Gastroenterology
General IM
Pulm/CC
ID
100
A 65 yo woman is evaluated for watery, nonbloody diarrhea x 8 months. She reports up to 6 BMs/day with nocturnal awakenings, but no abdominal pain, bloating, flatulence, or weight loss. Her last screening colonoscopy at age 60 years was normal. She has no personal or family history of colon cancer or polyps. She also has osteoarthritis. Only medication is ibuprofen 3x/week. Not exposed to children and no recent travel or engagement in outdoor recreational activities.
On exam, vital signs are normal. The remainder of the physical examination, including abdominal examination, is normal.
Laboratory studies show hemoglobin, serum albumin, total IgA, and tissue transglutaminase IgA levels to be within normal limits.
What is the most likely cause of this patient's diarrhea?
What is microscopic colitis?
100
A 23 yo woman is evaluated for depression as she prepares for discharge from the hospital to home hospice care. She was diagnosed with metastatic ovarian cancer 2 years ago, and she progressed through four lines of chemotherapy, a trial of immunotherapy, and a failed attempt at a phase 1 clinical trial. Her life expectancy is measured in weeks. She is currently hospitalized with volume depletion, and after consultation with her oncologist and palliative care team, she has decided to be discharged home with hospice care.
On exam, the patient exhibits substantial fatigue and poor concentration. She has a flat affect except when intermittently tearful. Previously upbeat despite all of the setbacks, she is now withdrawn and describes feeling hopeless. She has pervasive guilt over the burden she believes she has caused her family. Medications are a fentanyl patch, oxycodone, ondansetron, polyethylene glycol, senna, and zolpidem.
What is the most appropriate treatment?
What is methylphenidate?
100
A 37 yo man is evaluated for a 1-month history of worsening cough and wheezing requiring use of rescue therapy several times per week, as well as increasing nasal congestion and rhinorrhea. He has a history of moderate persistent asthma and rhinitis since his early twenties. One month ago the patient underwent repair of a traumatic anterior cruciate ligament tear and has some residual daily knee pain. His medical history is notable for sinusitis. He has no symptoms of gastroesophageal reflux disease. Medications are albuterol, budesonide/formoterol, and ibuprofen.
On physical examination, vital signs are normal. Pulse ox is 97% on room air.
Examination demonstrates conjunctival injection and nasal polyps in both nostrils. Chest examination reveals wheezing on expiration. The remainder of the examination is noncontributory.
Laboratory studies reveal IgE 265 (elevated), CBC 4000 with 10% eosinophils. Office spirometry demonstrates moderate airflow obstruction
What is the most appropriate initial management?
What is stop ibuprofen and start prednisone?
100
A 66 yo woman is evaluated in the ED with a 2-day history of fever and nonbloody diarrhea occurring several times a day. She recently completed a 10-day course of cephalexin for cellulitis of the leg.
On physical examination, temperature is 39.0 °C (102.2 °F), blood pressure is 98/60 mm Hg, pulse rate is 110/min, and respiration rate is 23/min. She appears uncomfortable but is not confused. Her abdomen is distended and bowel sounds are decreased. She has tenderness and abdominal guarding to palpation. Cellulitis has resolved.
Labs significant for:
WBC 30,000 with 80% neut, 15% bands
Albumin 2.5
Cr 2.5
Lactate 2.8
Stool polymerase chain reaction assay is positive for Clostridium difficile toxin gene. Abdominal imaging reveals evidence of toxic megacolon.
The patient is admitted to the ICU, and a surgical consultation is requested.
What is the most appropriate antibiotic treatment?
What is oral vancomycin and IV metronidazole?
200
A 78 yo man is evaluated in the ED for worsening jaundice of 2 weeks' duration, dry mouth, dark urine, and light stools. He has also noticed swelling under his jaw bilaterally. He reports no abdominal pain or weight loss.
On exam, vital signs are normal. Swollen submandibular glands bilaterally and jaundice are noted.
