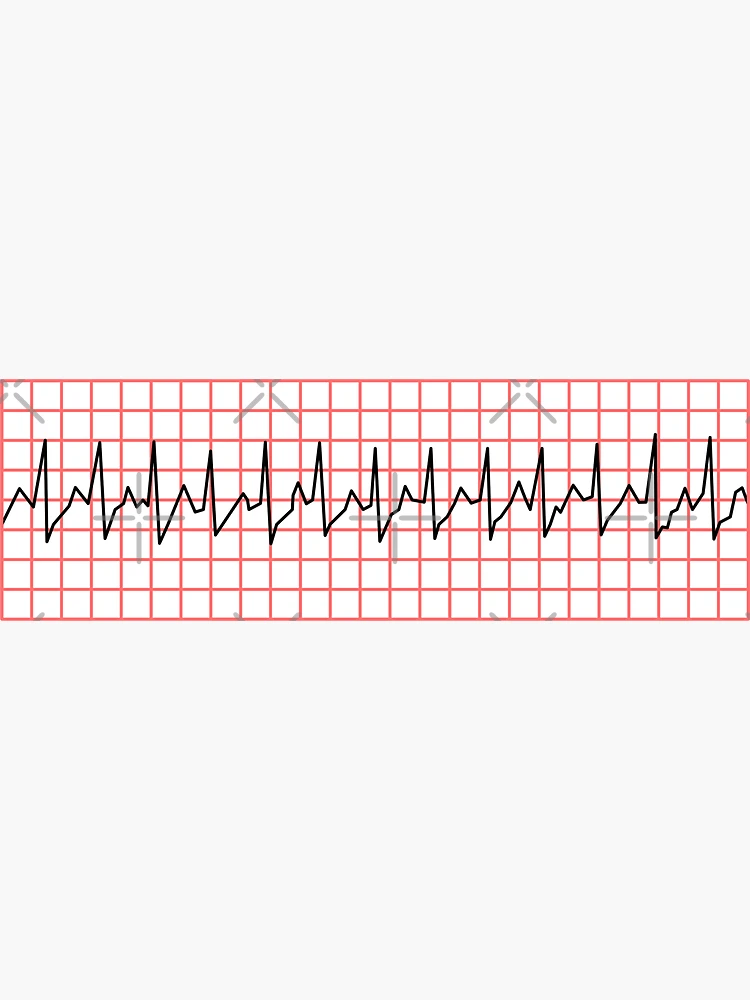
Supraventricular tachycardia (SVT)
- try vagal maneuvers
- Adenosine 6mg -> 12mg
200
Your patient's potassium is 3.0 on AM labs and you want to replace it, what options do you have, and how much should you give?
Potassium Chloride pills (big), Potassium chloride oral solution (tastes bad), potassium chloride IV (takes forever to run, burns)
You should give at least 40 mEq to get their level close to normal range
200
A very common side effect of this medication is a metallic taste. This should also not be taken with alcohol.
Metronidazole?
200
You're working on an admission med rec for a 62 yo female with DM2. Her last A1C was 9.6 five weeks ago. Her home diabetes medications are:
Lantus 60u QHS
Lispro 10u TID AC
Metformin 1000mg BID
Trulicity 3mg qWeek
What would you do with her: Metformin
Hold Metformin
Risk of lactic acidosis when acutely ill. Can restart once stable.
300
You get a call on nights that your patient is hyperkalemic to 6.0. What do you do?
Obtain EKG
Place pt on tele
tx: lokelma, insulin + dextrose, calcium gluconate, lasix
300
You get a page about a floor patient that you're cross covering. 67 yo female here for sepsis, she's complaining of palpitations. Vitals are stable. You get an EKG and it shows the following. What would you like to do?

