Neurology
Hem/Onc
Dermatology
Nephrology
100
A 29 yo woman is evaluated before attempting pregnancy. Juvenile myoclonic epilepsy was diagnosed 11 years ago, at which time she started taking valproic acid; she has had no symptoms for 10.5 years. Her only other med is an oral contraceptive agent. She is concerned about taking her medications if she becomes pregnant.
All exam findings are normal, as was her most recent EEG.
A plan is made to discontinue the oral contraceptive, start folic acid, and then taper the valproic acid.
What is the best next step?
What is start Keppra?
100
A 22 yo woman undergoes routine evaluation for chronic anemia, which was diagnosed 6 years ago. Medical history is otherwise unremarkable, but a maternal aunt also has anemia. Her only med is a combination OCP. On exam, vital signs are normal. No hepatosplenomegaly is noted.
Labs:
Hgb 10
MCV 67
Ferritin 200
Iron 150
TIBC 350
Hemoglobin electrophoresis reveals a normal pattern of migration of hemoglobin A and normal levels of hemoglobin A2 and hemoglobin F.
What is the most likely diagnosis?
What is a-Thalassemia trait?
100
A 35 yo man is evaluated after 3 weeks of worsening sinus pain and congestion. He was prescribed amoxicillin-clavulanate. Four days into his treatment, he developed a rash.
On physical examination, vital signs are normal. Skin findings are shown.

There is purulent postnasal drainage noted in the oropharynx. There are no oral, genital, or corneal erosions. There are no findings on the palms, soles, wrists, or ankles. The patient has no skin pain, mouth ulcers, or dysuria. His conjunctivae are injected, but there is no ocular pain.
Labs show peripheral eosinophilia. Other laboratory values, including creatinine, BUN, and liver chemistry tests, are unremarkable.
What is the most likely diagnosis?
What is morbilliform drug reaction?
100
A 70 yo man is evaluated for a recent onset of macroscopic hematuria. History is significant for ESRD and HTN. He has been on HD for 3 years. Urine output is approximately 250 mL/d. Medications are sevelamer, sodium bicarbonate, lisinopril, and amlodipine.
On exam, blood pressure is 150/90 mm Hg, and pulse rate is 70/min. Bilateral flank tenderness is noted. There is no abdominal mass.
Labs show a Hgb 15.
Kidney ultrasound shows several complex cysts and two bilateral solid masses.
What is the most appropriate management?
What is bilateral radical nephrectomy?
200
47 yo woman is evaluated in the hospital for a 4-month h/o increasingly frequent falls and episodes of confusion. She was fired from her job 3 months ago because of poor performance. Since that time, she also has had occasional anxiety, problems sleeping, and visual hallucinations. For the past 2 weeks, she has had repeated falls, exhibited erratic behavior, and been unable to prepare even a cup of coffee.
On exam, vital signs are normal. She is agitated and disoriented to place and time. She exhibits word-finding difficulty and intermittent myoclonic movements of the arms and legs. She scores 8/30 (normal, ≥24) on the Mini–Mental State Examination.
Results of labs are normal, including CSF findings of a normal leukocyte count and normal glucose and protein levels.
An EEG shows periodic sharp wave complexes. Diffusion-weighted brain MRIs show high-signal changes in the basal ganglia and cerebral cortex.
What is the most likely diagnosis?
What is Creutzfeldt-Jakob disease?
200
A 25 yo woman is evaluated in the ED for mild shortness of breath and right lateral chest pain x 2 days. She reports no orthopnea or lower extremity edema. Medical history is unremarkable other than anxiety related to meeting the demands of her new job as an engineer. She takes no medications.
On exam, she is in no apparent distress. Vital signs are normal. Ox sat 99% on room air. Lungs are clear to auscultation. No peripheral edema is noted.
Her Wells Criteria for Pulmonary Embolism score is 0.
A CBC, ECG, and CXR are normal.
What test should be performed next to rule out pulmonary embolism?
What is no further testing?
200
A 36 yo woman is evaluated for a 6-year history of tender, foul-smelling, draining nodules in the inguinal folds. She has had occasional nodules in the axillae. She has taken multiple courses of oral clindamycin with only temporary improvement. She has a 14-pack-year smoking history. Medical history is otherwise unremarkable.
On exam, vital signs are normal. BMI is 34. There are tender nodules, draining sinus tracts, and comedones in the inguinal folds. Scarring is present in right and left axillae. Additional inguinal skin findings are shown.