Alk phos 180
ALT 66
AST 55
Tbili 6.2
Dbili 4.8
CT abdomen shows a narrowed pancreatic duct and enlargement of the pancreas parenchyma, described as a “sausage-shaped” pancreas, as well as findings consistent with retroperitoneal fibrosis. Endoscopic ultrasound–guided biopsy of the pancreas shows more than 10 IgG4-positive cells/hpf and no evidence of malignancy.
What is the most appropriate treatment?
What is prednisone?
200
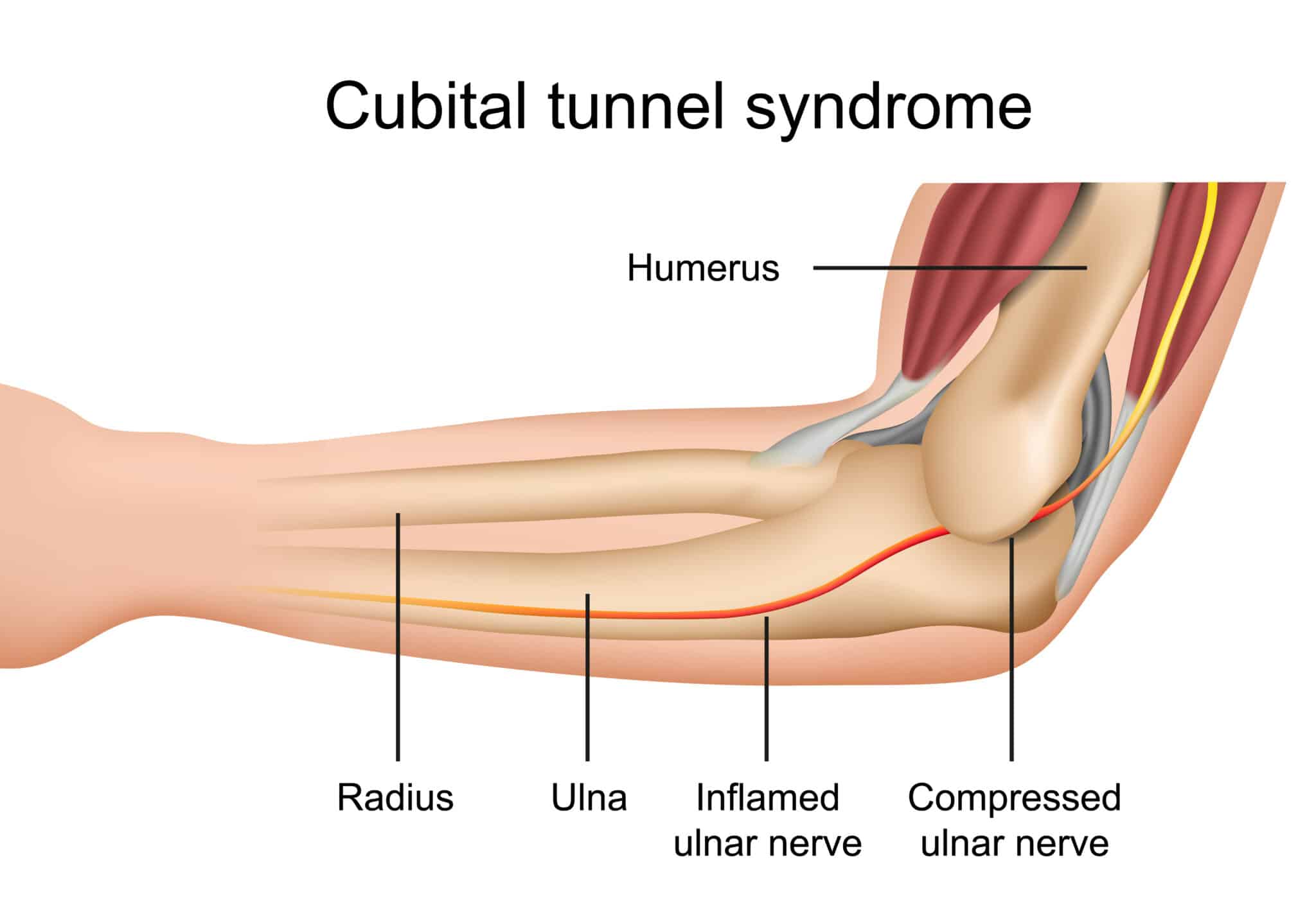
A 44-year-old man is evaluated for right medial elbow pain that began 2 months ago with a dull ache and has gradually worsened. The pain is worse with elbow flexion, and his right fourth and fifth fingers are numb.