Afib with RVR
- If stable: IV metoprolol 5mg or Dilt 10-20mg (if no known CHF)
- Not stable: call cards! Amio drip/cardioversion
- Will need TTE, discuss anticoagulation
300
What single agent is the preferred empiric treatment for a cat bite, which can be polymicrobial but can often contain the gram-negative coccobacillus Pasturella multicoda.
Augmentin; Amoxicillin/clavulanate
If penicillin allergy, can use combination therapy with Doxycycline and Metronidazole
If fails orals/needs IV - Unasyn
300
You're working on an admission med rec for a 62 yo female with DM2. Her last A1C was 9.6 five weeks ago. Her home diabetes medications are:
Lantus 60u QHS
Lispro 10u TID AC
Metformin 1000mg BID
Trulicity 3mg qWeek
What would you do with her: Lantus
Decrease home # by ~ 20%
order aprox 48u Lantus, can do less if having poor PO intake or is NPO
400
Your patient has hypothyroidism and takes 100 mcg of Synthroid daily. She is currently NPO due to aspiration risk pending speech eval. What do you do?
- If for a day or two, probably ok to hold med
- IV Synthroid: 1/2 (ish) the PO dose daily
400
Common cause of young person to go into tachydysrhythymia + only having high blood pressure in the hospital or clinic
What is Wolff-Parkinson-White Coat Syndrome
400
A patient is admitted for hyponatremia. List 3 medications/classes of meds that could be causing their low sodium.
Diuretics (mostly thiazides)
Seizure meds: carbamazepine, valproate, lamotrigine
Psych meds: SSRI's, TCA's, Venlafaxine, Antipsychotics
Desmopressin, oxytocin, vasopressin
Opiates, PPI's, Amiodarone, NSAIDs, Linezolid, Illicit drugs (MDMA, ecstasy)
400
Your patient has Staph Aureus bacteremia. What are some things you should do?
Consult ID!
Start antibiotics - Vancomycin until MRSA vs MSSA results
TTE (infective endocarditis)
Repeat cultures
400
You're working on an admission med rec for a 62 yo female with DM2. Her last A1C was 9.6 five weeks ago. Her home diabetes medications are:
Lantus 60u QHS
Lispro 10u TID AC
Metformin 1000mg BID
Trulicity 3mg qWeek
What would you do with her: Trulicity
Hold Trulicity
Typically, with GLP-1's will hold while admitted
500
What are the four pillars of GDMT (and name a medication from each drug class)
What are:
Beta Blockers (Metoprolol succinate, carvedilol, bisoprolol)
ACE/ARB/ARNI
MRA (spiro, eplerenone)
SGLT2 (Dapagliflozin, Empaglaflozin)
500
A patient presenting for dehydration due to diarrheal illness is found to have a Na of 154 on admission.
What is your goal Na over the next 24 hrs and how are you going to get them there?
What are you worried about if you drop it too fast?
- if chronic or unknown timeline goal is to drop Na by no more than 8-10 mmol/L over 24 hrs (0.5 mmol/hr)
- calculate pt's Free water deficit -> best to try PO fluid intake, but if not tolerating, IV fluid resus can be used.
- If you drop the Na too fast your pt can develop Osmotic demyelination syndrome AKA central pontine myelinolysis, this occurs when the myelin sheath around nerve cells in the brain is destroyed. Symptoms include muscle weakness, paralysis, difficulty speaking, and behavioral changes.
500
Vancomycin must be infused slowly to prevent this side effect from occurring.
Bonus - what causes is to happen?
Red man syndrom - Flushing and/or an erythematous rash that affects the face, neck, and upper torso.
It is due to mast cell degranulation.
500
You're working on an admission med rec for a 62 yo female with DM2. Her last A1C was 9.6 five weeks ago. Her home diabetes medications are:
Lantus 60u QHS
Lispro 10u TID AC
Metformin 1000mg BID
Trulicity 3mg qWeek
What would you do with her: Lispro
Consider holding on admission, would favor SSI with meals at first, can adjust based on glucose trends