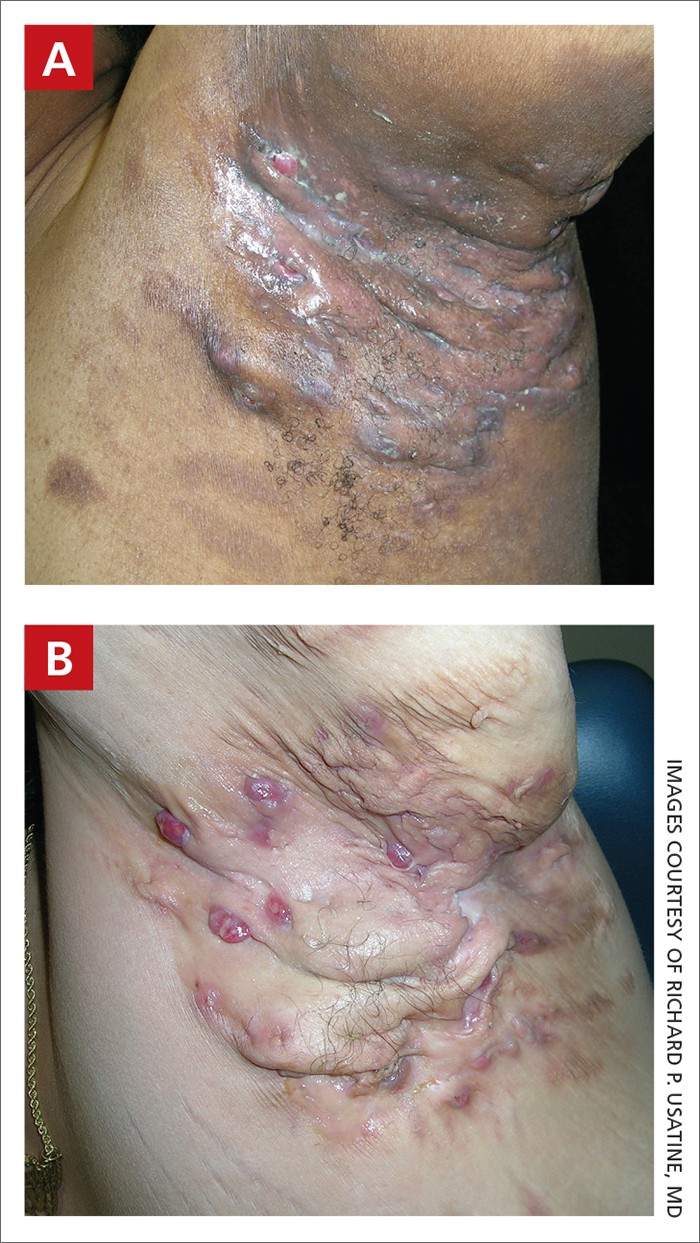
What is the most likely diagnosis?
What is hidrandenitis supperativa?
200
A 48 yo woman is evaluated for edema, dyspnea, and proteinuria. She has a 10-year history of rheumatoid arthritis. She was initially treated with NSAIDs, methotrexate, and prednisone. She stopped taking the NSAIDs 6 months ago because of gastritis. Three months ago she began noticing swelling of her legs, and two weeks ago she began experiencing dyspnea when walking. She has never received penicillamine, gold, or a biologic agent. Current medications are methotrexate, prednisone, and omeprazole.
On exam, the patient appears chronically ill. Temperature is 37.2 °C (99.0 °F), blood pressure is 158/90 mm Hg, pulse rate is 96/min, and respiration rate is 20/min. Jugular venous pressure is elevated. Cardiac examination reveals a summation gallop. The lungs are clear. Swelling and tenderness at the MCP joints and wrists are noted. There is 3+ lower extremity edema to the knees.
Labs:
Albumin 2.8
Creatinine 1.1
Serum protein electrophoresis - Polyclonal gammopathy
UA: pH 5.5, no blood, 4+ protein
Urine protein-creatinine ratio: 6000 mg/g
ECG reveals low voltage, pronounced in the limb leads, but without acute changes.
What is the most likely cause of this pt's proteinuria?
What is AA amyloidosis?
300
51 yo woman is evaluated in the ED for a 1-month history of new-onset abnormal movements, paranoia, hallucinations, and progressive confusion. She was healthy before onset of symptoms and takes no medication.
On exam, vital signs are normal. She is alert but oriented to person and place only, recalls none of three objects after 5 minutes, requires constant redirection to follow commands and sustain attention, is having ongoing visual and auditory hallucinations, and exhibits intermittent slow, writhing (choreiform) movements of the arms. Muscle strength is normal, as are sensation and deep tendon reflexes.