On physical examination, vital signs are normal. Decreased sensation over the volar aspect of the right fourth and fifth fingers is noted, with adduction and abduction weakness of the fingers. The right elbow has full range of motion and no notable erythema, swelling, or tenderness.
What is the most likely diagnosis?
What is ulnar nerve entrapment?
200
A 32 yo man is evaluated in the hospital for symptoms of persistent asthma. He was evaluated in the emergency department 2 days ago for dyspnea accompanied by wheezing, dysphonia, and upper chest and throat tightness. Symptoms persisted despite use of albuterol inhaler every 3 to 4 hours and intravenous methylprednisolone, and he was hospitalized. He was diagnosed with asthma in high school and generally requires several courses of prednisone per year. Current medications are albuterol and fluticasone/salmeterol inhalers, prednisone, and montelukast.
On exam, BP is 130/85 mm Hg, pulse rate is 110/min, and respiration rate is 18/min. Pulse ox 100% on 2L.
BMI is 25. Chest examination demonstrates monophonic wheezing on inspiration.
Labs including CBC, metabolic panel, and IgE is normal. CXR is unremarkable and bedside spirometry is normal.
What is the most appropriate next step?
What is laryngoscopy?

200
A 25 yo woman is evaluated for chronic intermittent nonbloody diarrhea with associated abdominal cramping, burping, and bloating. Symptoms began several months ago. She has a history of selective IgA deficiency with recurrent sinopulmonary infections. She has not taken antibiotics in the past 6 months.
On physical examination, temperature is 37.3 °C (99.1 °F); the vital signs are otherwise normal. On abdominal examination, bowel sounds are present with minimal diffuse tenderness to palpation.
Stool testing for occult blood is negative.
Which of the following is the most likely cause of this patient's diarrheal illness?
What is Giardia lamblia?
300
A 65 yo man is evaluated after a screening ultrasound for abdominal aortic aneurysm showed incidental gallbladder findings. He reports no symptoms. He continues to smoke cigarettes, 1 pack per day. He has no other medical problems and takes no medications.
On exam, vital signs are normal, as is the remainder of the examination.
Labs, including a complete blood count and alkaline phosphatase, ALT, AST, and total bilirubin levels, are within normal limits.
The abdominal US shows numerous layering gallstones and an immobile 8-mm gallbladder polyp.
What is the most appropriate next step?
What is cholecystectomy?
300
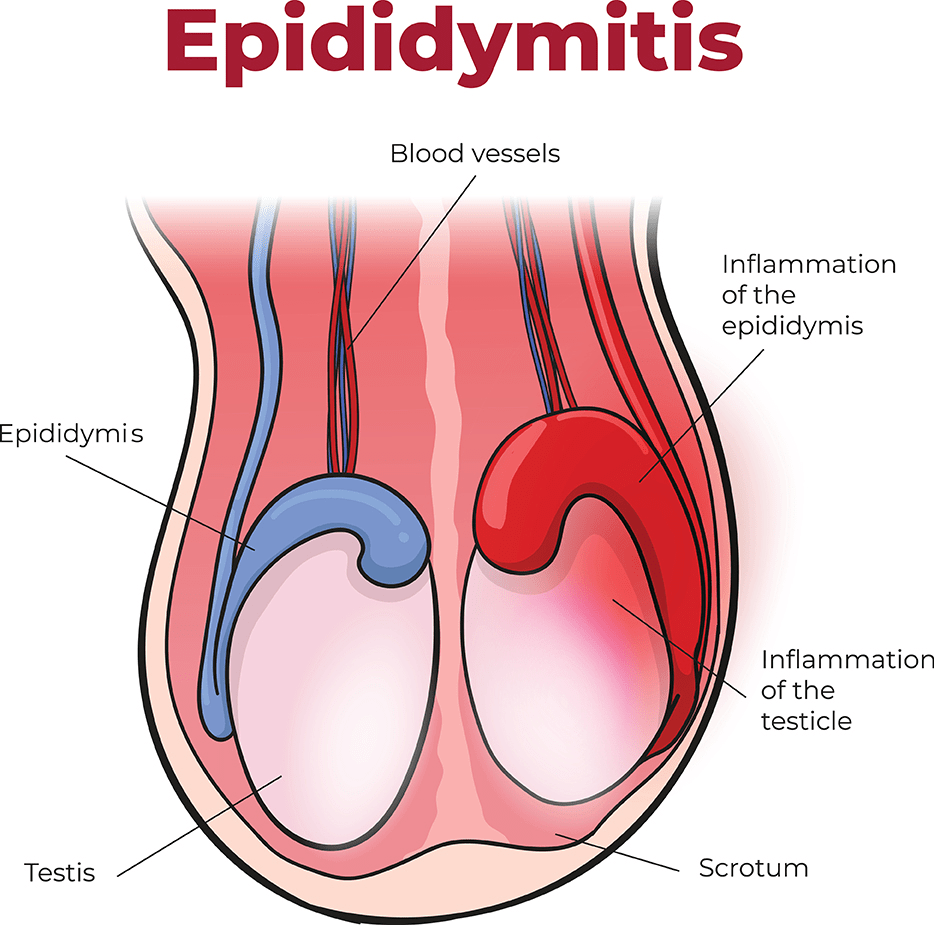
A 29 yo man is evaluated in an urgent care center for a 2-day history of pain and swelling of the right hemiscrotum. The pain is stable in intensity, neither worsening nor improving. Other symptoms include low-grade fever and dysuria. He reports no abdominal pain, nausea, or vomiting.
On exam, temperature is 38.3 °C, and pulse rate is 103/min. BP and respiration rate are normal. There are erythema and swelling of the right hemiscrotum and moderate tenderness to palpation of the superolateral aspect of the right hemiscrotum. The hemiscrotum is not elevated, and there is no scrotal mass, rash, or penile discharge.
What is the most likely diagnosis?
What is epididymitis?
300
A 67 yo man is evaluated in the ED with a 3-day history of weakness and nausea and a 2-week history of difficulty swallowing. He has lost 22.7 kg (50 lb) during the past year. He has no other symptoms. History is significant for a 30-pack-year history of smoking. He quit smoking 4 years ago. He takes no medications.
On exam, vital signs are normal. Lung examination reveals decreased tactile fremitus above the lower portion of the right lung as well as dullness to percussion and decreased breath sounds. His neurologic examination is normal.
Lab showed Na 127 but otherwise normal.
What is the most likely diagnosis?
What is small cell lung cancer?
300
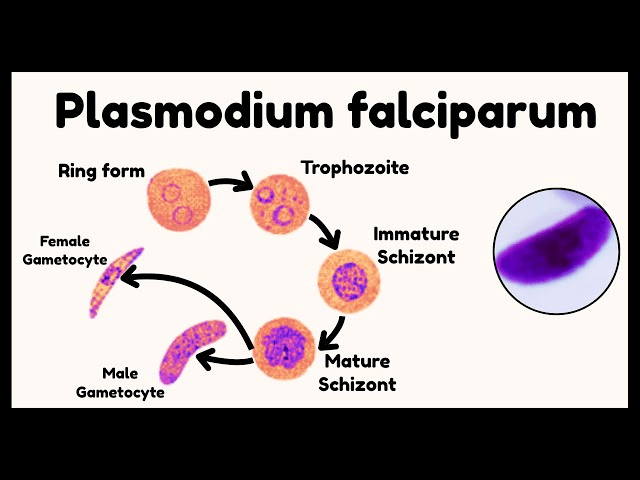
A 27-year-old woman is hospitalized with a 5-day history of intermittent fever, headache, muscle pains, and abdominal cramps. She returned 8 days ago from a 1-week trip to Kenya and Tanzania. She spent time outdoors in the evening and went hiking in a wooded park. She is pregnant at 20 weeks' gestation. She declined pretravel immunizations as well as antimalarial chemoprophylaxis. Her only medication is a prenatal vitamin.