Results of labs, including a CBC and CMP, are unremarkable. Results of brain MRI and lumbar puncture are normal. Subsequent testing for serum anti–N-methyl-D-aspartate receptor antibody is positive.
What is the most likely underlying malignancy?
What is ovarian teratoma?
300
A 22 yo woman is seen for a routine prenatal evaluation; she is 10 weeks pregnant. This is her second pregnancy; the first pregnancy was uncomplicated. Medical history is notable for sickle cell disease requiring 1-2 hospitalizations per year for painful events. She has no history of stroke or acute chest syndrome. Her only medication is a folic acid supplement.
On exam, vital signs are normal. Cardiac examination reveals a grade 2/6 systolic flow murmur. She has a gravid uterus.
Laboratory studies show a hemoglobin 6.4 (baseline 5-7), WBC 11k, platelets 230k.
What is the most appropriate treatment?
What is expectant management?
300
A 44 yo woman is evaluated for painful nodules, ulcers, and skin changes on the lower legs of 2 years' duration. She takes no medications.
On exam, vital signs are normal. Tender subcutaneous nodules, stellate ulcerations, and livido reticularis are evenly distributed bilaterally over her lower legs. The dorsalis pedis and posterior tibial pulses are normal. There are no varicosities present on the legs. The remainder of the exam is normal.
Labs show an ESR 65, Skin biopsy shows vasculitis of a mid-sized arteriole in the subcutaneous. ANCA screen is negative. Antinuclear antibodies titer is 1:40. C3, C4 normal. RF, Hep B/C negative.
Stool is negative for occult blood, and UA is unremarkable.
What is the most likely diagnosis?
What is polyarteritis nodosa?
300
A 55 yo woman is evaluated for increasing serum creatinine and oliguria; she has cirrhosis. She was hospitalized 3 days ago for worsening ascites, confusion, and an elevated creatinine to 1.5 (baseline 1.1). Her diuretics were held, and lactulose was continued. A paracentesis was negative for spontaneous bacterial peritonitis. IV albumin was administered at 1 g/kg/d for 2 days, and today her Cr is 3.0.
Urine output for the previous 24 hours was 300 mL. History is significant for cirrhosis secondary to NASH. Outpatient medications are lactulose, spironolactone, furosemide, and propranolol.
On exam, the patient is confused. She is afebrile, blood pressure is 100/70 mm Hg (stable since admission), pulse rate is 84/min, and respiration rate is 16/min. Asterixis is noted. The skin and sclera are icteric. The jugular venous pressure is normal. Ascites is present. There is 3+ lower extremity edema. The remainder of the examination is normal.
Current Labs: Bicarb 18, Cr 3.0, K 5.0, Na 129, urine Na <10.
Specific gravity 1.025; pH 5.0; trace protein; 2-4 erythrocytes/hpf; 1-3 pigmented granular casts/hpf
Abdominal ultrasound demonstrates ascites, and normal-sized kidneys with no hydronephrosis.
What is the most appropriate treatment?
What is octreotide and midodrine?
400
A 52 yo man is evaluated for a 1 yr history of progressive weakness that began as R foot drop and bilateral tingling in the feet. Within the past 2 months, he has developed progressive weakness, which makes walking difficult; he also notes weakness in the hands and burning below the knees but no autonomic symptoms. He has hypothyroidism treated with levothyroxine.
On exam, vital signs are normal. Motor strength is 4/5 in the intrinsic hand and quadriceps muscles and 3/5 in the tibialis anterior and gastrocnemius muscles; bulbar and facial muscle strength is normal. Deep tendon reflexes are absent in the lower extremities. Sensory perception of vibration is severely impaired at the knees. Pinprick testing shows reduced sensation below the ankles. Splenomegaly is present, as are patchy areas of hyperpigmentation and scattered angiomas on the trunk. Gait is broad based and wobbly, and a Romberg test has positive results.
Serum immunofixation reveals a λ (lambda) light chain monoclonal protein.
Needle electromyography reveals a demyelinating sensorimotor polyneuropathy.
What is the most likely diagnosis?
What is POEMS?
400
A 43 yo man with chronic alcoholic liver disease is hospitalized after massive vomiting of blood. Medical history is notable for alcohol dependence. He takes no medications.
On physical examination, temperature is normal, blood pressure is 102/68 mm Hg, pulse rate is 118/min, and respiration rate is 22/min. He is jaundiced and has spider angiomata on the anterior chest. The liver is palpable but not tender.
Labs:
aPTT 45 seconds
PT 17.8 seconds
Hgb 9.8
Platelet 42,000
Dimer 5200
Fibrinogen 66
He receives volume resuscitation with fluids, erythrocyte and platelet transfusions, and vitamin K.