On physical examination, temperature is 39.1 °C (102.3 °F), blood pressure is 98/64 mm Hg, pulse rate is 112/min, and respiration rate is 16/min. Her conjunctivae are icteric. Cardiopulmonary examination reveals regular tachycardia. The remainder of the examination is unremarkable.
A peripheral blood smear is shown.
What is the most likely causative agent?
What is Plasmodium falciparum malaria?
400
A 43 yo man is evaluated for 4 days of fever and arthralgia, as well as a raised purple rash over his lower extremities x 1 week. He is a current IV drug user. He has no other medical problems and takes no medications.
On exam, temperature is 37.8 °C (100 °F) and blood pressure is 132/85 mm Hg; other vital signs are normal. The large and small joints are tender to palpation without evidence of synovitis. The abdomen is not tender to palpation. The liver edge is palpable below the right costal margin. The skin findings are shown.

AST 130 Hep B surface antigen +
ALT 142. Hep B e antigen +
Tbili 2.5. Hep B surface antibody +
Cr 1.0. Hep B DNA 10 million
Hep C, HIV negative
Crypoglobulin normal
What is the most appropriate treatment?
What is Entecavir or tenofovir?
400
A 68 yo woman is evaluated for a 6-month history of incontinence typified by continuous leakage and dribbling. She reports no back pain, dysuria, or fever. Medical history is significant for a 30-year h/o T2DM and a 10-year history of HTN and HPLD. Medications include benazepril, metformin, and rosuvastatin.
On exam, BP is 147/76 mm Hg, and pulse rate is 92/min. On abdominal examination, the bladder is palpable just above the pubic symphysis. Foot examination demonstrates dry feet, loss of sensation to monofilament testing, and vibration up to the ankles. Lower extremity tendon reflexes are absent.
Urinalysis results are normal.
What is the most appropriate diagnostic test?
What is post-void residual?
400
A 60-year-old woman is evaluated during a follow-up visit. She has a lifelong history of intermittent asthma previously provoked by exertion and exposure to cold air. During the past 2 years her symptoms have progressed, and she now has dyspnea after walking one block or going up any incline. COPD was diagnosed 4 days ago after spirometry revealed an FEV1 of 65% which was only partial reversible with albuterol.
She has no history of acute exacerbations. She has recently discontinued cigarette smoking. She currently takes albuterol as needed.
On exam, vital signs are normal; pulse ox normal.
Lungs are clear to auscultation.
Laboratory studies reveal normal hemoglobin and leukocyte count with 8% eosinophils. CXR was clear.
What is the most appropriate treatment?
What is inhaled corticosteroid and long acting beta agonist?
400
A 67 yo man is evaluated for a chronic, nonhealing ulcer on his left foot x 3 months. He was at a local sauna when he sustained an abrasion to the bottom of his foot after stepping on a sharp object. He subsequently developed an ulcer at the site of the injury and received several courses of antibiotics, including trimethoprim-sulfamethoxazole, doxycycline, and cephalexin, with no improvement. The ulcer continues to expand in size and deepen. Medical history is notable for hypertension and a 40-pack-year smoking history. His only medication is hydrochlorothiazide.
On exam, the vital signs are normal except for a temperature of 37.3 °C (99.2 °F). The legs and feet are without edema or discoloration. Pedal and popliteal pulses are symmetrical and intact. Lower extremity sensation is intact. He has a 2- × 2-cm ulcerated lesion on the plantar aspect of the metatarsal region of the great toe, with surrounding erythema, yellowish discharge, and firm edges.
What is the most likely cause of the ulcer?
What is Mycobacterium fortuitum?
500
A 28 yo woman is evaluated at 28 weeks' gestation. This is her first pregnancy. She has chronic hepatitis B virus infection acquired through vertical transmission. The patient reports feeling well. Her only medication is a prenatal vitamin.
On exam, vital signs are normal. The uterus is enlarged, consistent with 28-week intrauterine gestation. No stigmata of chronic liver disease are noted.
Labs are positive for hepatitis B surface antigen and hepatitis B e antigen. The HBV DNA level is 300,000 IU/mL. The results of other studies, including alanine aminotransferase, aspartate aminotransferase, and total bilirubin levels, are within normal limits.
What is the most appropriate next step?
What is tenofovir?
500
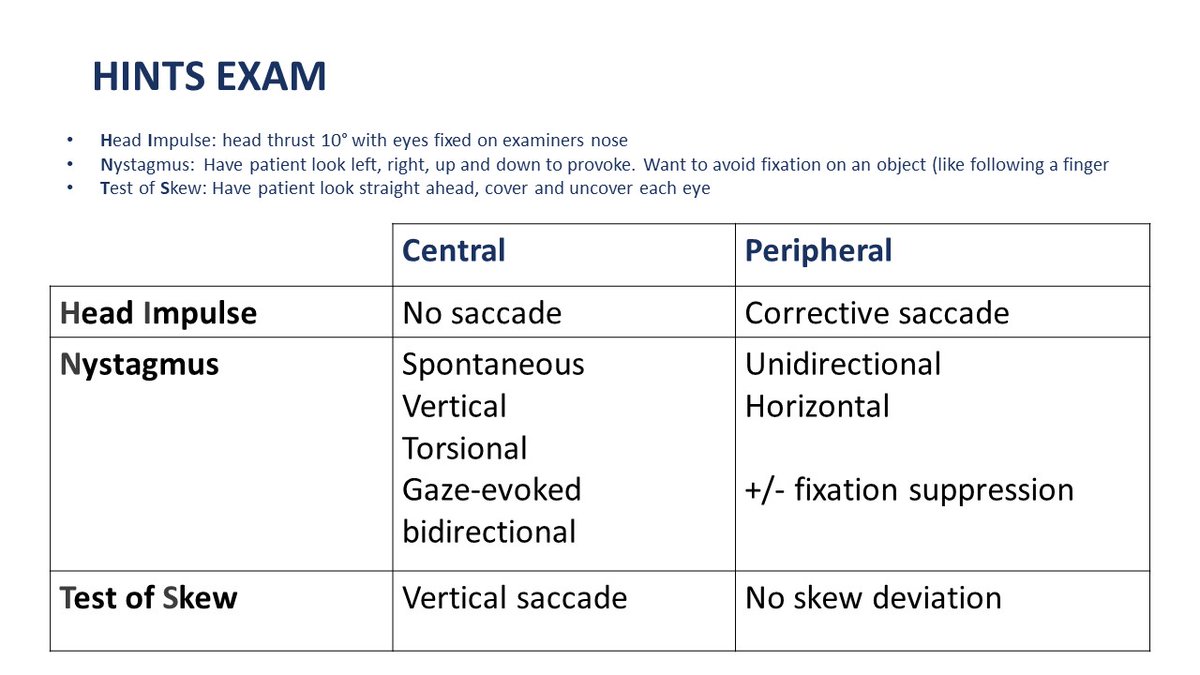