What should also be provided to manage this patient's coagulopathy?
What is cryoprecipitate?
400
A 52 yo woman is evaluated in the ED for increasing redness, scaling, and itchiness of the skin. Over the last 2 days, it has expanded to cover most of her body. She complains of being cold and shivering. Her skin is flaking so badly she is embarrassed to go out in public. Medical history is significant for psoriasis since childhood and COPD for 5 years. She was treated for a COPD exacerbation last week with 5 days of 40-mg prednisone therapy. Medications are triamcinolone ointment, tiotropium, fluticasone/salmeterol, and albuterol as needed.
On exam, temperature is 37.8 °C (100 °F), blood pressure is 118/70 mm Hg, pulse rate is 100/min, and oxygen saturation 98% on RA.
BMI is 32. The patient is acutely uncomfortable, covered in many blankets and shivering. Her skin is leathery, indurated, and hot to the touch. Skin findings are shown.

There is active bleeding at a few sites where some scale has detached. Nail pitting is present on most of her fingernails. There are no conjunctival, oral, or genital lesions.
What is the most likely cause of the patient's new symptoms?
What is prednisone?
400
A 60 yo woman is evaluated for fatigue and weakness. She reports no nausea or vomiting. History is significant for hypertension, stage 4 CKD, and T2DM. Medications are labetalol, amlodipine, insulin glargine, insulin lispro, and sodium bicarbonate.
On exam, blood pressure is 140/90 mm Hg; other vital signs are normal. A mature radiocephalic arteriovenous fistula (AVF) with a strong thrill and bruit is noted. There are no lung crackles. Trace pedal edema is present.
Laboratory studies show normal serum bicarbonate and potassium levels; BUN 50, and GFR of 18.
What is the next most appropriate management?
What is kidney transplant referral?
500
An 18 yo woman is evaluated for a 2 yr history of repetitive fast movements of the neck that tilt the head to the right side. She reports that these movements are preceded by a feeling of discomfort in the right shoulder and that if she concentrates and taps the right foot immediately after this sensory cue, she usually can avoid the neck movements. She is a senior in high school and says she has not been able to use this method successfully in the classroom, especially during exam, when she often experiences a cluster of movements that exhaust and distract her. Her mother notes that before onset of the neck symptoms, the patient used to roll her eyes and clear her throat frequently. She has OCD treated with sertraline.
On exam, vital signs are normal. During the examination, she displays rapid tilting movements of the head followed by rolling of the head and shoulder; these movements repeat several times in a stereotyped manner. She can suppress these movements on request.
What is the next most appropriate treatment?
What is clonidine?
500
A 35 yo man is evaluated for a 6-month history of night sweats, malaise, and weight loss of 11.3 kg (25 lb). He reports no fevers or other localizing symptoms. His only medication is acetaminophen.
On exam, vital signs are normal. Abdominal examination reveals splenomegaly. The remainder of the examination is noncontributory.
Laboratory studies show a Hgb 12.5, WBC 50k with with 87% neutrophils, 2% myelocytes, 1% metamyelocytes, 0.5% basophils, 7% lymphocytes, and 2.5% monocytes; and a platelet count 424k.
PCR for BCR-ABL fusion gene is positive. A bone marrow biopsy specimen shows hypercellular marrow with myeloid hyperplasia and 1% myeloid blasts.
What is the most appropriate treatment?
What is imatinib (tyrosine kinase inhibitor)?
500
An 18 yo woman is evaluated for a mole on her back that has been changing in color for several weeks. There are no other associated symptoms. She has no significant PMH and takes no medications.
On exam, vital signs are normal. Skin findings are shown.

The remainder of the exam is unremarkable.
What is the most likely diagnosis?
What is a halo nevus?
500
A 65 yo man is evaluated for a 2-month history of low back pain. The pain is worse with movement, but it does not radiate. He reports associated fatigue and a 4.5-kg (10-lb) weight loss. He has osteoarthritis and GERD. He has been taking ibuprofen without any pain relief. His only other medication is omeprazole.
The exam, including vital signs and neurologic examination, is normal.
Labs significant for: Hgb 9.9, Cr 3.0, UA with trace protein; no blood, erythrocytes, leukocytes, leukocyte esterase, or nitrites; urine protein-creatinine 2000 mg/g.
Ultrasound reveals normal-sized kidneys with slightly increased echogenicity; no hydronephrosis or abnormalities of the collecting system are seen.
In addition to discontinuing ibuprofen, what is the most appropriate next step in management?
What is urine protein electrophoresis?