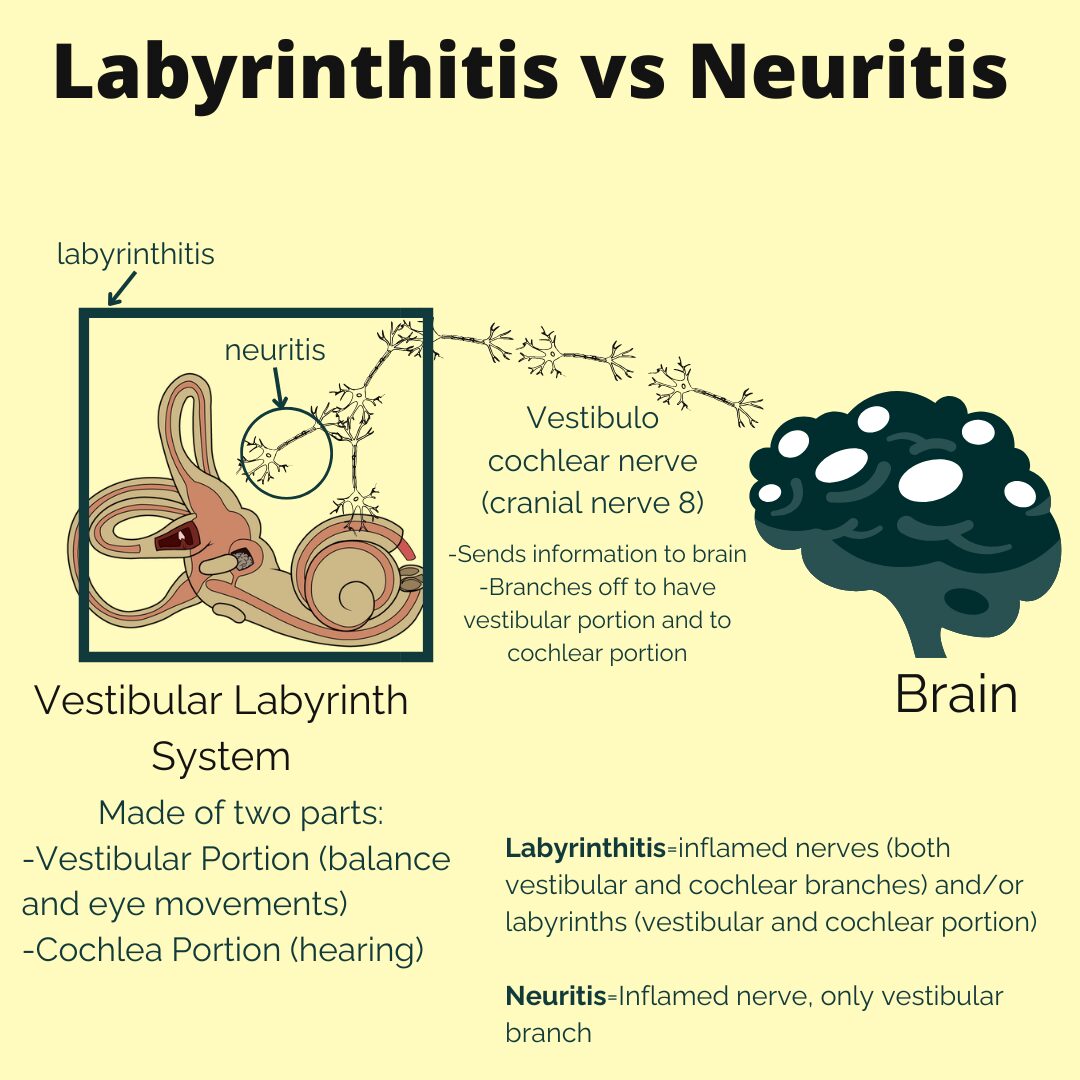
A 55 yo man is evaluated in the ED for a 2-day history of dizziness accompanied by nausea and vomiting. He works as an electrician, and his symptoms started suddenly while installing an overhead light fixture with his head tilted back for a prolonged period. He describes the dizziness as a constant whirling sensation that is unaffected by changes in position. He also reports symptoms of a recent upper respiratory tract infection but no fever. He has no other medical problems and takes no medications.
On exam, temperature is normal, blood pressure is 155/84 mm Hg, pulse rate is 99/min, and respiration rate is normal. Hearing is diminished on the left side. Spontaneous combined horizontal and torsional nystagmus is noted but lessens with a fixed gaze. The patient declines further examination because of severe nausea.
What is the most likely diagnosis?
What is labyrinthitis?
500
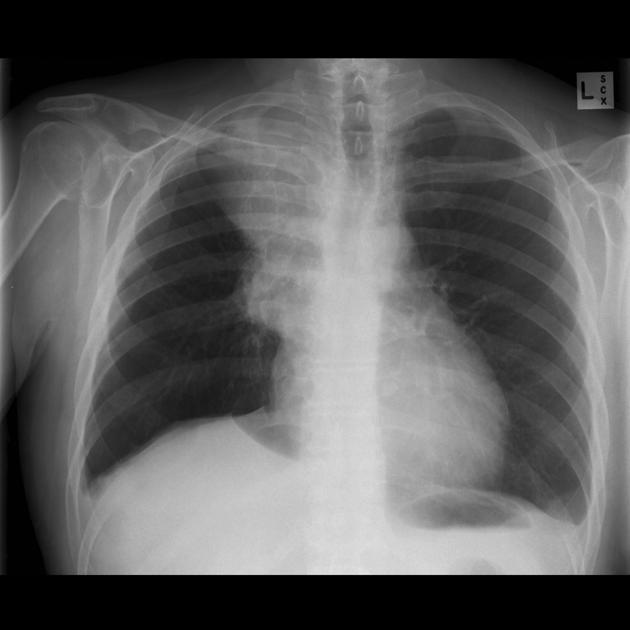
A 49 yo man is evaluated for a 4-month history of cough, chest pressure, and double vision. He has no fever, night sweats, or weight loss. He has never smoked.
On exam, vital signs are normal. There is ptosis bilaterally. The remainder of the physical examination is normal.
A CT scan of the chest is shown.
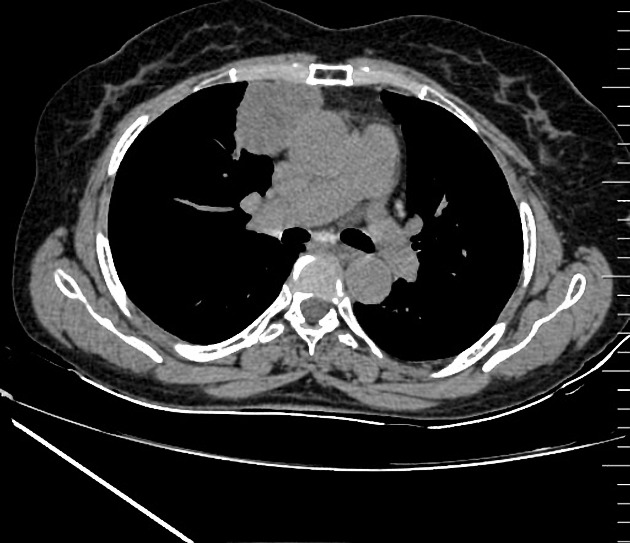
What is the most appropriate next test to perform?
What is an acetylcholine receptor (AChR) antibody test?
500
A 19 yo woman is evaluated in the ED for a 2-day history of fever, headaches, and jaundice. She vacationed in Hawaii 1 month ago and reports swimming in lakes and rivers. She was diagnosed with a flu-like illness 2 weeks ago that resolved spontaneously. No history of a rash. She is sexually active with one partner. She takes no medications other than an oral contraceptive.
On exam, she is alert and oriented. Temperature is 38.9 °C (102 °F), blood pressure is 92/60 mm Hg, pulse rate is 124/min, and respiration rate is 24/min. Generalized lymphadenopathy, conjunctival suffusion, and scleral icterus are noted. She has photophobia, and passive neck flexion elicits resistance and discomfort. The remainder of the examination is unremarkable.
Labs significant for:
Tbili 5.6
Cr 2.6
CSF: WBC 176, glucose 72, protein 78
Cerebrospinal fluid Gram stain is negative and culture results are pending
What is the most likely cause?
What is leptospirosis?
